
Abstract
The ankle-foot orthosis (AFO) with oil damper, GaitSolution (GS), was previously developed to make heel rocker function possible during the gait of hemiplegic patients. To clarify the characteristics of patients who show adaptation to GS use, a questionnaire was completed by the clinicians responsible for 99 patients with hemiplegia who participated in this study. Clinicians completed items concerning gait data of patients without AFO use and with GS use, adaptation to the use of GS, and patient opinion of GS use. Approximately 60% of patients achieved heel rocker function during the loading response of the paretic limb and improved gait when using GS. A comparison of the patients whose gaits were improved by GS more than by other AFOs revealed the use of GS was well suited to the gait of patients with a relatively higher Brunnstrom stage and a slightly flexed knee joint during the stance phase. Approximately 60% of patients reported feeling comfortable using GS, although patient comfort did not necessarily coincide with the results of gait assessment by clinicians. Patient comfort mainly depended on trunk posture and hip joint outward rotation; hip joint outward rotation could be improved using GS in the recovery phase but not in the maintenance phase. This result implies the importance of gait training in the early stage of rehabilitation.
Introduction
The use of ankle-foot orthoses (AFOs) has been widely shown to improve the gait of hemiplegic patients 1 and AFOs can be categorized into two groups: Non-articulated AFO (NAAFO) and articulated AFO (AAFO). The use of NAAFOs are reported to increase gait velocity, decrease double stance duration, improve the symmetry ratio of stance duration and of deceleration force, increase step length of the paretic limb, decrease body sway in stance, normalize heel strike, improve control of inversion of the foot, and improve activities of the hamstrings and calf muscles. 2–9 The use of AAFOs has shown improvement of gait velocity, cadence, stride length, single stance duration of the paretic limb, and dorsiflexion angle of the paretic ankle joint during stance. 10–13 Comparing the two kinds of AFOs, Weis et al. reported that NNAFOs impeded the natural movement of the ankle joint in stance and shortened the step length, resulting in slower velocity. 13 Gok et al. reported a metallic AFO to be superior to a plastic AFO in terms of stabilization of the ankle, allowing improved heel strike and push-off. 14 The results of these numerous studies were based on instrumented gait analysis, and the effectiveness of AFOs in the improvement of gait is generally accepted. However, there has as yet been insufficient investigation of the effects of different kinds of AFOs on hemiplegic gaits, and only a limited number of studies have examined patient opinion regarding the use of AFOs. deWit et al. reported that 70% of patients felt more self-confident while wearing an NAAFO, 6 and Tyson and Thornton reported that 96% (24/25) of patients found gait comfortable when using an AAFO. 12 However, the relationship between patient opinion and gait improvement when using AFOs remains to be examined in detail.
It is widely accepted clinically that the gait of hemiplegic patients is improved by the use of AFOs. To improve the gait of individual patients, orthotists and therapists must select appropriate AFOs. Their decisions are usually based on observational gait analysis, and rarely on the results obtained from using instrumented gait analysis systems, for example, employing 3D motion capture and force plates. Therefore, it is important for clinicians to understand the specifics of gait improvement when carrying out observational gait analysis. Moreover, it is also important that they understand the factors affecting patient comfort during gait.
Conventional AFOs are used to prevent foot drop during the swing phase, to maintain lateral stability of the ankle during stance, and to optimize the position and stability of the knee by adjusting the position of the ankle joint of the AFO. Previous studies involving gait analysis of more than 100 hemiplegic patients have identified the desirable functions of AFOs. 15,16 The most important function of the AFO is to assist eccentric contraction of the dorsiflexors during the loading response of the paretic limb, which resists the abrupt plantar flexion of the ankle joint from heel contact to foot flat, making the heel rocker function possible. 17 The magnitude of resistance must be adapted to each patient's condition. To realize these functions, an AFO with oil damper called GaitSolution (GS) was previously developed. 18 The oil damper generates the resistive force to plantar flexion and the magnitude of the resistance can be changed easily. We have shown by gait analysis the gait improvements of hemiplegic patients using GS. 19
Due to the limited number of patients undergoing gait analysis, the prescription guidelines for GS have not yet been clarified. To resolve this problem, we undertook the monitoring of GS usage among a large number of patients, in cooperation with 34 facilities in Japan. 20,21 A questionnaire including items concerning patient demographics, gait data, and adaptation of the patient to wearing GS was completed by the clinicians of participating patients. Gait data was taken from the observational gait analysis by clinicians, with the exception of walking time and number of steps taken for a 10-m walk test. Patient opinion of GS use was also examined.
The purpose of this study was to answer the following questions:
What are the characteristics of patients whose gait is improved by GS? Which gait parameters affect adaptation to GS use? What happens when patients feel that their gait is comfortable when using GS? Does gait improvement coincide with patient opinion?
Method
A total 88 GSs were fabricated by Kawamura-Gishi Co. Ltd, Japan: 12 sets of plastic GS (each set consisting of six GSs, with three sizes each for the right and left) and four sets of metallic GS (each set consisting of four GSs, with two sizes each for the right and left) (Figure 1).

The GaitSolution AFO (left) metallic type; (right) plastic type.
The functions of both GSs were the same. As mentioned above, GS generates the resistive force when the ankle joint moves to plantar flexion, and the magnitude of the resistive force and the initial ankle joint angle can be changed easily. The resistive force assists the eccentric contraction of the dorsiflexors to make the heel rocker function possible during the loading response of the paretic limb. The alteration of the resistance and the initial ankle joint angle are achieved according to manufacturer's instructions. The aims of making such alteration is to establish smooth plantar flexion of the ankle and slight flexion of the knee during the loading response of the paretic limb so as to prevent foot drop during the swing phase, and to achieve the most comfortable gait for each patient. The ankle joint of GS allows for free dorsiflexion movement to 30°, and GS has a contouring footbed.
GS sets were lent for three months each to 34 participating facilities (30 hospitals, three orthotic manufacturers, and one nursing home) who responded to a public appeal for participation, and patient usage was monitored and the questionnaire then completed. The selection criterion of participants for this study was a hemiplegic patient who uses an AFO daily or who is willing to use an AFO. Other conditions including the duration of GS use differed depending on the facility. The monitored use of GS started in January 2004 and finished in May 2005. We asked clinicians responsible for each patient to complete the questionnaire.
The questionnaire was designed to clarify the patient demographics and the difference in gait without an AFO and with GS. It was revised eight times during a preliminary survey administered among a small group of clinicians. Patient demographic data was collected via 21 items, such as age, gender, cause of hemiplegia, Brunnstrom stage for the lower extremities, ROM, spasticity (Modified Ashworth Scale (MAS), 22 and independence. These data were recorded before GS usage. Questionnaire items regarding detailed gait parameters when walking without an AFO and with GS included initial contact, knee joint angle, outward rotation of the hip, trunk upright posture, ankle joint angle during swing phase, and toe off. (see question A in the Appendix for details). These gait parameters were chosen because they were found to be important for assessing the gait of hemiplegic patients in previous studies. 18,19 Arm movements were not taken into account because most of the patients used assistive devices when walking.
