
Abstract
The aims of this study were to: (i) Determine if there were significant bone mineral density and muscle strength differences between intact and amputated limbs, and (ii) investigate the possible relationship between local bone loss and muscle strength in transtibial amputees. Fifteen male veterans with traumatic unilateral transtibial amputations who ranged in age from 18–45 years were included in this prospective study. Lower limb muscle strength was measured with an isokinetic dynamometer. Dual energy X-ray absorptiometry was used to determine bone mineral density of the femur and tibia. The bone mineral density values of the femur and tibia were found significantly decreased on the amputated side. Significant decreases (p < 0.001) in strength of the quadriceps and hamstrings were observed in the amputated limb. There was a weak correlation between quadriceps strength and total femur bone mineral density (p = 0.048, r = 0.518) on the amputated limb. Transtibial amputees are prone to bone mineral loss and muscle strength decrease on the amputated side. Our results also indicate that muscle strength itself might not be of decisive importance for bone mass in transtibial amputees.
Introduction
Lower extremity amputation is associated with significant changes in body composition such as muscle atrophy and weakness in the thigh muscles and decreased local bone mineral density (BMD). 1–6 Muscular atrophy and weakness is due to disuse or underuse, and mainly related to reduction of the muscle fibre size. 7 Atrophy and strength of the thigh muscles in TT amputees have been investigated by several authors. In their ultrasonographic study, Schmalz et al. reported the atrophy at the amputated extremity compared with the sound limb. 8 Atrophy or hypotrophy following amputation, caused by underuse 9 , mainly at the cost of reduction of fibre size, and occurs not only in the amputated side but globally. 10
In transtibial (TT) amputees, caused by loss of proprioceptive feedback, principally from the ankle joint and relative structures, residual limb is less active in walking or standing activities. 4,5 On the other hand, gait of TT amputees is asymmetrical, with more time spent on the support phase of the non-amputated limb (and consequent overload of this limb) 11 and the metabolic cost of ambulation in amputated subjects is near the upper physiological range found in the normal population. 7,12 Therefore TT amputees are under the risk of reduction of physical activity and muscle strength. Previous studies which compared isokinetic strength between the thigh muscles of the amputated versus the sound limb, finally showed a significant higher strength in the non-amputated side. 4–7,13 This dramatically strength deficit in the amputated limb occurs in the first years after amputation. 5,7
BMD is determined mainly by genetic factors, while nutrition, physical activity, muscle strength, and body composition contribute to a varying extent throughout life. 14 Regional significant bone loss on femur and tibia is an inevitable consequence in patients with lower limb amputations. 1 The aetiology of bone loss is uncertain but it is likely to be a local phenomenon in lower limb amputees. Altered gait pattern, decreased weight load, disuse atrophy and lack of muscular action at the limb seem to be important causal factors in the development of both local and generalized osteoporosis. 1–3
In the able-bodied population, mechanical loading and exercise are important factors to increase or protect BMD. However; it was shown that standing activities and exercises can not prevent bone loss in spinal cord injured patients. 15 The amputee patients are a similar population because of decreased weight load and changed muscle configuration. During the amputation surgery insertions of muscles are changed to non-physiological sites and marked atrophy occurs. 16
Local muscle strength and muscle contractions are important factors for local BMD and these factors need to be paid more attention in amputee patients. We hypothesize that BMD and muscle strength is lower in amputated side than in sound side and local bone loss is related to the loss of muscle strength in transtibial amputees.
Methods
This is a prospective cohort study of patients who had suffered from land-mine injuries. The study was approved by our institutional local ethics committee, and informed written consent was obtained from each participant. Fifteen healthy male veterans with traumatic unilateral TT amputations who ranged from 18–45 years in age were included in this study. Patients who were younger than 18 and older than 45 years of age and patients with aetiologies other than land-mine injury were not included in the study. Patients with a known metabolic disease that may affect the bone metabolism also led to exclusion.
Bone mineral density
Dual energy X-ray absorptiometry (DEXA/LUNAR DPX®) was used to determine bone mineral density (BMD) of the femur/hip (total, neck, Ward's triangle) and tibia/knee at the amputated and the non-amputated limbs. For bilateral hip and proximal tibia scans, subjects lay in a supine position. When the femoral neck was scanned, the leg was rotated internally and abducted slightly. Before starting the proximal tibia scan, knee was placed in approximately 5° of flexion and lower limb was slightly rotated internally. Then the laser crosshair was positioned 10 cm distal to the superior border of the patella and preceded proximally 11 cm. The tibia was positioned such that the shaft appeared vertically straight and that the epiphysis was centered on the imaging screen.
