
Abstract
There is an increasing need for outcome measures in the orthotic and prosthetic field and specifically a lack of outcome measures in Swedish. The Orthotics and Prosthetics Users' Survey (OPUS) was developed in the USA for assessment of the outcome of orthotic and prosthetic interventions, and could potentially also be used for shoe insoles and orthopaedic shoes. The aims of this study were to translate OPUS into Swedish and test the translated version's linguistic validity in a Swedish context. The Orthotic and Prosthetic Users' Survey was translated into Swedish and back-translated into English, following a modified version of the World Health Organization guidelines. After revision of the Swedish version, 39 Swedish clients (12 men, 27 women) answered the OPUS questionnaires and were systematically debriefed afterwards. Most items were understood correctly by the respondents, but some words and expressions had to be changed to avoid misunderstandings or unintended interpretations. The resulting Swedish version of OPUS, OPUS-Swe, showed acceptable linguistic validity and has potential for use in both clinical practice and scientific settings. Nevertheless, before OPUS-Swe can be fully implemented, its psychometric properties need to be evaluated.
Introduction
During the last decades, orthotic and prosthetic (O&P) research has mainly focused on biomechanics and engineering. 1 However, while assessment of the mechanical outcome of use of a device can explain how it works, it cannot answer the more fundamental question of whether it is effective, i.e., whether the device has an impact on the person's everyday life. The intended impact is the self-experienced gain from using the device and can be assessed, for example, through the use of self-report surveys.
Several self-report instruments have been developed for the O&P field, 1–10 but only two are available in Swedish, and their use is limited to clients with prosthesis. 4,6 No Swedish self-report instruments are available for assessing the outcome in clients using orthoses, orthopaedic shoes, or shoe insoles. Hence, a large group of Swedish O&P clients are left without any instrument for systematic follow-up.
Orthotics and Prosthetics Users' Survey
In contrast to most self-report instruments in O&P, the Orthotics and Prosthetics Users' Survey (OPUS)
1
was developed to assess the outcome in both orthotic and prosthetic users. The instrument consists of five independent modules:
Upper Extremity Functional Status (UEFS) module consisting of 23 items covering activities of daily living (ADL).
Lower Extremity Functional Status (LEFS) module consisting of 20 ADL items. The UEFS and LEFS module items are rated on a 5-level Likert scale ranging from 1 = ‘Very easy’ to 5 = ‘Cannot perform activity’.
Client Satisfaction with Device (CSD) module consisting of 11 items.
Client Satisfaction with Services (CSS) module consisting of 10 items. The CSD and CSS module items are rated on a 4-level Likert scale ranging from 1 = ‘Strongly agree’ to 4 = ‘Strongly disagree’.
Health Related Quality of Life (HRQoL) module consisting of two parts. Part I has 12 items covering the social consequences of the physical condition rated on a 5-level Likert scale ranging from 1 = ‘Not at all’, to 5 = ‘Extremely’. Part II has 11 items covering the client's emotions during the past week rated on a 5-level Likert scale ranging from 1 = ‘All of the time’ to 5 = ‘None of the time’.
Thus, while being applicable to most O&P clients, and, also, including common goals for O&P treatment, OPUS has the potential for use in a wide range of the Swedish O&P field. The Orthotics and Prosthetics Users' Survey was developed in English and has displayed good internal consistency. 1 It has been translated into Spanish (A.W. Heinemann, personal communication 2007) and into Slovenian. 11 Hitherto, there has been no Swedish version of OPUS.
When translating an instrument for use in a new cultural context, the aim is to achieve conceptual rather than literal equivalence, 12,13 that is, the concepts assessed by the instrument should have the same meaning within the cultures concerned. While focusing on the conceptual equivalence, three aspects of equivalence have to be considered by the translators: 12,14,15 (i) Semantic equivalence, which implies that words and expressions have the same meaning after the translation as they had before; (ii) Experiential equivalence, which means that the new target group is familiar with the situations described in the items; and (iii) Idiomatic equivalence, which refers to how idioms, which seldom can be translated literally, should be expressed in the target language.