Items concerning heel rocker function and improvement of gait using GS were included. We defined adaptation to GS function as a positive response to both of these questions, “Could you recognize ankle plantar flexion from initial contact to foot flat, which is the function of GS?” and “Did the patient's gait improve when using GS compared to when using his or her own AFO?” since this indicated the patient achieved heel rocker function using GS, thereby improving gait. See questions B and C in the Appendix for details. In question C, the definition of improvement depended on the individual clinician's assessment through observational gait analysis since, in clinical practice, gait is assessed by clinicians. In addition, duration and number of steps taken on the 10-m walk test when walking without an AFO and with GS were recorded; in both conditions the patients were permitted to use walking assistive devices if necessary. The patient's subjective opinion about using GS was also recorded on a four-point scale; see question D in the Appendix.
Results
We appealed to the public for participation in this study. As a result, 34 faculties responded. We explained the purpose and study design and asked clinicians in each faculty to decide if they are able to participate in this study according to their ethical regulations. If they accepted, we started the study. Prior to GS usage, the purpose and the study design were explained to the patients and written informed consent was obtained by clinicians who were responsible for each patient.
Basic data collected
The questionnaire was answered by 104 participants: 94 physical therapists, four medical doctors, four others, and two whose role was not recorded. Based on the fact that the recovery curve of stroke patients rises to plateau at around six months post-onset, 23 we categorized patients into one of the following two groups: In the recovery phase within 180 days post-onset (n = 55) or in the maintenance phase after 181 days post-onset (n = 44). Five patients were excluded from the analysis because the time of stroke onset was not reported. Thus, data was analyzed for a total of 99 patients.
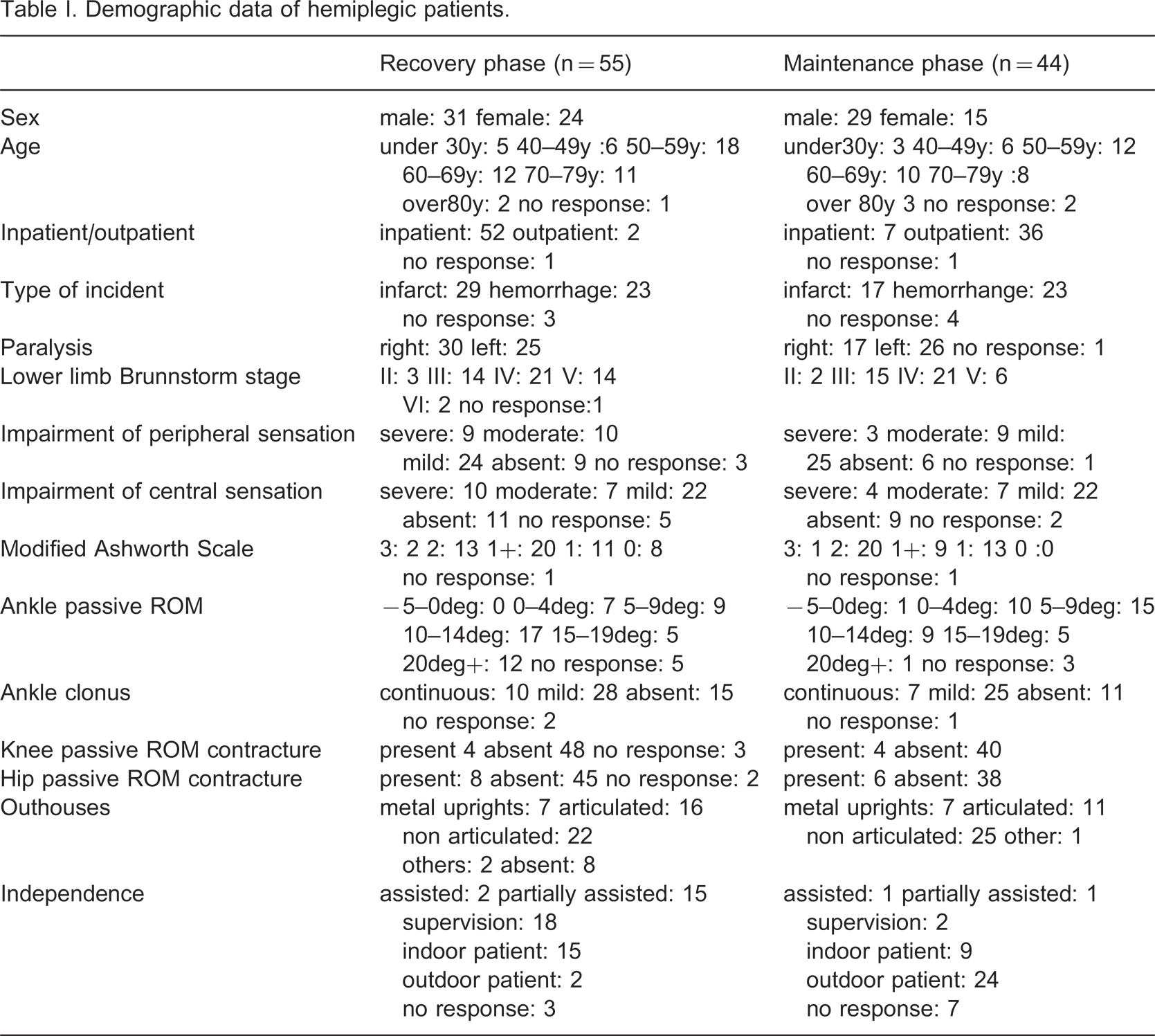
Patient demographics are shown in Table I. No large differences were observed between patients in the recovery phase and maintenance phase except in terms of in- or outpatient status, spasticity (MAS), ankle joint passive ROM, and independence. The duration of GS use varied, ranging from one hour to more than 60 days, but was longer for patients in the recovery phase due to their inpatient status.
Demographic data of hemiplegic patients.
Walking time and number of steps taken on 10-m walk test when not using an ankle-foot orthosis (AFO) and when using GaitSolution (GS).