Isokinetic assessment
Lower limb muscle strength was measured by Cybex Norm isokinetic dynamometer (Lumex, Ronkonkoma, NY, USA). Hip and knee extensor and flexor muscle groups of the patients were tested at 30 and 120°/sec angular velocities of the amputated and non-amputated sides. Peak torque (Nm) was recorded for each muscle at each velocity.
For each patient the test procedures complied with reproducibility criteria (i.e., axes of movement, subject positioning, positioning of proximal joints, attachments and stabilizing straps, and practice test in concentric mode). The subject was placed on the seat with the hip at an angle of 90° of flexion. The subjects were strapped to the chair at the chest, pelvis and thigh. Additional stabilization and support at the heel was provided to the prosthesis in order to minimize relative movement between the residual limb and socket. 4 The subject was attached in position after adjustment of the depth of the seat, the height of the dynamometer, and the length of the support lever, allowing the axis of rotation of the dynamometer to be aligned with a prolonged virtual rotation axis of the knee, as determined by a line passing through the femoral condules.
Examination protocol started with a warm-up, which was performed on cycle ergometer with a low resistance setting (<600 rpm) for 5 min. The warm-up continued using the dynamometer with 6–10 submaximal and 2–3 maximal flexion-extension concentric contractures. After 2-min resting period, patients were asked to perform 5 flexion-extension concentric exercises at 30°/sec and at 120°/sec. All patients were allowed a 2-min rest period between tests on the same joint and a 5-min resting period between tests on each side.