Previous studies using systematic translation and validation procedures have shown that linguistic and cultural adjustments of the text may be necessary to achieve conceptual equivalence, i.e. linguistic validity, of the instrument in the new cultural context. 16–19 For this reason, a translation of OPUS into Swedish needs to be conducted in a systematic way and be followed by a linguistic validation.
Hence, the aims of this study were to: (i) Translate OPUS into Swedish, and (ii) test the linguistic validity of the translation in a Swedish context.
Methods
Although various guidelines for the process of questionnaire translation have been proposed, 12–15 there is a consensus in the literature about the main elements in the procedure: (i) Forward translation into the target language; (ii) back-translation into the source language; (iii) consensus meetings of people involved; and (iv) testing of the translation to the target language, with or without cognitive debriefing of the respondents. The test and cognitive debriefing constitute the linguistic validation of the instrument. This procedure is compatible with the guidelines for translation and adaptation of instruments published by the World Health Organization (WHO), 13 and several studies have used this method successfully, with minor modifications. 6,17–23 The procedure used in the present study was a modified version of these guidelines (Figure 1).

Procedure for translating the Orthotics and Prosthetics Users' Survey from English to Swedish.
Forward translation and first consensus version
Four certified medical professionals, a prosthetist/orthotist, an occupational therapist, a physical therapist, and an orthopaedic surgeon, were recruited to translate OPUS to Swedish. All translators received a written Swedish version of the translation instructions proposed by WHO 13 together with the original English version of the OPUS modules. When the translations were completed, the four Swedish translations were merged into a single set of modules by the first author. When the wording in the translations differed, the different translation alternatives were included in the text. The translators and authors met twice to discuss the translation alternatives and as a result a first Swedish consensus version was created.
Back-translation and second consensus version
The back-translation was performed by an independent translator whose mother tongue was English and who had no previous knowledge of OPUS. Like the forward translation, it was intended that the back-translation should aim at conceptual rather than literal equivalence. Hence, the translator received the same written translation instructions as were given to the forward translators, in addition to the first Swedish consensus version of OPUS. Subsequently, the resulting back-translation was compared with the English original and with the first Swedish consensus version by the authors. In cases of discrepancies between the versions, the wording in the Swedish version was changed to come closer to the original English version. The back-translation was also sent to the developer of OPUS, Professor Allen W. Heinemann, with explanatory comments and with suggestions for interpretation of the discrepancies between the original and the back-translation.
Based on the results of the back-translation and on comments made by the developer of the instrument, a draft for a new Swedish version was sent to the four forward translators for approval. After their consent, this was adopted as the second consensus version of OPUS.
Linguistic validation and final Swedish version
The method for linguistic validation was based on in-depth interviews with structured questions adopted from the WHO guidelines. 13 At least 10 persons should answer each section of an instrument in a linguistic validation. 13 Since OPUS consists of five modules, with the two shortest modules (CSD and CSS) treated as one, 40 subjects were needed. Furthermore, the respondent group should be representative of those to whom the instrument is to be administered and include persons of different gender, ages and socio-economic groups. 13
Subjects
Thirty-nine persons (27 women, 12 men, mean age 59.8 years, age range 20–82) participated in this study. The sample was selected with the principal aim that the respondents should represent users of different kinds of orthopaedic assistive devices. Persons below 18 years of age and persons unable to understand the questions correctly because of poor language skills or low cognitive level were excluded. The recruitment of participants continued until 10 persons had answered each module (Table I).
Characteristics of the 39 subjects participating in the linguistic validation of the Orthotics and Prosthetics Users' Survey (OPUS), distributed among the OPUS modules.