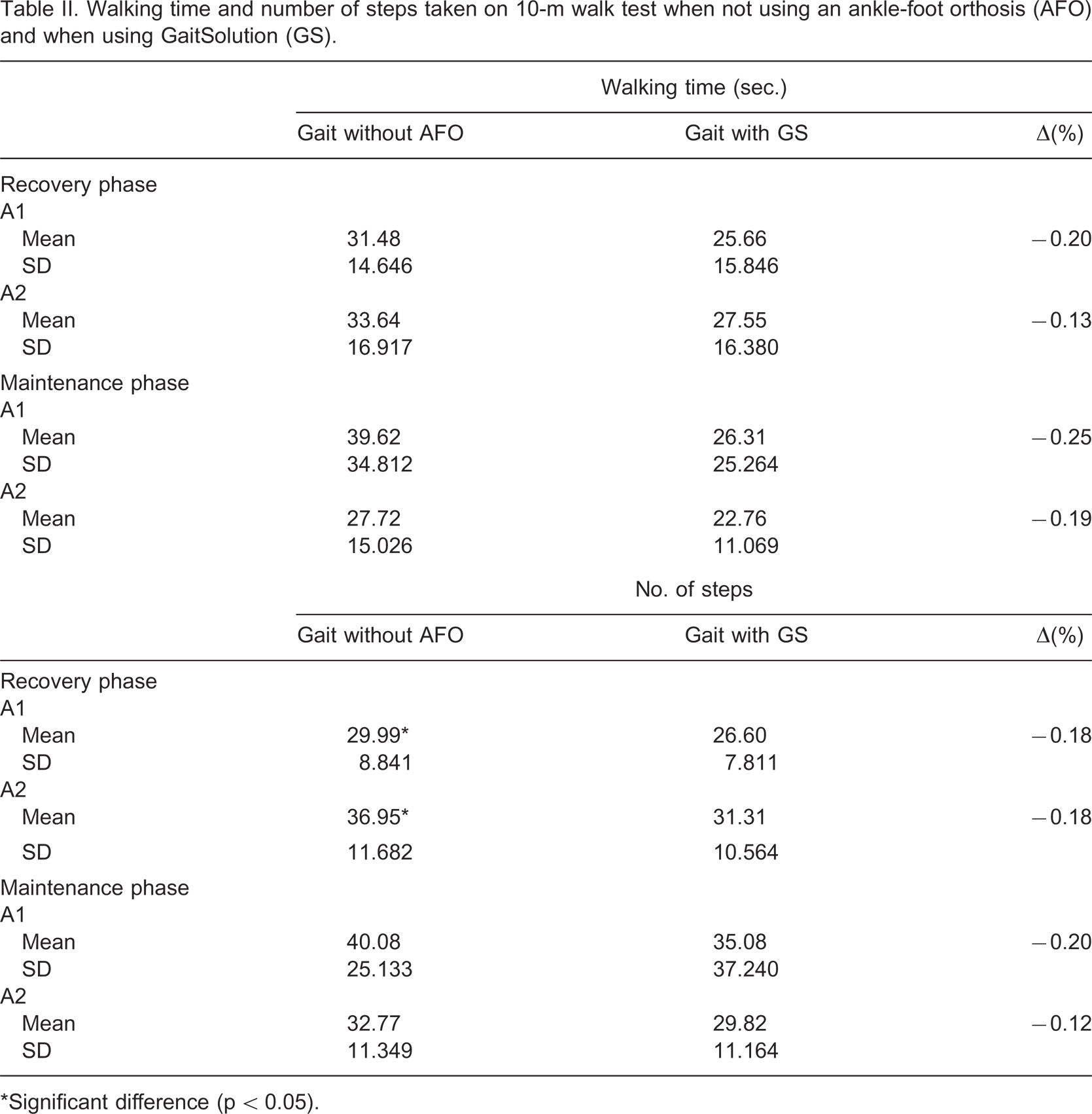
∗Significant difference (p < 0.05).
Patient adaptation to GS function and gait improvement
Approximately 80% of clinicians recognized ankle plantar flexion from initial contact to foot flat (the function of GS), with little difference noted in the number of patients in the recovery phase and maintenance phase (Figure 2a). For those clinicians who could recognize such ankle plantar flexion, approximately 60% reported the patient's gait was improved when using the GS compared to when using his/her own AFO (Figure 2b). A positive response to both questions indicated patients who showed adaptation to GS function.
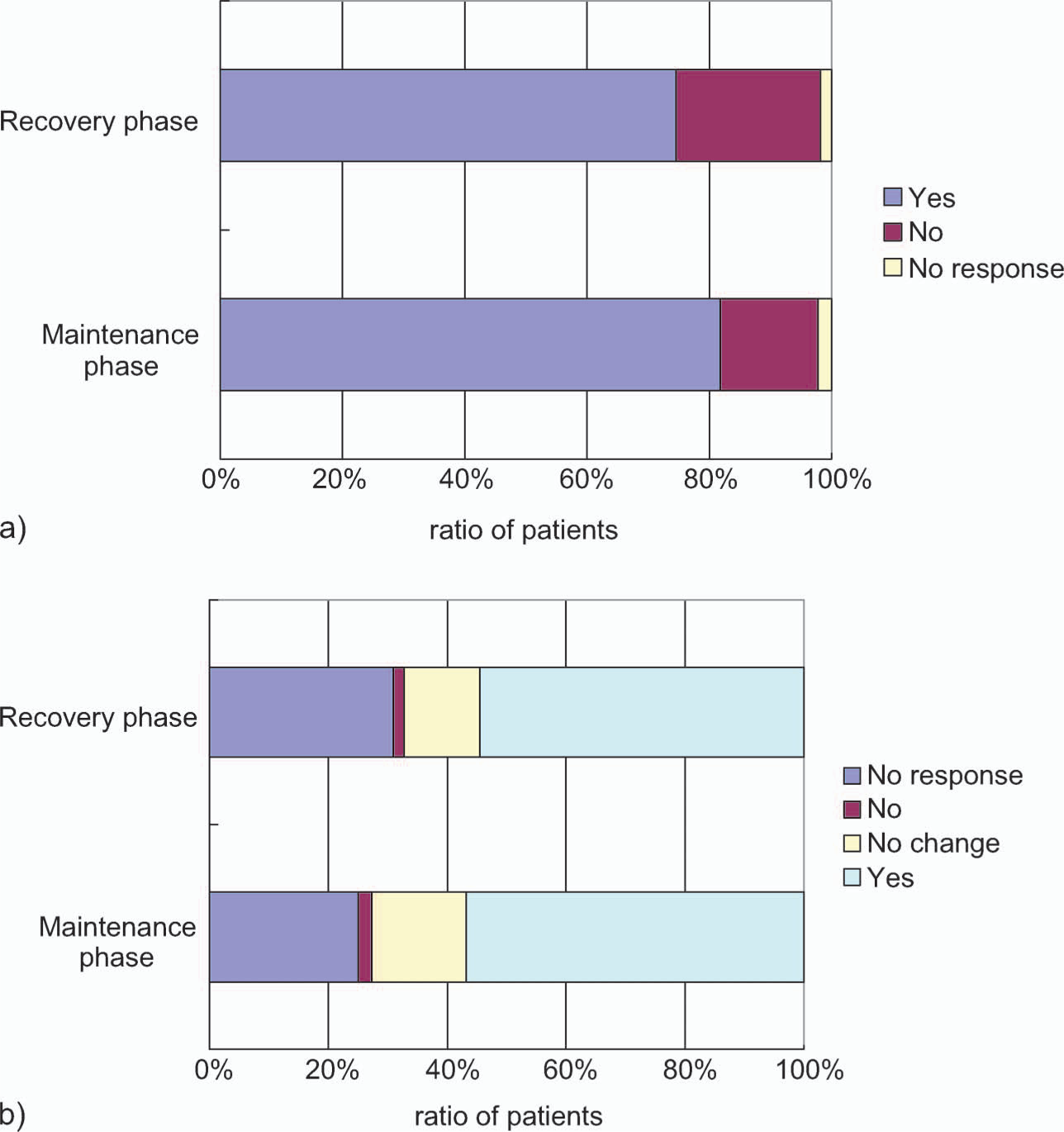
(a) Questionnaire responses concerning plantar flexion and gait improvement. Questionnaire item concerning whether the clinician could recognize ankle plantar flexion from initial contact to foot flat, which is the function of GS. (b) Questionnaire item concerning whether the patient's gait improved using GS compared to using his or her own AFO. ‘No response’ includes cases in which plantar flexion was not recognized in the previous question.