Statistical analysis
All analyses were carried out using SPSS 10.0 for Windows. The BMD value and muscle strength differences between sound and amputated limbs were evaluated by Wilcoxon Signed test. Spearman correlation analyses were performed to evaluate the hip/knee muscle strength and local BMD values in sound and amputated sides. Results were considered statistically significant at the <0.05 level.
Results
Of the 15 men who were participated in this study, eight (53.3%) were right-sided and seven (46.7%) were left-sided TT amputees. All had amputations because of a land-mine injury. Mean age at the time of study was 26.2 ± 3.9 (range: 21–34) years and the mean duration of amputation was 57.9 ± 43.5 (range: 6–160, median: 52) months. All of the patients were wearing their prostheses, which were endoskeletal types with patellar tendon bearing sockets, more than five h a day and none of them was using any ambulatory aids. All patients reported that they had an educational course about isometric and endurance exercises for residual limb and their exercise frequency was at least 2–3 days in a week.
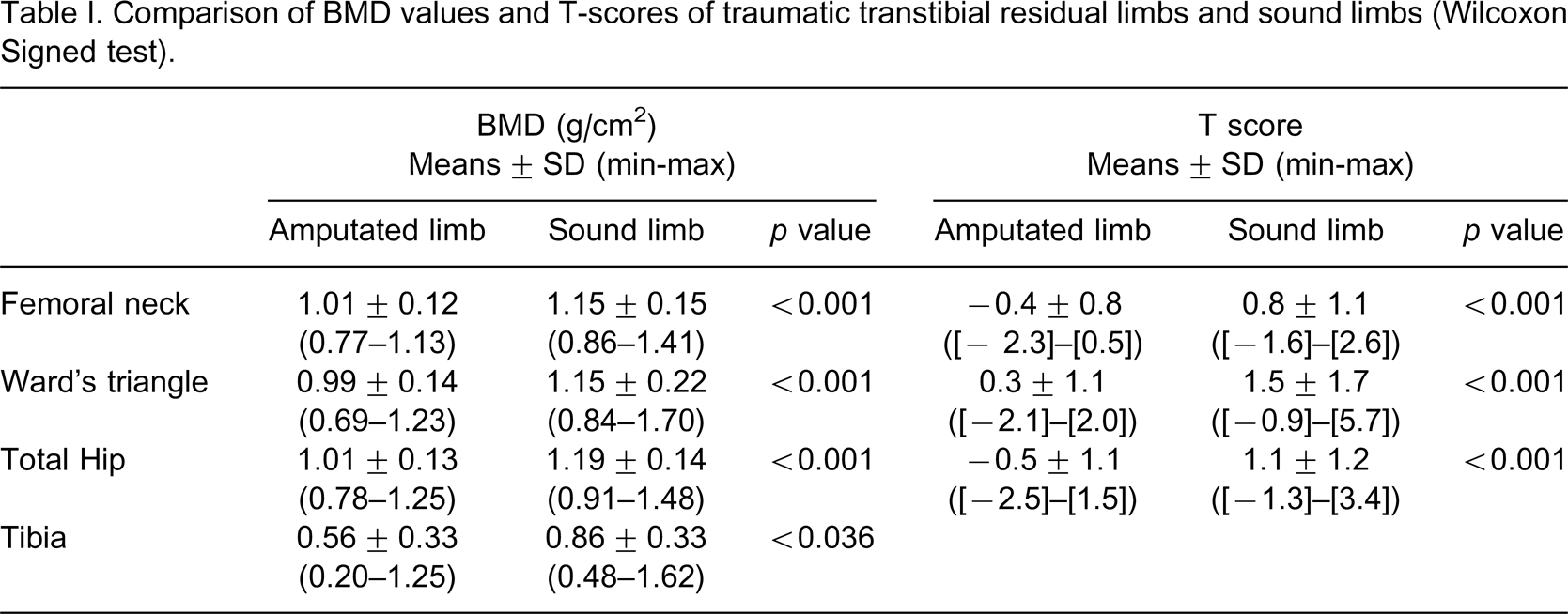
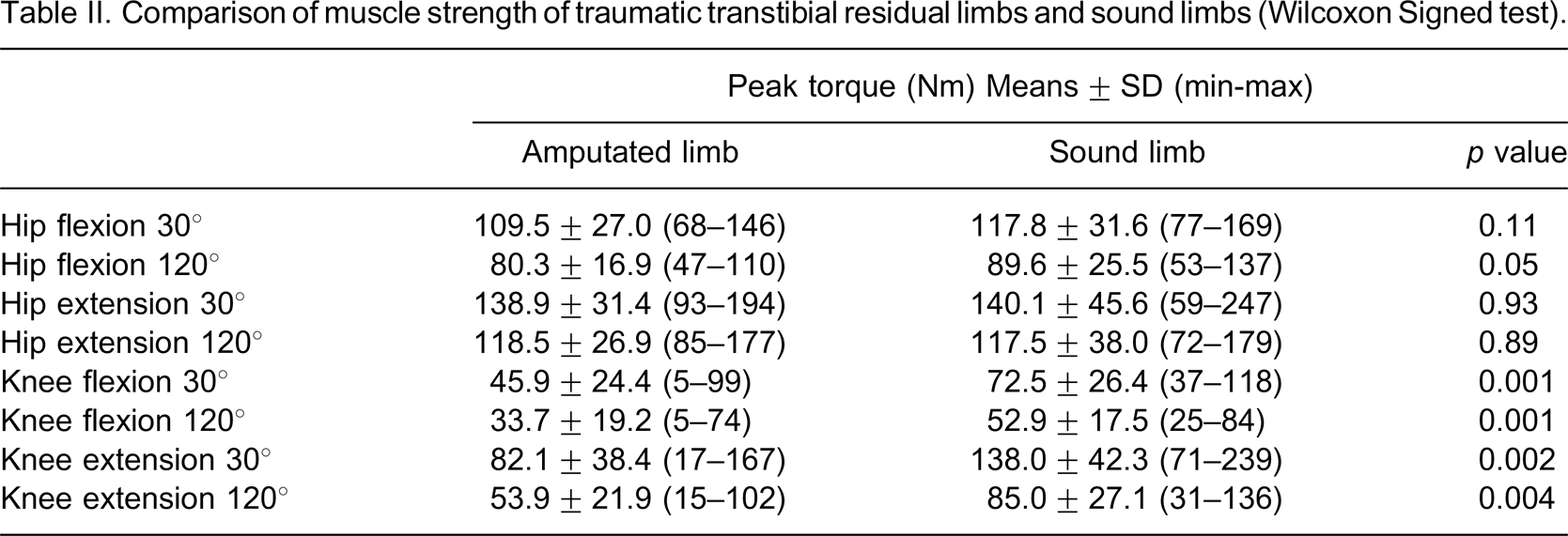
The BMD values of the femoral neck, Ward's triangle, total femur and tibia on the amputated side were significantly lower than the non-amputated side (Table I). Significant decreases (p < 0.001) in strength of the quadriceps and hamstrings were observed in the amputated limb (Table II). There were no significant differences (p ≥ 0.05) in hip flexor/extensor muscle strength between the amputee and intact sides (Table II).