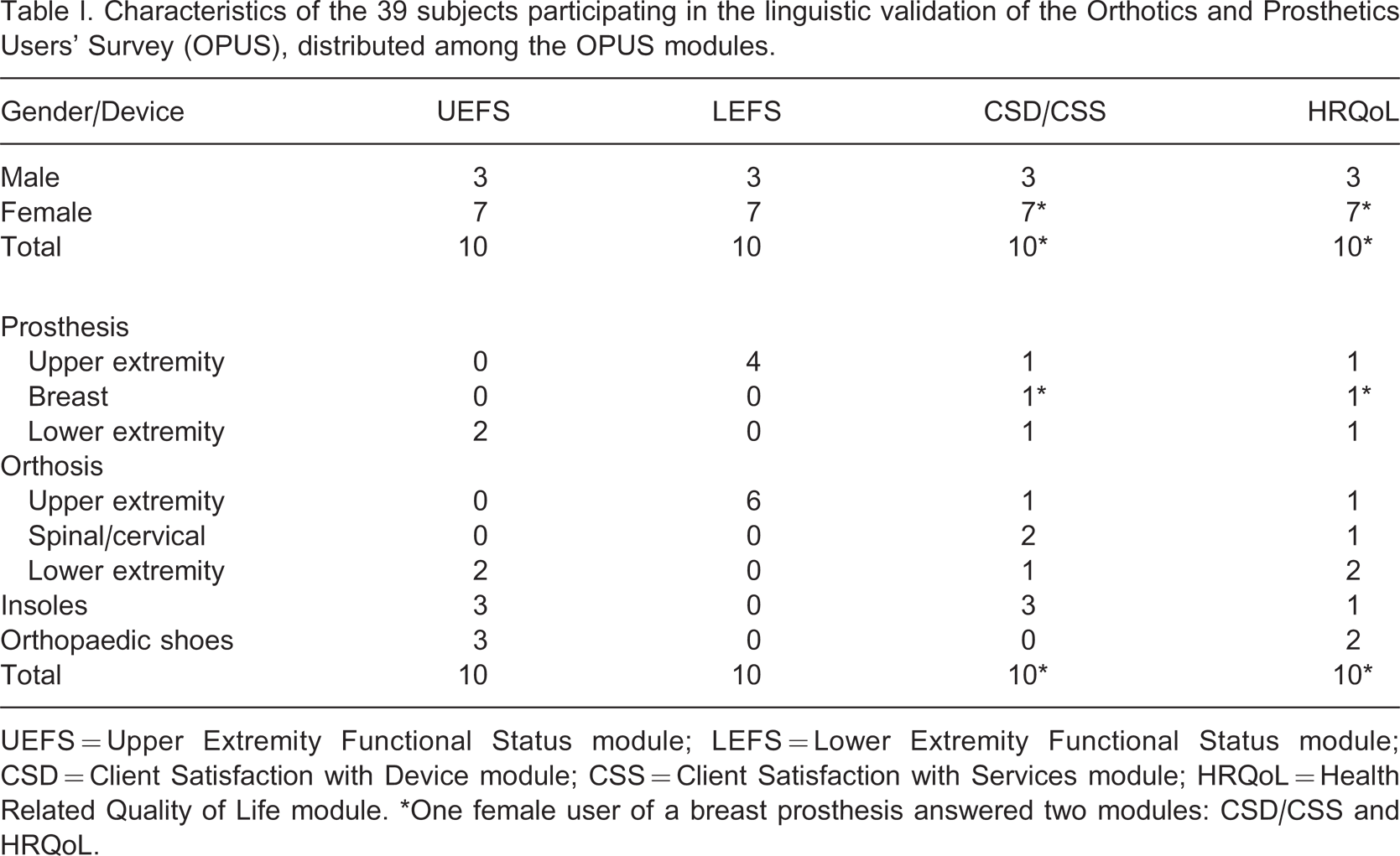
UEFS = Upper Extremity Functional Status module; LEFS = Lower Extremity Functional Status module; CSD = Client Satisfaction with Device module; CSS = Client Satisfaction with Services module; HRQoL = Health Related Quality of Life module. ∗One female user of a breast prosthesis answered two modules: CSD/CSS and HRQoL.
Procedure
After approval by the Regional Ethics Committee review board, outpatients at the Department of Prosthetics and Orthotics, Örebro County Council, Sweden, were selected and recruited for this study. Prior to a scheduled visit at the outpatient clinic, the clients were contacted by phone, informed about the study and asked for participation. If they agreed to participate, written information was sent by mail or given at the appointment.