Figure 3 shows the number of patients categorized by Brunnstrom stage. A large number of patients at higher Brunnstrom stages adapted to GS use in both the recovery and maintenance phases. Figure 4 shows the number of patients categorized by patients' own AFO. Patients who used an NAAFO showed a higher adaptational capacity than those who used an AAFO.
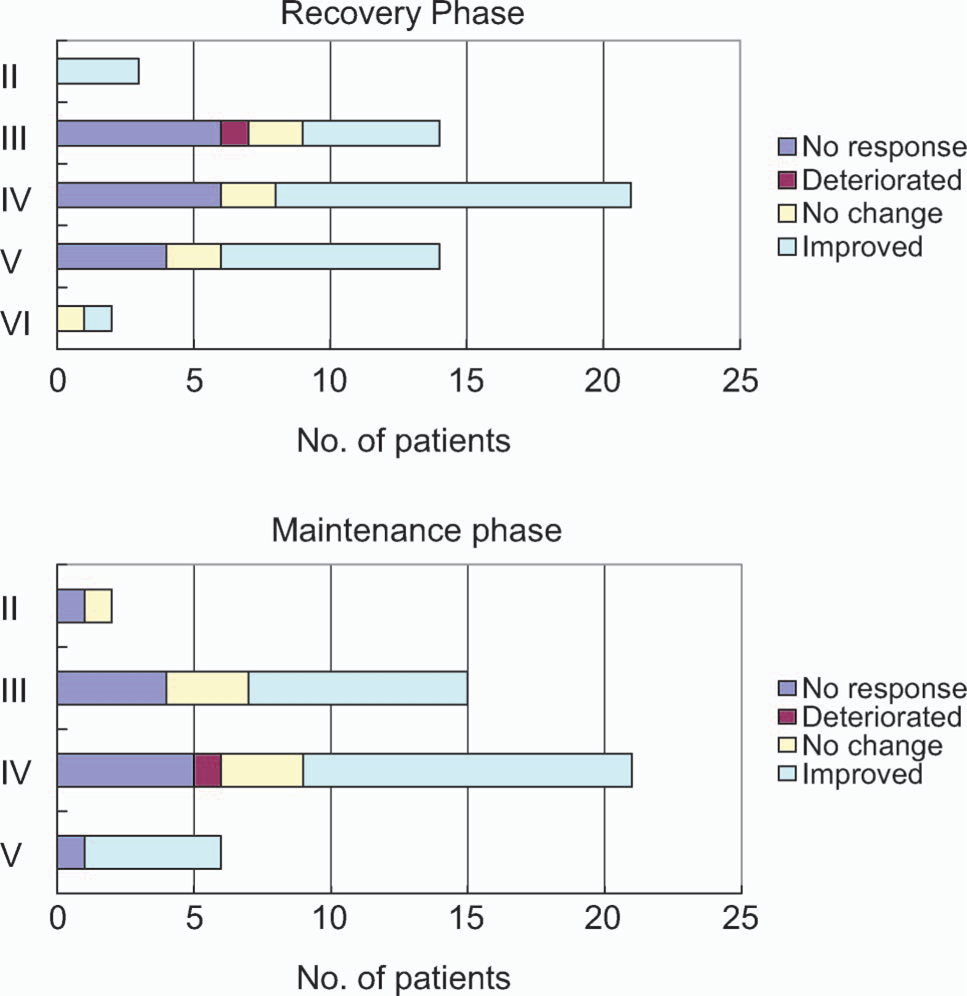
Gait improvement of patients categorized by Brunnstrom stage. ‘No response’ includes cases in which plantar flexion was not recognized.
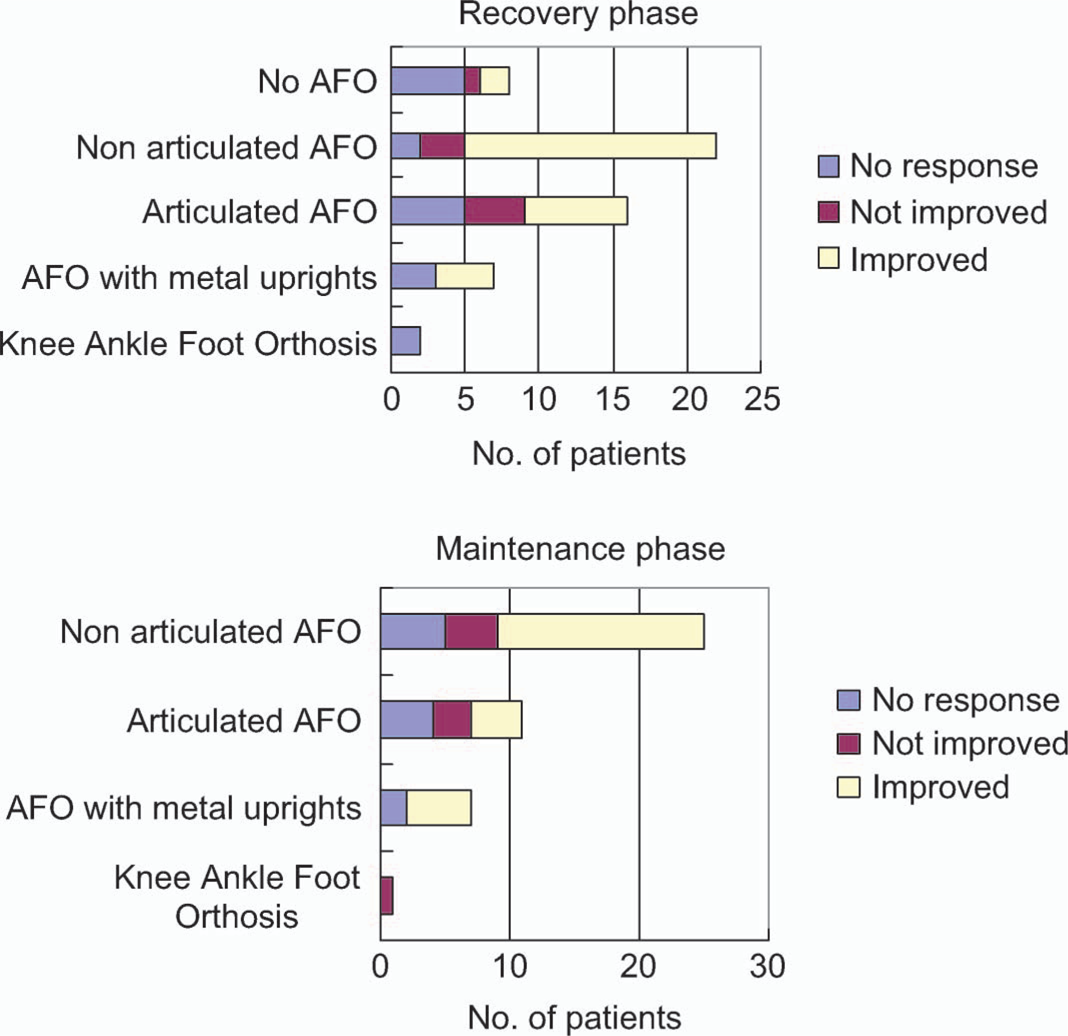
Gait improvement of patients categorized according to the type of their own orthosis. ‘No response’ includes cases in which plantar flexion was not recognized.
