
Abstract
This study aimed to provide sonographic imaging of the patellar tendon (PT) – one of the main weight bearing structures for prosthetic use – in transtibial amputees. Thirteen males, who had been under follow-up for unilateral traumatic transtibial amputations, were enrolled. After physical examination of the limb, pain was evaluated by visual analogue scale and Leeds Assessment of Neuropathic Symptoms and Signs. Sonographic evaluations were performed by using a linear array probe (Aloka UST-5524-7.5 MHz) on both sides. Measurements pertaining to the contralateral limbs were taken as controls. In three subjects (23.1%), two with a silicone liner and one with a pelite liner, cortical irregularities were detected at the tibial insertion of the PT on the amputated sides. PTs were found to be thicker on the amputated sides when compared with those of the contralateral sides (p = 0.03), and this increase in thickness correlated with disease duration (r = 0.67, p = 0.01). Overall, our preliminary results imply that after transtibial amputation, PTs of the amputated sides tend to become thicker by time. These findings need to be complemented with future studies. In this regard, sonography seems to be promising for imaging the soft tissue problems of the stump.
Introduction
Attaining adequate coupling between the prosthesis and the transtibial stump is paramount after lower limb amputation. Accordingly, load transfer between the prosthesis and the residual limb has been substantially studied. 1–6 Research mainly concerning the skin complications, i.e., pressure ulcers, blisters, cysts, edema, skin irritation and dermatitis has also been carried out. 7
In non-amputees, patellar tendon problems due to overuse and load bearing have been reported before. 8–10 The role of sonography in clearly demonstrating the relevant pathological findings – even better than magnetic resonance imaging – is again well established. 10 Further, the relationship between the sonographic findings and the painful complaints of such patients has also been shown. 8,10 Herewith, considering the fact that the patellar tendon (PT) is the main weight bearing structure for prosthetic use in transtibial amputees, it would not be unfounded to expect certain structural damage also in the amputee patients. However, to our best notice, any possible changes have not been studied in the hitherto literature. Therefore, the purpose of this study was two-fold; first, we considered that sonography could provide detailed imaging of the PT in transtibial amputees and second, we aimed to find out whether clinical and sonographic findings could be interrelated.
Methods
Thirteen males who had been under follow-up after unilateral transtibial amputations due to traumatic injuries were enrolled. They had completed stump healing and none of the subjects had concomitant (metabolic or rheumatologic) diseases that would impact the PT. All were otherwise healthy and active young individuals who were using their prostheses at least 10 hours a day. The subjects were informed about the procedure and consented to participate. The study protocol was approved by the Institutional Review Board.
Patient demographics, medical history and type of amputation/prostheses were recorded. After physical examination of the limb, pain was evaluated by visual analogue scale (VAS) and LANSS (Leeds Assessment of Neuropathic Symptoms and Signs). 11
Sonographic evaluations were performed by a physiatrist experienced in musculoskeletal sonography (LÖ). A linear array probe (Aloka UST-5524-7.5 MHz) was used for visualizing the PTs on both sides while the patients were kept in supine position. On longitudinal view, starting from the inferior pole of the patella until its insertion on the tibial tuberosity, the PT was visualized for any pathology (Figure 1). Particular care was taken to ensure that the scan planes were parallel to the tendon fibers to avoid acoustic fiber anisotropy. In case of an abnormality, it was also confirmed on the axial view. PT thicknesses were measured at the midportion of its alignment on axial imaging. The values pertaining to the contralateral limbs were taken as controls.