In conjunction with the appointment at the clinic, the clients received further information about the study and gave their consent to participation. The clients completed the OPUS modules and were afterwards systematically debriefed at in-depth personal interviews following the guidelines by WHO. 13 The first participant completed two modules, but the cognitive debriefing proved to be too time consuming. For this reason, the subsequent participants completed only one module each. The interviews were conducted by an experienced interviewer in a secluded room and were recorded in writing. In accordance with the guidelines, 13 the clients were asked what they thought the questions were asking about, whether there was any word they did not understand, et cetera.
Analysis
The records from the interviews were reviewed question by question by the interviewer and the first author. Items, expressions and words that were misunderstood, incorrectly interpreted or found unacceptable were discussed to find a more straightforward and appropriate formulation. Furthermore, special attention was paid to any other comments made at the interviews, i.e., regarding layout and difficulty in understanding the modules. Problems encountered were discussed with the developer of the instrument.
Results
Both the back-translation and the linguistic validation led to several linguistic adjustments of OPUS items for the final Swedish version. These were made during different stages of the translation procedure and examples of the adjustments are presented in Table II.
Examples of adjustments of expressions and items made during the process of translating the Orthotics and Prosthetics Users' Survey from English to Swedish.
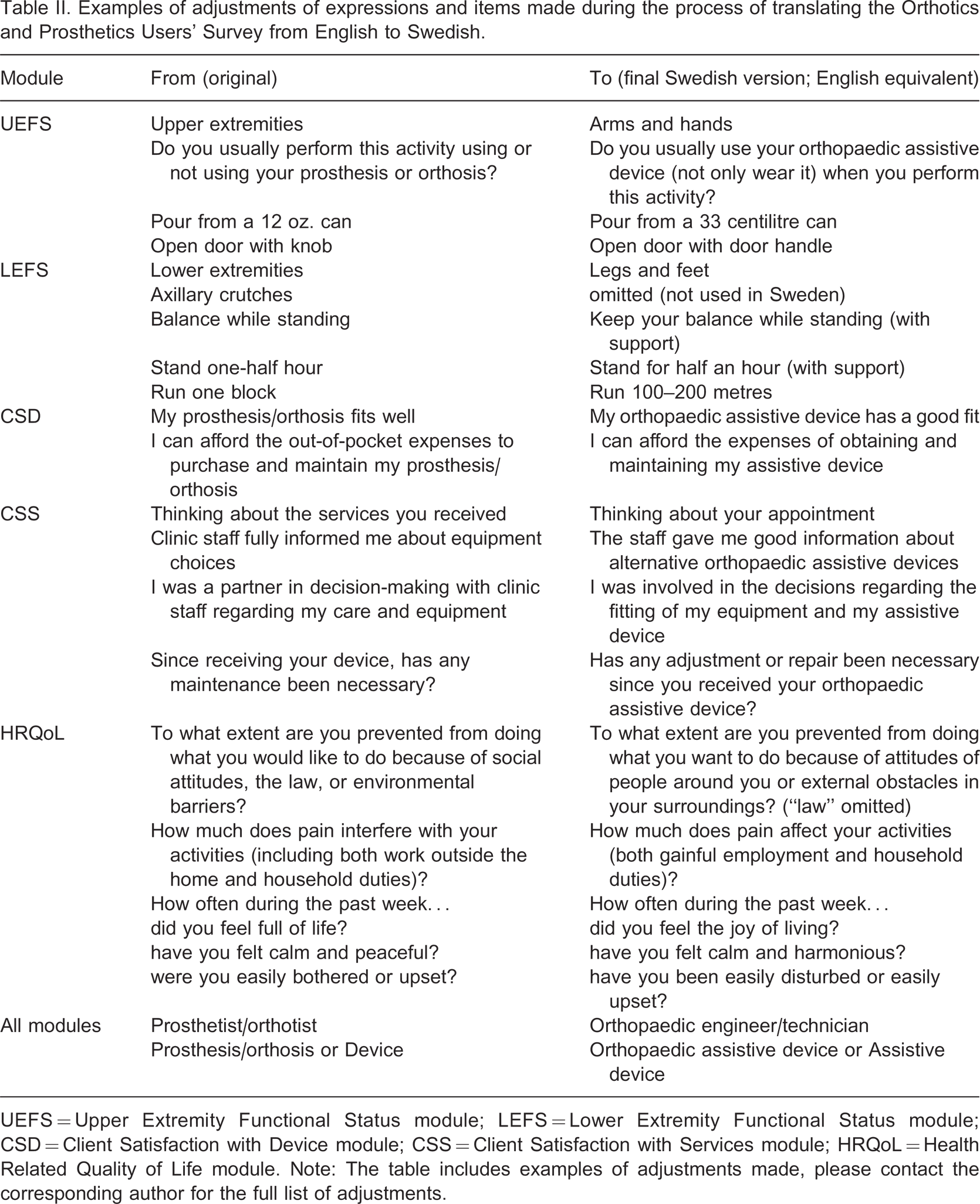
UEFS = Upper Extremity Functional Status module; LEFS = Lower Extremity Functional Status module; CSD = Client Satisfaction with Device module; CSS = Client Satisfaction with Services module; HRQoL = Health Related Quality of Life module. Note: The table includes examples of adjustments made, please contact the corresponding author for the full list of adjustments.