Gait parameters affecting adaptation to GS use
Patients were categorized into two groups according to gait following use of GS: Group A1, patients for whom there was a positive response to both questions B and C in the Appendix (n = 55; recovery phase n = 30; maintenance phase n = 25); and Group A2, all other patients including those who showed no change in gait (n = 44; recovery phase n = 25; maintenance phase n = 19). Demographic data and gait data were compared between these groups. Statistical analysis involved unpaired t-tests for data concerning duration and number of steps taken on the 10-m walk test, the Mann-Whitney U-test for unpaired data on an ordinal scale, Wilcoxon's signed-rank test for paired data on an ordinal scale, and the χ 2 test for data on a nominal scale. All results reported as significant were at the p < 0.05 level.
The comparison of demographic data revealed no significant difference between groups A1 and A2 in either phase. The duration and number of steps taken on the 10-m walk test were remarkably reduced on use of GS, but there was no significant difference between groups A1 and A2 except for the number of steps taken by patients in the recovery phase during gait without AFO use (p = 0.028) as shown in Table II.
A comparison of gait data for patients in the recovery phase revealed significant differences for the following parameters.
Initial contact in gait when using GS (p = 0.020).
Knee joint angle during the loading response in gait without AFO use (p = 0.044).
Comparing gait without AFO use to gait with GS use, the following parameters were improved in group A1, but not in group A2.
Hip joint outward rotation (p = 0.014 for group A1, p = 0.982 for group A2).
Trunk upright posture (p = 0.030 for group A1, p = 0.096 for group A2).
Toe off (p = 0.000 for group A1, p = 0.102 for group A2).
The ratios of these gait parameters are shown in Figure 5; Figure 5a shows the parameters for which there was a significant difference between groups A1 and A2, and Figure 5b shows the parameters for which there was a significant difference between gait without AFO use and gait with GS use in group A1 but not in group A2.
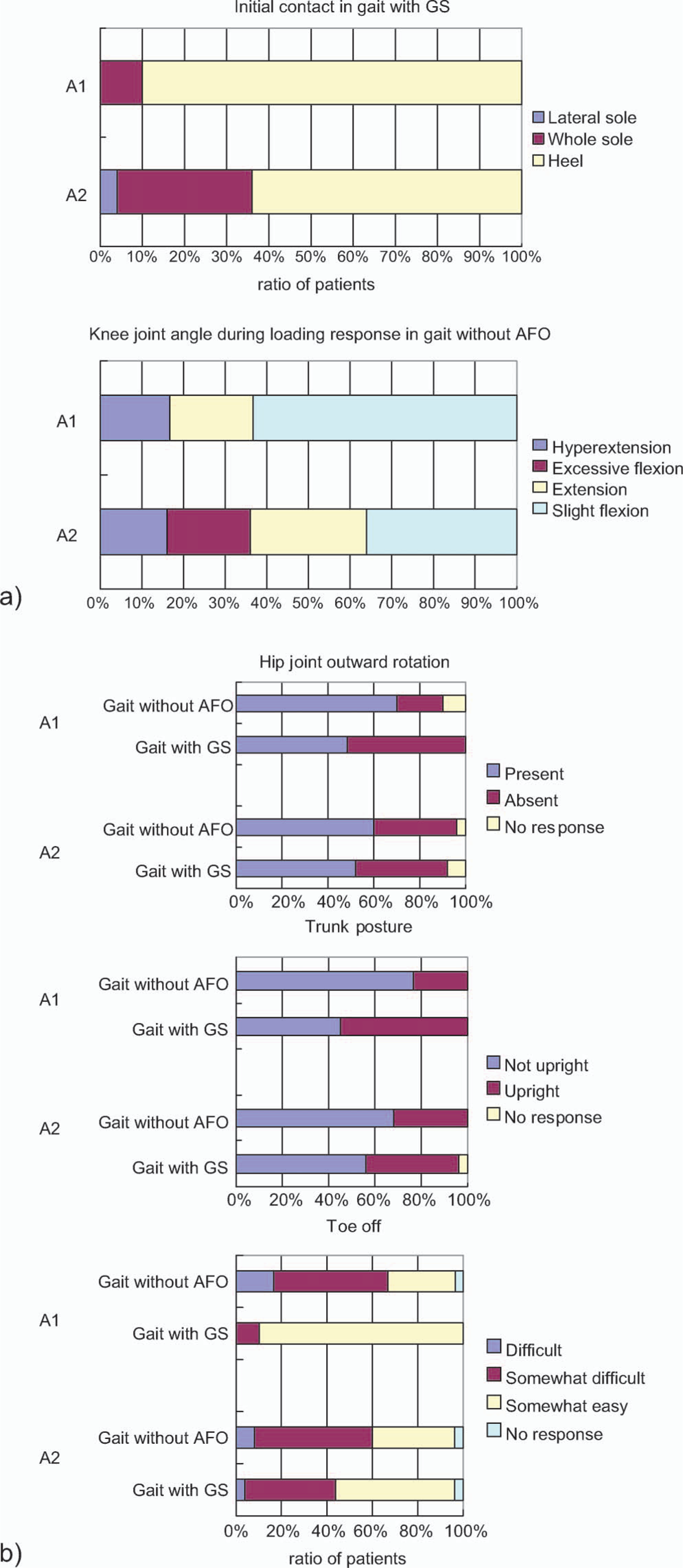
Gait parameters affecting gait improvement of patients in the recovery phase (a) Gait parameters showing the difference between groups A1 and A2. (b) Gait parameters showing the difference between with and without AFO use. A1, improved group; A2, not improved group.
These results indicate that patients in the recovery phase adapted to GS use when they could achieve heel contact, and showed improved hip joint outward rotation, trunk upright posture, and toe off. Patients showing slight knee flexion during the loading response in gait without AFO use tended to adapt to using GS, while patients whose knee joint showed excessive flexion did not.
For patients in the maintenance phase, a comparison of gait data for groups A1 and A2 revealed a significant difference in the following parameter:
Knee joint angle during midstance in gait without AFO use (p = 0.043).
Comparing gait without AFO use to gait with GS use, the following parameters were improved in group A1 but not in group A2.