Comparison of BMD values and T-scores of traumatic transtibial residual limbs and sound limbs (Wilcoxon Signed test).
Comparison of muscle strength of traumatic transtibial residual limbs and sound limbs (Wilcoxon Signed test).
In the amputee side, we only found a statistically significant correlation between quadriceps muscle strength and total femur BMD (r = 0.518, p = 0.048) (Table III). In the intact side we found significant correlations between hip muscle strengths and BMD in the proximal tibia (p < 0.001) (Table IV). However, there were no consistent correlation between hip muscle strengths and BMD in the proximal femur (femoral neck, Ward's triangle and total femur BMD values). There were only two significant correlations (between quadriceps strength and BMD values in the femoral neck (r = 0.59, p = 0.02) and Ward's triangle (r = 0.66, p = 0.007) (Table IV).
Spearman correlation analyses for hip/knee muscle strength and local BMD values in amputee side.
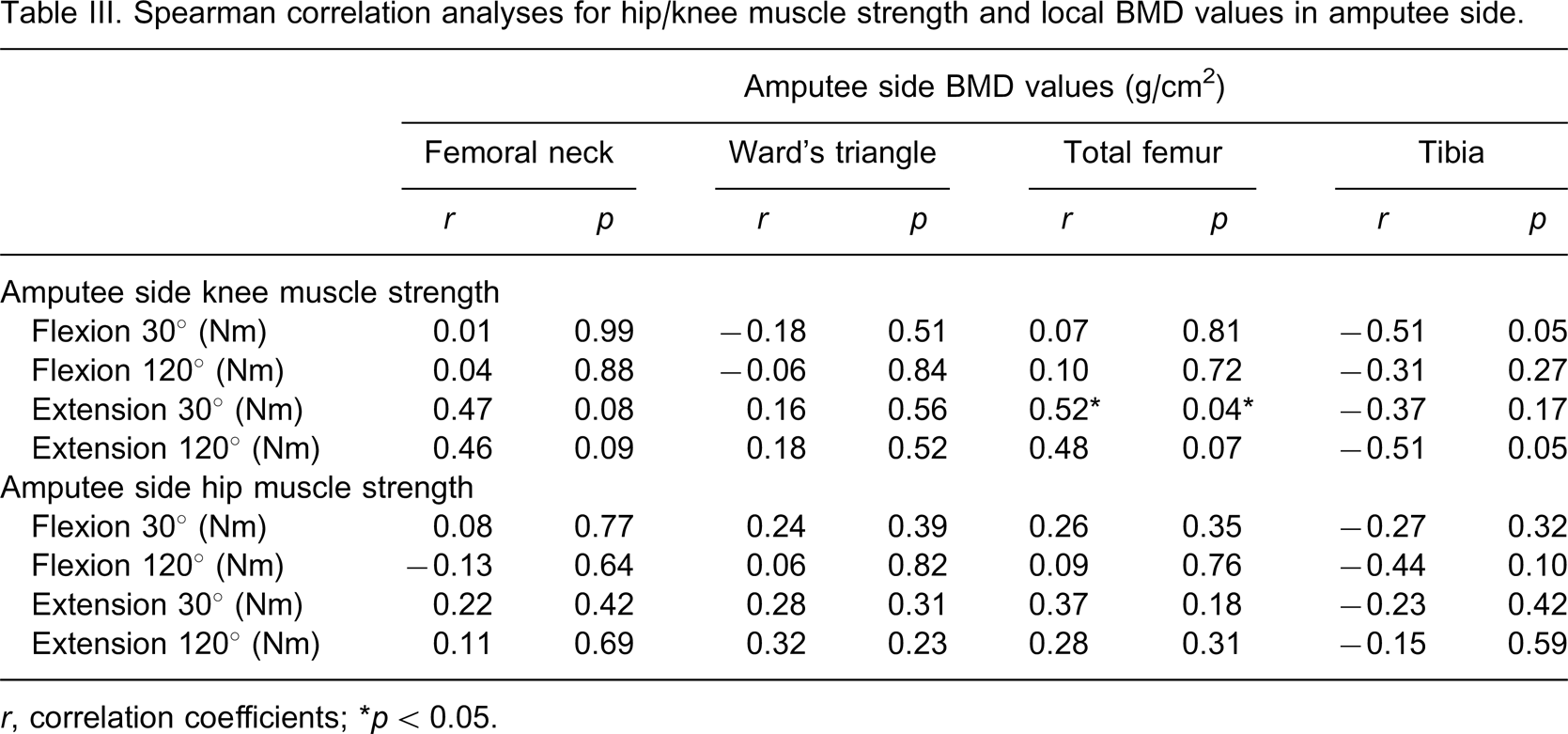
r, correlation coefficients; ∗p < 0.05.