Back-translation and second consensus version
On the whole, the discrepancies between the English original and the back-translation were small, and due to semantic adjustments during the forward translation. Some semantic adjustments of the Swedish version were made after the back-translation in order to come closer to the English original text (two items in CSD, three items in CSS, eleven items in HRQoL). In a similar way, some of the introductory text and headings were adjusted. When the differences between the original and the back-translation were due to well-motivated adjustments during the forward translation, they were accepted. The resulting Swedish version was then adopted as the second consensus version.
Linguistic validation and final Swedish version
The results from the linguistic validation showed that the items in most cases were understood as intended. The only item that was clearly misunderstood was “my prosthesis/orthosis fits well” (CSD). The Swedish expression used was ambiguous and could also be interpreted as meaning “my prosthesis/orthosis is appropriate for its purpose”. Consequently, five respondents misunderstood the item and it was therefore necessary to adjust the translation using more unambiguous wording. In addition to this adjustment for semantic equivalence, further adjustments were necessary to improve the experiential and idiomatic equivalence.
One respondent asked if support was allowed in the activities “balance while standing” and “stand one-half hour” (LEFS). In these cases clarification was made in parentheses after the question (Table II). Nine respondents found the Swedish word “extremiteter” (“extremities”, UEFS and LEFS) strange, hard to understand, and unacceptable. This expression was therefore replaced by “arms and hands” or “legs and feet”. The interviews also revealed some misunderstandings of the introductory text of the modules, necessitating some adjustments (Table II).
Some of the response alternatives were changed for semantic reasons or reasons of consistency (Table III). The developer of the instrument gave his approval of these alterations. Nine respondents of the UEFS and LEFS modules commented on or misunderstood the response alternative “Not applicable”, which was considered too similar to the Swedish expression for “Cannot perform activity”. For this reason, a clarification was added after “Not applicable”.
Adjustments of response alternatives when translating the Orthotics and Prosthetics Users' Survey from English to Swedish.