Trunk upright posture (p = 0.014 for group A1, p = 0.564 for group A2);
Ankle joint angle during swing phase (p = 0.001 for group A1, p = 0.257 for group A2)
The ratios of these gait parameters are shown in Figure 6; Figure 6a shows the parameters for which a significant difference was revealed between groups A1 and A2, and Figure 6b shows the parameters for which a significant difference was found between gait without AFO use and gait with GS use in group A1 but not in group A2.
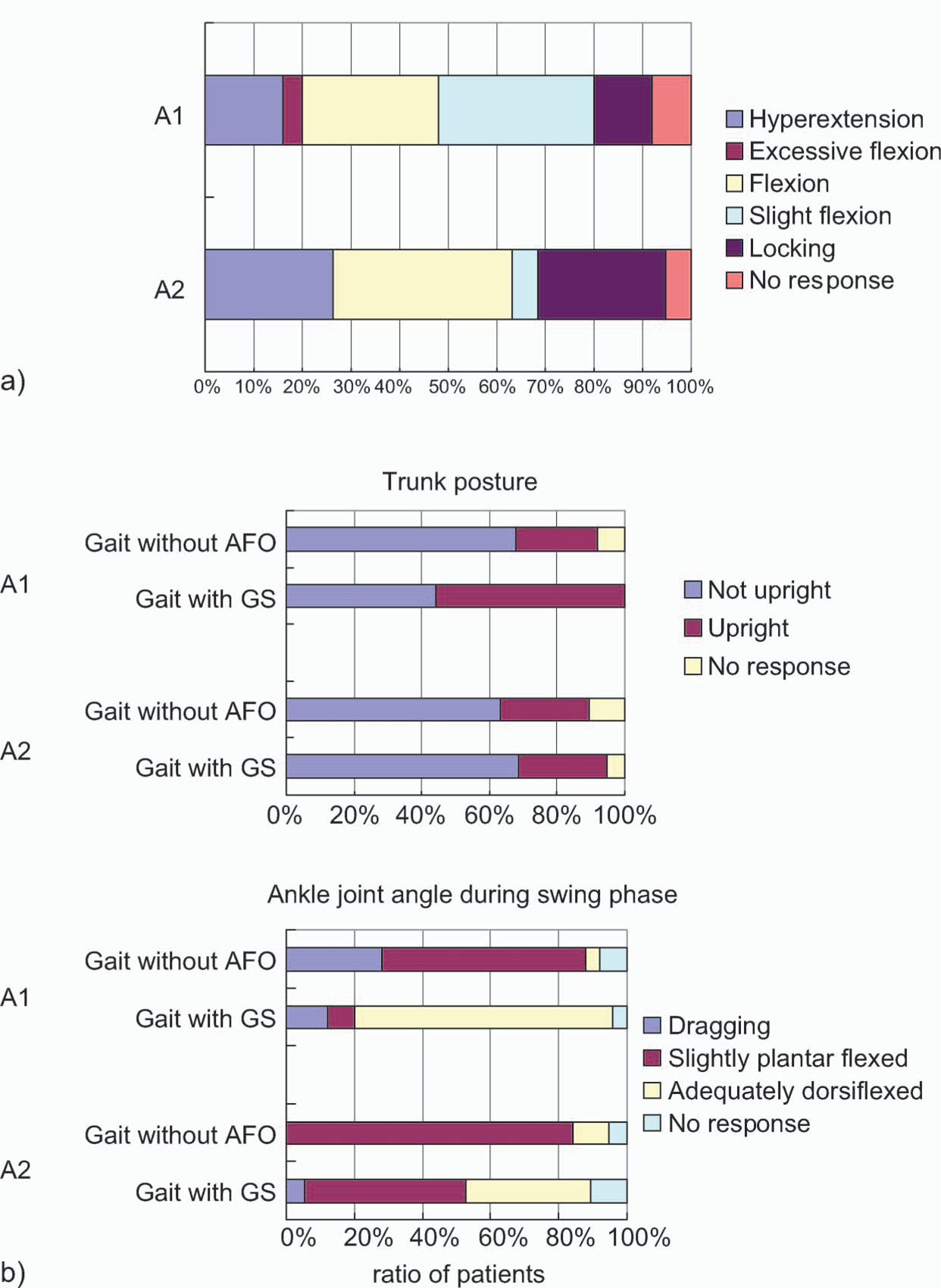
Gait parameters affecting gait improvement of patients in the maintenance phase. (a) Gait parameters showing the difference between groups A1 and A2. (b) Gait parameters showing difference between with and without AFO use. A1, improved group; A2, not improved group.
These results indicate that patients in the maintenance phase adapted to using GS when the trunk upright posture and ankle joint angle during the swing phase were improved by GS use. Regarding the knee joint angle in gait without AFO use, patients who showed slight knee flexion during midstance tended to adapt to GS use, but patients whose knee joint showed locking did not.
Patient opinion
Regarding the question asked of patients, “How did you feel the gait when using GS compared to the gait when using your own AFO?” more than 60% of all patients reported feeling comfortable or extremely comfortable when walking with GS compared to when walking with their own AFO (Figure 7). The number of patients who found walking extremely comfortable using GS was higher in the maintenance phase than in the recovery phase.
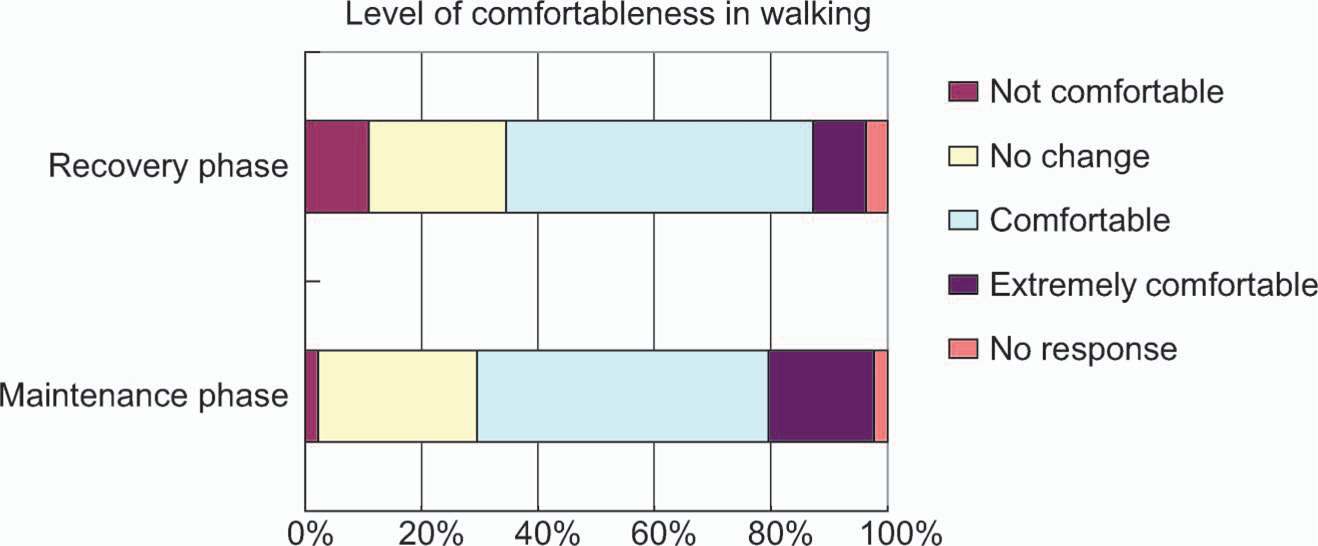
Questionnaire item concerning the level of comfort experienced by patients when walking with GS compared to walking with their own AFO.