Spearman correlation analyses for hip/knee muscle strength and local BMD values in intact side.
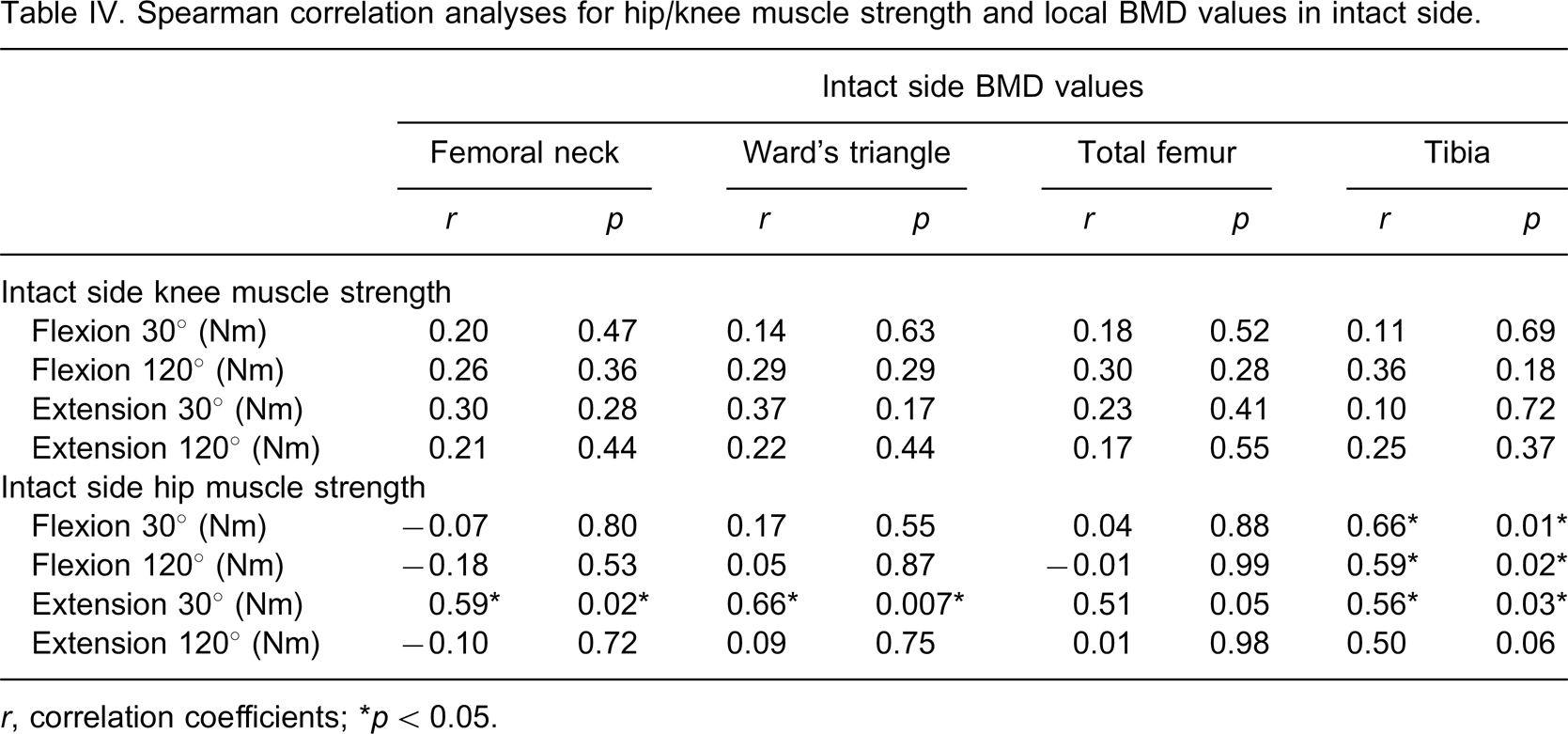
r, correlation coefficients; ∗p < 0.05.