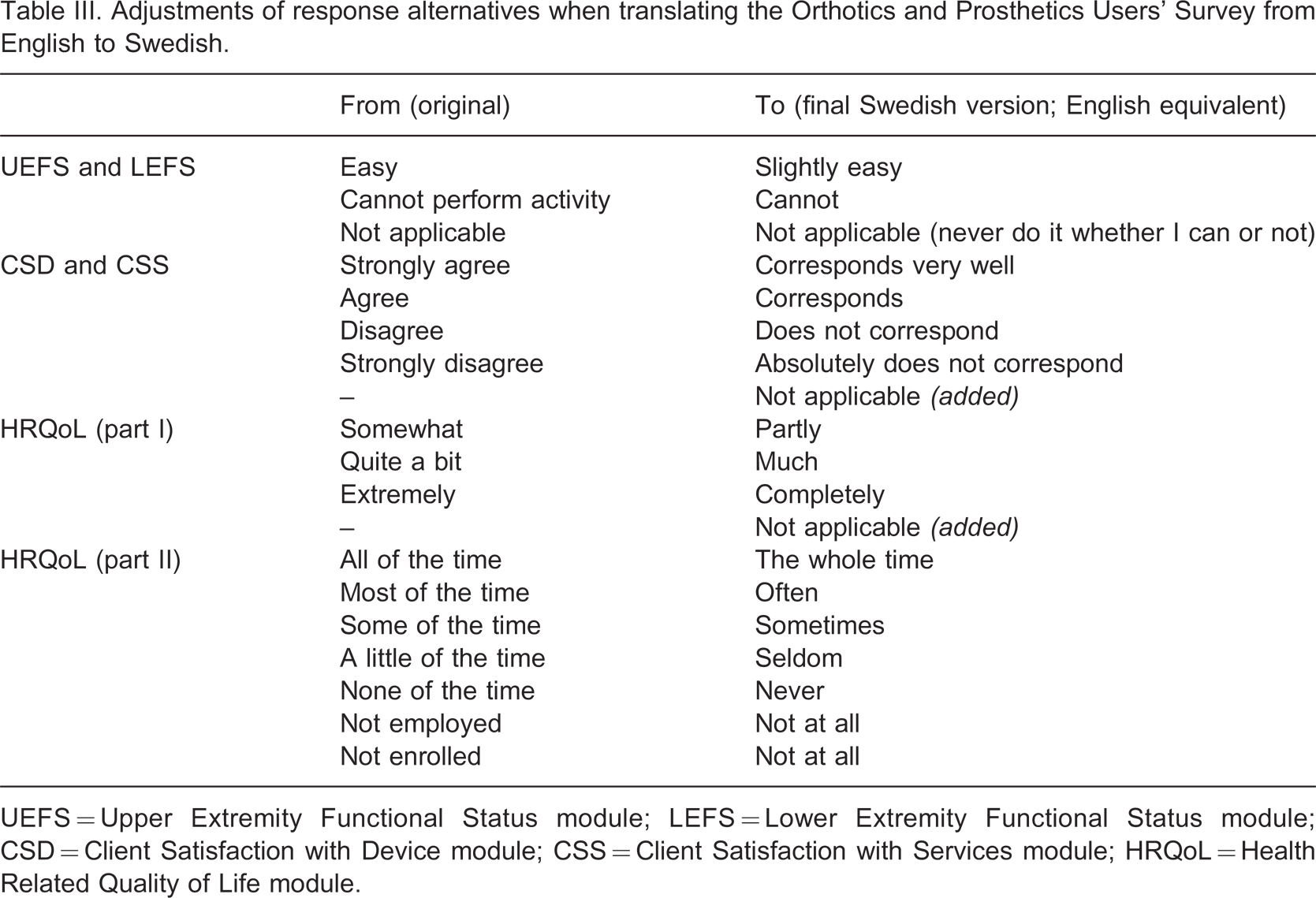
UEFS = Upper Extremity Functional Status module; LEFS = Lower Extremity Functional Status module; CSD = Client Satisfaction with Device module; CSS = Client Satisfaction with Services module; HRQoL = Health Related Quality of Life module.
Discussion
In the present study OPUS was translated from English into Swedish and the Swedish version was tested on Swedish O&P clients. The main finding was that the Swedish version of OPUS (OPUS-Swe) was understood by the clients as intended.
The translation procedure chosen for this study (Figure 1) is well known and frequently used. According to the WHO translation guidelines, 13 one person should translate the instrument into the new language. We chose to follow other recommendations, 12,15 claiming that using more than one translator, who translate the instrument independently of each other, increases the validity of the translation. The forward translators of OPUS were of different health professions, which we consider advantageous, as they all contributed with a unique perspective. Some studies have involved lay-persons in the forward translation 24 to ensure that the language of the translation is everyday. This was not practised in the present study, but a cognitive debriefing of the respondents was performed, at which inappropriate expressions could be identified.
The back-translation technique has been recommended as a way to identify weaknesses in the forward-translation. 15 This was also shown in the current study, where the back-translation demonstrated that several linguistic corrections of the OPUS-Swe were necessary in order to come closer to the original text.
During the interviews the person's answers were recorded in writing by the interviewer. This limited the amount of data that could be collected compared to if audio recording had been used. However, as the intention was to study the linguistic understanding of the items and not to make a qualitative analysis we consider the technique used to be appropriate.