According to these results, patients were categorized into two groups: Group B1, patients who answered comfortable or extremely comfortable to question D in the Appendix (n = 53; recovery phase n = 34; maintenance phase n = 19); and Group B2, others (n = 43; recovery phase n = 30; maintenance phase n = 13). Patients who did not answer this question were excluded from the analysis. Differences in gait data between groups B1 and B2 were examined. In this analysis the significance level was modified to p < 0.025 due to regrouping of the data.
As for patients in the recovery phase, gait data for groups B1 and B2 showed no significant difference. Comparing gait without AFO use to gait with GS use, the following parameters were significantly improved in group B1 but not in group B2:
Hip joint outward rotation (p = 0.024 for group B1, p = 0.564 for group B2); Trunk upright posture (p = 0.007 for group B1, p = 0.059 for group B2).
These results indicate that patients in the recovery phase felt comfortable when hip joint outward rotation and trunk posture were improved by GS use (Figure 8a).
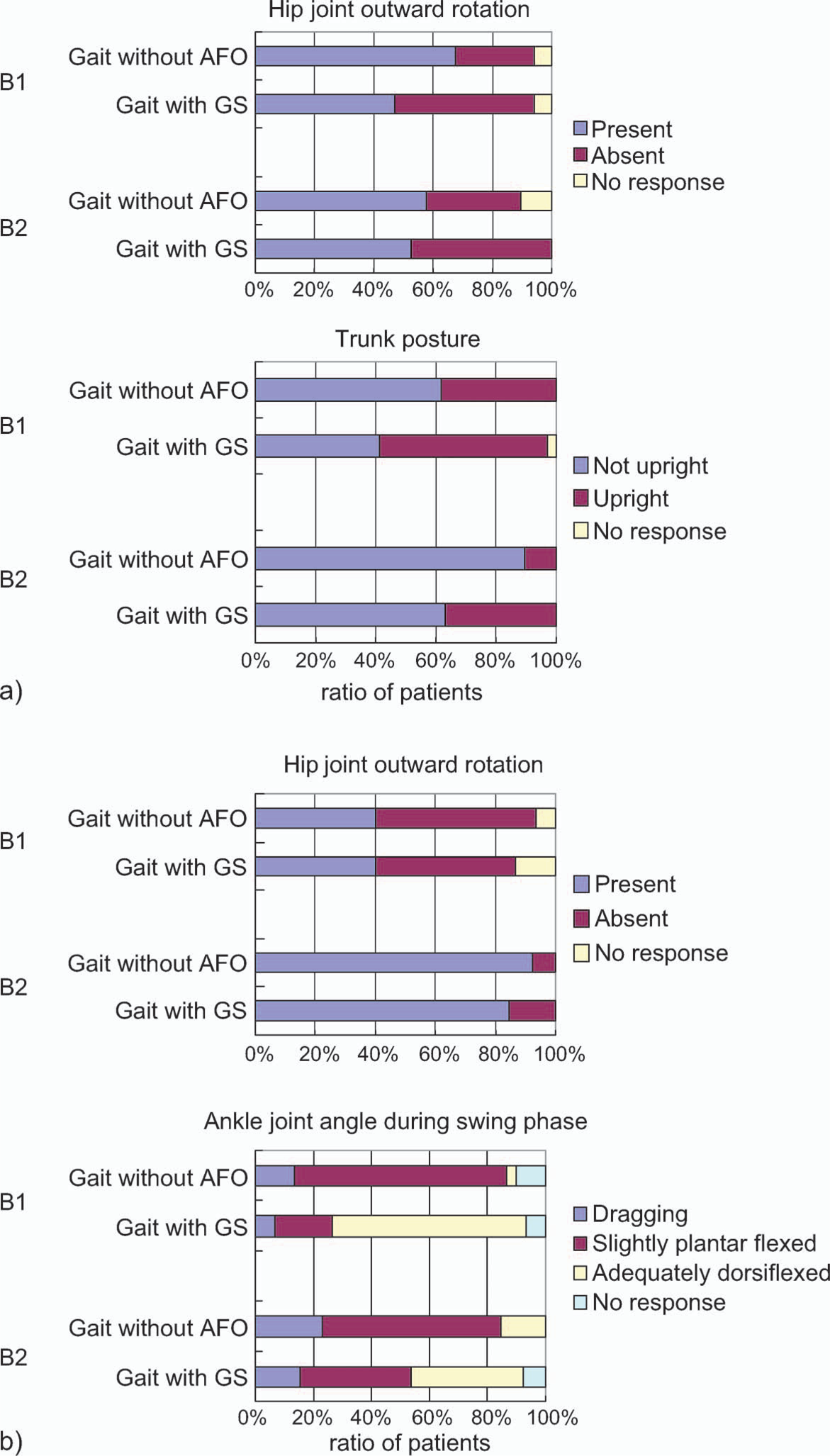
Gait parameters affecting patient comfort. (a) Patients in the recovery phase. (b) Patients in the maintenance phase. B1, comfortable group; B2, not comfortable group.
Regarding patients in the maintenance phase, a significant difference was found for the following parameter:
Hip joint outward rotation in gait without AFO (p = 0.011).
Comparing gait without AFO use to gait with GS use, the following parameter was improved significantly by GS use in group B1 but not in group B2:
Ankle joint angle during the swing phase (p = 0.000 for group B2, p = 0.340 for group B2).
Figure 8b shows that the gait of patients in the maintenance phase who showed hip joint outward rotation was not improved by GS use and gait using GS was uncomfortable. Drop foot could be improved by GS, making gait comfortable.
Relationship between gait improvement and patient comfort
Figure 9 shows the relationship between gait improvement and patient comfort. The top chart includes patients who did not show plantar flexion during the loading response and the other charts show the results of gait assessment by clinicians. Improvement of gait did not necessarily coincide with patient comfort in either the recovery or maintenance phases. When the patient felt extremely comfortable, the clinician assessed the gait to be improved, although in some cases patients felt comfortable but gait was not assessed to be improved, and some patients did not notice any change in comfortableness even though gait was assessed to be improved.