Discussion
The present study showed that there were bone loss in femur and tibia and decreased muscle strength at the quadriceps and hamstring muscles on the amputated side in traumatic young unilateral TT amputees. In addition to these findings, this study also showed a significant correlation between hip muscle strength and BMD in the femoral neck, Ward's triangle and tibia of in the intact side; whereas no correlation was seen between muscle strength and BMD, except weak relationship between quadriceps strength and total femur BMD in the amputated side.
In recent study, Yazicioglu et al. demonstrated that the BMD values of proximal femur and proximal tibia on the amputated side were significantly lower from the non-amputated side in the unilateral traumatic TT amputees. 1 In such previous studies, similar BMD differences were observed between the femoral region of the amputee and sound limbs. 2,3 BMD is determined mainly by physical activity, muscle strength, genetic factors, nutrition, and body composition. 14 Specifically, the two most important forces acting on the bones are muscle contractions and gravitational forces which have an osteogenic effect on the skeleton. Bone adapts its remodelling and functional structure depending on the daily pattern of these forces. 17 Herein, it would be noteworthy to mention that we did not consider some of the aforementioned factors in our study because our study population consisted of young, healthy males without any known systemic/metabolic illnesses. Furthermore, the subjects were physically active with their prosthesis in their daily lives.
In the TT amputated patients, caused by loss of proprioceptive feedback, principally from the ankle joint and relative structures, residual limb is less active in walking or in standing activities. Also, in TT amputees, body-weight bypasses the proximal tibia, loads directly into the prosthesis and down to the ground by the way of patellar tendon. According to this decreased or lack of loading effect on the tibia, we supposed that bone mass associated with only muscle strength in the tibia. Gait of TT amputees is asymmetrical and their energy requirement during ambulation is increased according to normal population. It is now widely accepted that physical activity is beneficial to BMD. Therefore TT amputees are under the risk of reduction of physical activity and bone loss.
The main aim of this study was to investigate the relationship between bone density and muscle strength in the TT amputees. To our knowledge, correlation between bone mass and muscle strength in TT amputee patients has not been investigated before. Several studies have also demonstrated a site-specific relationship between muscle strength and adjacent BMD sites in healthy and non-amputated subjects.
Bevier et al. found that isometric back strength correlated with spine density 18 and Madsen et al. found that quadriceps strength was a significant predictor of the proximal tibia in women. 19 Nordström et al. demonstrated a site-specific relationship between BMD of the tuberositas tibia and quadriceps strength in adolescent boys with low activity. 20 Some of previous studies have been suggested that the skeletal and muscular systems are structurally interdependent and both adapt to mechanical loading. In this manner the muscular action provides a stimulus for bone remodelling by muscle pull at the site of attachment of the tendon into the bone, and that the skeleton adapts to the increased magnitude of loading by depositing bone. 16,21–24
Although some reports (mentioned above) have documented positive correlations between muscle strength and bone mass, other authors stated that the effect of muscle strength is systemic and found no link between muscle strength and bone mineral content. 25–31 Sinaki et al. found that back extensor strength correlated with bone mineral density of the hip however, there was no significant correlation between the strength of the spinal flexor or extensor muscles and the site-related bone mass (lumbar spine). 27 Similarly, Pocock et al. showed that strength of the biceps was a better predictor of hip BMD than strength of the quadriceps. 25 Madsen et al. assessed the relationship of quadriceps strength to site-specific BMD of the tibia and to BMD of the forearm. This study provided support for regional relationship between quadriceps strength and both BMD of the proximal tibia and a distant muscle group. 30
Furthermore, some authors emphasized that the relationship between muscle strength and BMD is generally more pronounced among sedentary individuals and those with low to moderate levels of physical training whereas little or no relationship is seen among highly trained individuals. 32,33 In addition, Ribom et al. reported that muscle strength was associated with BMD in women, but not in men. 14 These reports are consistent with our results that there is a weak relationship between local BMD and muscle strength on the intact side. The relationship in the amputated side was not studied before.
In conclusion, our findings imply that muscle strength itself does not seem to be of significant importance for BMD and also indicate that muscle strength itself might not be of decisive importance for bone mass in the TT amputees.
Footnotes
Acknowledgements