The WHO 13 recommends that respondents at a cognitive debriefing should be representative of the persons to whom the test will be administered. In the present study the respondents were representative of most O&P clients regarding the devices used (Table I) and of the age range. However, only 12 of the 39 respondents were male, a fact which might jeopardize the linguistic validity of OPUS-Swe for men. Nevertheless, three men answered each module of OPUS and thus the male perspective was not lost for any of the modules.
To achieve a translation that is conceptually equivalent to the original it is necessary to consider semantic, experiential, and idiomatic equivalence. 12 Several adjustments of OPUS-Swe were related to semantic equivalence, and necessitated by the inherent differences between the Swedish and English languages. A few adjustments were related to experiential equivalence. For instance, “open door with knob” (UEFS) was translated as “open door with door handle”, as door knobs are not used in Sweden. Further, Swedish O&P clients seldom purchase their device, but often pay a fee for the visit and the device, and therefore the statement “I can afford the out-of-pocket expenses to purchase and maintain my prosthesis/orthosis” (CSD) was translated as “I can afford the expenses of obtaining and maintaining my assistive device”. Finally, one adjustment of OPUS-Swe was related to idiomatic equivalence. Three respondents found the idiom “full of life” (HRQoL) hard to understand when translated literary and, therefore, it was changed to the Swedish idiom “livsglädje” (“joy of living”).
The linguistic validation also revealed complicated linguistic constructions in the OPUS-Swe. In three items a double negation, i.e., negation in both the question and the response alternative, appeared in the CSD module. This was changed, as it was pointed out by two respondents and resulted in one respondent giving the opposite answer to what she intended. Without the interviews this might have been overlooked and could have resulted in future problems with the use of OPUS-Swe. Linguistic validation can thus be recommended not only for translations but also for development of new instruments.
It is important to ascertain that the respondents will understand not only the items themselves but also the introductory text in a questionnaire, and use the questionnaire as intended. In this study the results from the linguistic validation showed that some of the wordings were misunderstood, and hence they were changed in the final Swedish version.
Like the other modules of OPUS, the LEFS module was originally developed for orthotic and prosthetic users and not for users of orthopaedic shoes and insoles, the latter often being persons in relatively good physical condition. Thus, on the basis of clinical experience a high ceiling effect can be expected from the low demands of the LEFS module items. Hence, new items including more demanding activities in the LEFS module are needed. These could include activities such as participating in strenuous sports, jogging, standing up for a longer time, visiting shops, or standing and walking during a working day.
Testing of a translated instrument has both qualitative and quantitative aspects, 15 in that the tests should cover both the linguistic validity and the psychometric properties of the new version. The OPUS-Swe showed linguistic validity, but linguistic equivalence with the original English version does not guarantee psychometric equivalence. 25 Hence the psychometric properties of OPUS-Swe need to be tested, and work is presently underway for assessing its internal validity and test-retest reliability.
Conclusion
In conclusion, the Swedish version of OPUS is linguistically valid for persons using orthoses, prostheses, shoe insoles, or orthopaedic shoes. It is a promising tool that is applicable to the Swedish O&P field. However, further tests of the psychometric properties of the Swedish version are needed before it can be implemented.
Footnotes
Acknowledgements
We acknowledge the valuable help from the developer of OPUS, Professor Allen W. Heinemann, Feinberg School of Medicine and Rehabilitation Institute of Chicago, Chicago, USA. We also acknowledge the contributions of the translators: Lis Sjöberg, Registered Occupational Therapist, Limb Deficiency and Arm Prosthesis Centre; Inga Röhfors, Registered Physical Therapist, and Sven-Arne Jakobsson, Orthopaedic Surgeon, at the Department of Orthopaedics; Örebro University Hospital, and Neda Razavy, Certified Prosthetist and Orthotist, Department of Prosthetics and Orthotics, Örebro County Council, Sweden. We extend our thanks to all the clients who participated in this study. This study was supported by grants from the Centre for Rehabilitation Research and the Research Committee, Örebro County Council, Sweden and the Norrbacka-Eugenia Foundation, Sweden.
Acknowledgements