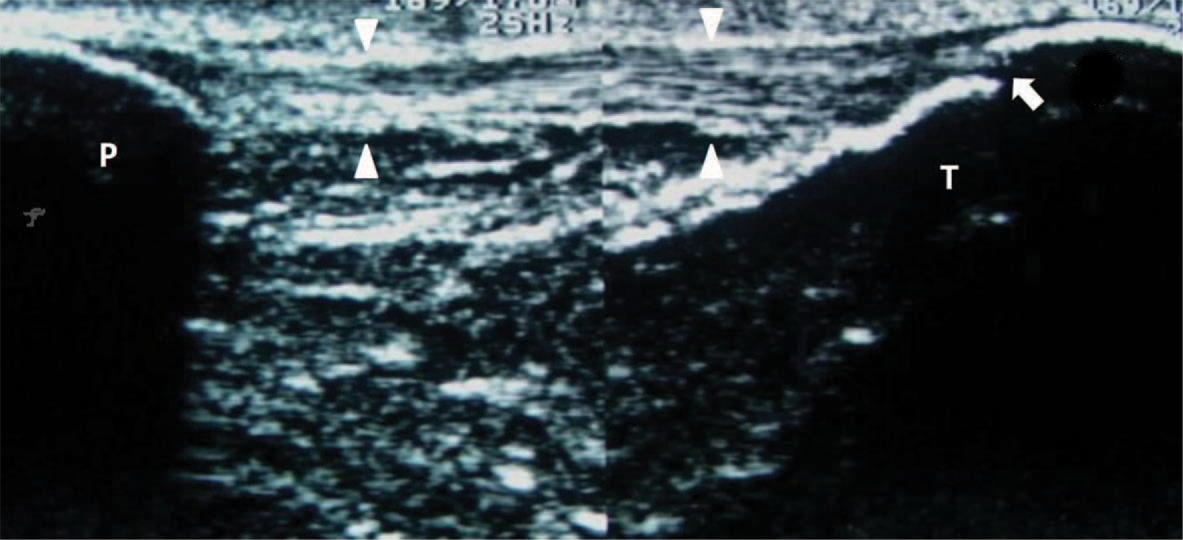
Sonography of the patellar tendon (longitudinal split-screen view). The tendon is seen as a hyperechoic fibrillar structure (between the white arrow heads) extending from the inferior pole of the patella (P) and inserting on the tibial tuberosity (T). A small cortical irregularity is observed on the distal region of its insertion (white arrow).
PT thickness values were compared by Wilcoxon (contralateral vs. amputated limbs) and Mann-Whitney U (between groups) tests. Correlations were analyzed by Spearman coefficients. SPSS 15.0 was used for statistical analysis and p values less than 0.05 were considered significant.
Results
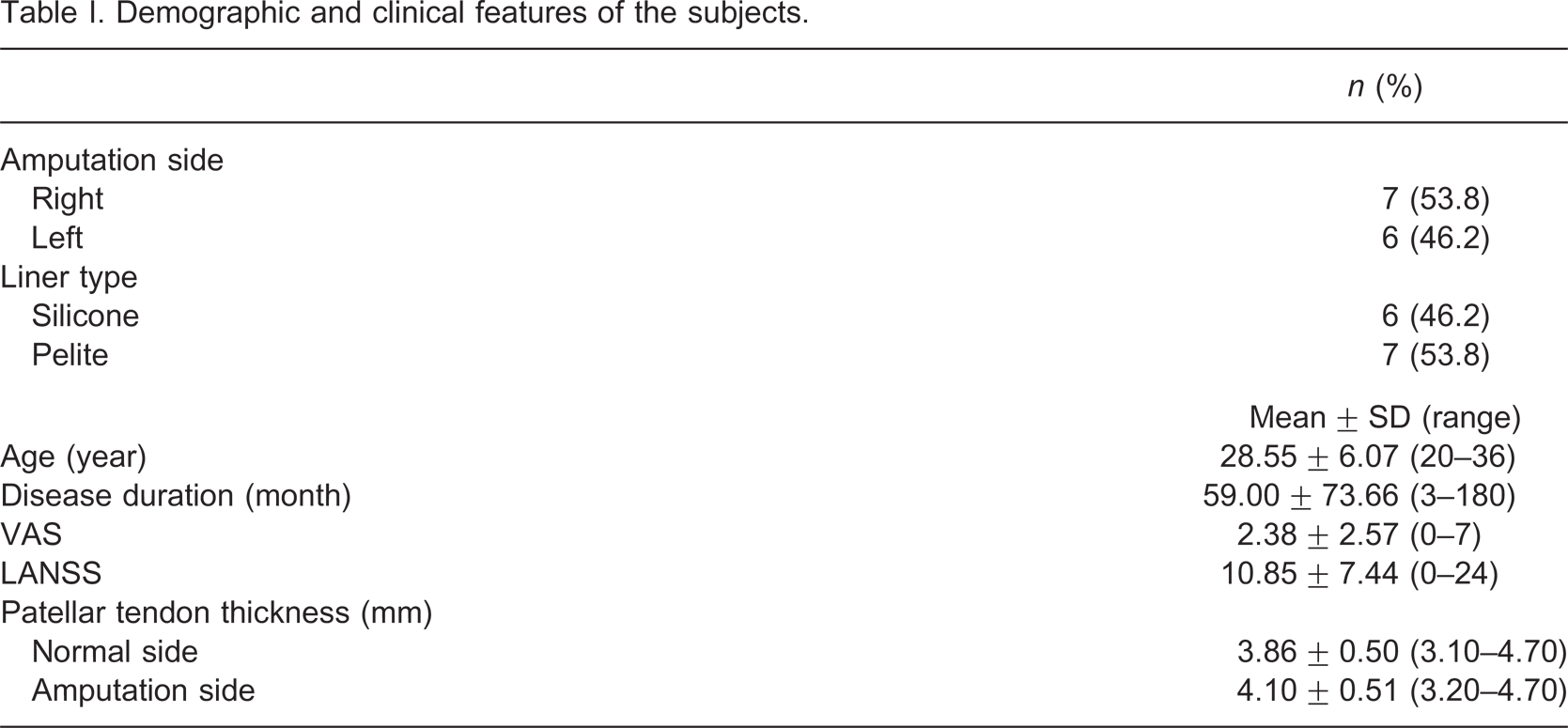
Demographic and clinical features of the patients are given in Table I. In three subjects (23.1%), two with a silicone liner and one with a pelite liner, cortical irregularities were detected at the tibial insertion of the PT on the amputated sides. Any other findings like tendonitis/rupture or bursitis were not present. The PT thickness values were found to be increased on the amputated sides of the patients when compared with the contralateral sides (p = 0.03). PT thickness values regarding the amputated limbs were found to be similar between subjects with silicone vs. pelite liners (p > 0.05). PT thicknesses of the amputated sides (r = 0.67, p = 0.01) – but not of the contralateral sides (r = 0.33, p = 0.27) – were positively correlated with disease duration. The thickness measurements were not correlated either with VAS or LANSS scores.
Demographic and clinical features of the subjects.
Discussion
In this study, we have evaluated the PTs of transtibial amputees by using sonography for the first time in the literature. The main aspect of our results worthy of discussion is the thickening of the PTs (amputated vs. contralateral sides) in parallel with disease duration.
Indisputably, stresses come into being at the stump/socket interface during activities of daily living and tissue injuries due to either sustained or intermittent peak pressure caused by the prosthetic socket may ensue. Yet, the residual limb does not have the same load-bearing capability as the plantar surface of the foot. Although the relevant mechanical problems are generally reflected to the skin, the underlying soft tissues can also be involved. Along with the other weight tolerant areas, i.e., medial tibial flare, residual pretibial musculature of the anterior compartment, the gastrocnemius muscle belly and the fibular shaft; PT has long been used as a reference point for load transfer in prosthetic design. 12 Therefore, it is inevitably a site that contains high risk of compromise. Accordingly, in this study, we reasoned that sonography could be used to uncover such possible structural changes of the PTs in transtibial amputees.