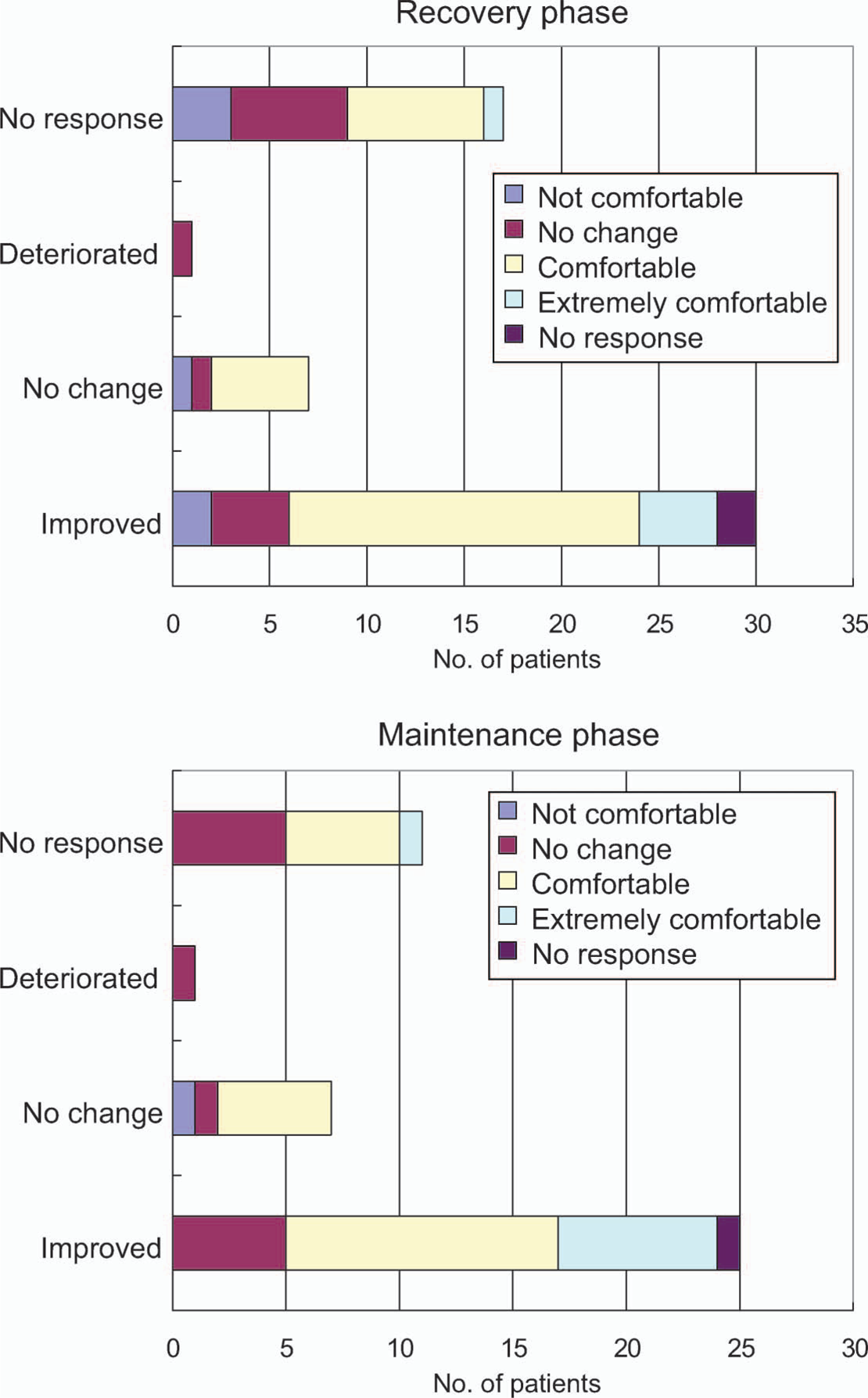
Relationship between gait improvement and patient comfort. In the gait assessment. ‘No response’ includes cases in which plantar flexion was not recognized.
Discussion
In this study, patients who showed the heel rocker function and whose gaits were improved using GS when compared to using their own AFO were considered to have shown adaptation to GS use. Approximately 60% of patients were categorized as such. The selection criterion of patients was a hemiplegic patient who uses an AFO daily or who is willing to use an AFO. However, regarding the demographic data, and in particular age and spasticity (MAS), participants of this study seemed to have somewhat higher gait ability than usual. Therefore, the percentage of adaptation might show some bias.
A greater number of patients with higher Brunnstrom stage showed adaptation to GS use. This result is reasonable because mobility of the GS ankle joint is larger than for other AFOs and it suits dynamic walking. A greater number of patients who used an NAAFO showed adaptation to GS use, which is not surprising since GS is a type of AAFO, and the superiority of AAFOs to NAAFOs in gait improvement was demonstrated in previous studies. 13,14 The present results might involve not only the effect of the oil damper but also that of articulated joints.
From the results obtained here we derive two major points. The first is an understanding of the types of patients that show adaptation to GS function, and the second is an understanding of how gait is improved in patients showing such adaptation. The results of the 10-m walk test revealed that GS suited patients whose steps were not as large as when walking without an AFO. Larger steps meant a shorter stride and step length. Those patients with shorter step length could not benefit from GS use to achieve smooth plantar flexion after initial contact of the paretic limb. Statistical analysis revealed that patients whose knee joint was slightly flexed during the stance phase showed a tendency to adapt to GS use, indicating that GS was suitable for patients who could control their knee joint during gait. Comparing gaits with and without GS use, patients using GS showed improved trunk forward bending, hip outward rotation, toe dragging in the terminal stance, and ankle joint plantar flexion during the swing phase. According to gait theory, body weight is gradually applied to the supporting limb during the loading response, and eccentric contraction of the dorsiflexors and knee extensors achieves forward rotation of the whole body. 17 At the same time, the contraction of the hip extensors maintains the upright position of the trunk. In hemiplegic gait, the activity of the dorsiflexors is not sufficient; the GS was developed to assist this activity. We previously demonstrated by gait analysis the improvement of the trunk movement in gait with GS use in a case series of two patients. 19 In the present study, the findings were replicated among a much larger sample of patients. The improvement seen in toe dragging in the terminal stance and ankle plantar flexion during the swing phase indicate that the assistance provided by GS during the loading response improved gait throughout the whole gait cycle.
Approximately 60% of patients reported improved comfort during gait when using GS, compared to when using their own AFOs. The GS used in the present study was not custom-made and therefore was not shaped to fit the limbs of individual patients. When we consider that patients are already accustomed to wearing their own AFOs, this result implies the superiority of an AFO that achieves heel rocker function. Our findings revealed that patient comfort depended on the lack of hip outward rotation. The hip outward rotation was improved by GS use in patients in the recovery phase but not in the maintenance phase, where patients reported it to be uncomfortable. These results suggest the importance of gait training in the early stage of rehabilitation in order to prevent malposition of the hip joint. Based on the results of this study, GS is a promising tool for gait training.
Footnotes
Acknowledgements
The authors thank Prof. K. Hachisuka of the University of Occupational and Environmental Health Fukuoka, Japan, for valuable advice regarding questionnaire design. We also thank the many patients who participated in this study, and the clinicians and orthotists of Kawamura Co., who fabricated GaitSolution, for their collaboration. This study was financially supported by the New Energy and Technology Development Organization of Japan.
Appendix
Sample of the questionnaire used