Tendons are the force transmitting units of the musculoskeletal system. Due to their low metabolic rate and slow healing, injuries of these structures produce considerable morbidity and the eventual disability may be quite lengthy despite what is considered appropriate management. According to our results, apart from the cortical irregularities (23.1%) which may indicate mechanical damage, PTs of our patients were found to be thicker on the amputated sides. This increase in thickness was also correlated with the disease duration but not with the pain scores. When compared with studies on non-amputees, PT problems have previously been demonstrated with sonography. 8,10 Although structural pathologies could be easily diagnosed, similar to our study, painful complaints of the patients were not always correlated with the gray-scale sonographic findings. 8 On the other hand, color Doppler imaging was found to be better predictive of acute and symptomatic pathologies. 10
Again, the liner types seemed not to have any impact on the thickness values. Herein, considering the patient spectrum of our study (with reasonable amount of prostheses use), we imply that cumulative stress on the PT might have caused this thickening. However, as this increase was not reflected on the complaints of the patients (pain scores), the clinical relevance of our findings needs to be elucidated. Yet, keeping in mind the fact that the tensile strength of tendons is mainly related to the thickness and the collagen content, our findings may either be due to a secondary adaptation or chronic asymptomatic tendinitis. On the other hand, it is noteworthy that larger samples and more detailed history concerning the liner use (including all the types and their cumulative duration) would be necessary to substantiate our initial results.
Conclusion
To summarize, in the light of our first and preliminary findings, we may conclude that PTs (on the amputated sides) seem to get thicker after transtibial amputations and that this increase parallels the disease duration. On the other hand, drawing attention also to the accompanying cortical changes in 23.1% of the patients, our results need to be complemented with future studies. Furthermore, highlighting the benefits of sonography also concerning the other soft tissue problems regarding the stump, 13,14 we imply that sonography is also beneficial for the evaluation of PT problems in amputee patients.
Footnotes
Acknowledgements