
Abstract
This phase 1 exploratory study aimed to establish proof of concept of the effects of dynamic elastomeric fabric orthoses (DEFOs) on the gait of children with spastic diplegic cerebral palsy. Replicated single case experiments employing an ABA methodology were carried out on eight subjects (median age 5.5 years, range 3–13 years; 4 girls/boys) utilizing quantitative/qualitative data collection. Outcome measures were: Ten metre walking test (10MWT); physiological cost index (PCI); visual analogue scale (VAS) scoring of perceived gait changes; functional mobility changes using Patient Specific Functional Scale (PSFS); subject/carer perceptions recorded in daily diaries. Results identified following analysis of quantitative data indicated a treatment effect from the orthoses which could be corroborated by participant subjective impressions and comments. Statistically significant (p < 0.05) intervention-related improvements in gait velocity and gait consistency were identified respectively in 5/8 and 4/8 subjects. Power calculations support the feasibility of a larger controlled study to further investigate this orthotic intervention. This study indicates that DEFO leggings can confer beneficial effects on the gait of some children with spastic diplegia resulting from CP. These findings have implications for orthotic intervention with this subject group.
Introduction
In Western Europe, the incidence of cerebral palsy (CP) is between 2–3 cases per 1000 live births, 1 a key cause of childhood physical disability in this region. Around 22% of CP cases present with spastic diplegia of varying severity, often influencing the child's gait. 2 Orthotic intervention is well documented for this subject group. 1
Dynamic elastomeric fabric orthoses (DEFOs) have been used internationally since the early 1990s. Although specific construction and prescription varies between manufacturers and orthotists, they consist essentially of bespoke close-fitting orthoses constructed from Lycra® or similar elastomeric fabrics, tailored to fit the affected body part(s). It is proposed that these orthoses exert a paratonic torsional and compressive effect to positively influence alignment, biomechanics and neuromuscular activity. 2 There is a growing body of literature contributing to evidence of their effectiveness: A recently conducted literature review covering the period 1993–2008 identified seven case-controlled studies, 12 single case studies and two MSc research theses. 3 Improvements in function, range of movement and thoracic stability, 3–5 as well as dynamic musculoskeletal correction, 6,7 have all been reported. Studies have evaluated the effects of DEFOs with respect to the functional problems of children with CP. 6,8 However, no studies have investigated the effects of DEFOs on the lower limbs, specifically during the treatment of spastic diplegic gait associated with CP.
The primary aim of this research was to conduct an exploratory study in an everyday clinical context to identify gait and mobility-related changes in a group of CP children who had been prescribed DEFO leggings. An exploratory study carried out in a clinical context imposed some limitations on the outcome measures used, requiring evaluative procedures which would fit easily into routine clinical practice. The study was intended as a phase 1 Medical Research Council (MRC) ‘proof of concept’ evaluation, 9 and a further goal was to evaluate the feasibility of a later stage controlled clinical trial.
Method
A multiple single-case report methodology was approved by UK COREC ethical committee (MREC04/1/022). Eight subjects (with existing orthotic and walking aids) were evaluated using a replicated single case experimental design (SCED) which is considered a pertinent means for conducting exploratory evaluations of the effects of novel interventions on single individuals. 9 External validity of several replicated single case experiments results is increased, providing researchers with preliminary impressions of probable treatment effects, whilst potentially providing indicators for further controlled clinical trials. This approach has previously been used successfully in similar paediatric contexts 10 to establish specific innovative therapeutic interventions. 9
The specific SCED used with each subject in this study followed the established tri-phase ABA reversal format. 11 The initial baseline (A1) observation phase aimed to identify the typical baseline performance characteristics of each subject. In the subsequent intervention (B) phase, the intervention was introduced, with continuing monitoring of subjects' performance. In the final baseline (A2) phase, the intervention was withdrawn, whilst subject monitoring still continued. This ABA methodology was intended to permit identification of any performance changes coincident with introduction and/or withdrawal of intervention, and also to provide opportunity for evaluation of persistency of effect (carry-over) once the intervention was withdrawn. An intervention (B) phase length of six weeks was chosen, being commensurate with anticipated progress periods based on clinical experience. Similar length adjacent baseline (A1 and A2) phases were then used. Thus there was an 18-week evaluation period in total for each subject.
Outcome measures
Previously validated outcome measures relating to aspects of gait performance and physical functioning which were comparatively simple and readily applicable in a clinical situation were selected. Frequency and nature of testing was based on individual outcome measure characteristics as well as feasibility and practicality of repeated testing. Each subject agreed to attend weekly for the 18-week period of evaluation, hence weekly testing where appropriate was feasible. Outcome measures were:
Ten Metre Walking Test (10MWT).
12,13
This standardized method for evaluating gait velocity establishes a walking time mean value over three walks of 10 m, and was conducted weekly by each subject's primary physiotherapist. Visual Analogue Scale (VAS).
14
Scoring of perceived changes in gait in relation to previous week's performance was made by each subject's main carer. Physiological Cost Index (PCI),
15,16
a derived quotient of energy expenditure during gait, was calculated using walking time data plus resting/post-walking pulse rates
∗
obtained during the 30-m walking of the 10MWT test. Conducted at the last measurement of walking time in each six-week phase by the principal researcher (MJAM). Patient Specific Functional Scale (PSFS),
17
a key mobility-related functional goal was identified for each child and scored by his/her primary physiotherapist on a 0–10 point VAS, at the end of the A1 and B phases. The wide variation in abilities of this patient group was recognized in the selection of an individual functional task for each subject. In addition to these quantitative evaluations, subjects/carers were encouraged to keep a daily diary, recording perceived salient features of mobility during their 18-week involvement in the study. They also recorded the total number of hours of orthotic wear each day during the intervention (B) phase.
Intervention
A bespoke pair of DEFO full length leggings was prescribed for each participant, constructed according to typical recognised criteria currently in UK clinical use. † The orthoses were constructed from polyester/lycra fabric incorporating de-rotative, compressive panels to initiate external rotation and abduction of the lower limbs, coupled with knee extension and pelvic compression (Figure 1). It was expected that these orthoses would be worn for approximately 8 hours per day during waking hours, in keeping with current clinical practice.

Shows the anterior and posterior view of the dynamic elastomeric fabric orthotic (DEFO) leggings.
Subjects
Patients with spastic diplegic gait as a result of cerebral palsy, aged between 3 and 16 years, were recruited into the study. Inclusion crieria were: A typical crouch pattern of gait as described by Gage; 18 under the care of a physiotherapist and already attending (or able to attend) for weekly assessment; able and motivated to walk, with or without walking aids, for a minimum of 30 (3 × 10) m. Exclusion criteria were those who were wheelchair dependent, had fixed lower limb contractures, had recent surgical intervention or botulinum toxin treatment within the last nine months, and excessive tibial torsion (greater than 20° by visual inspection).
Eight participants were recruited to the study from three treatment centres. Median age of participants was 5.5 years (range 10 years, minimum three years, maximum 13 years); ratio of males to females was equal.
Analysis was primarily via visual inspection of graphical presentations of data, looking for inter-phase changes in trend, level, slope and variability. 11 Inferential statistical analysis of each subject's results was also conducted where weekly repeated measures gave continuous data; e.g., 10MWT results. This latter analysis utilized the celeration line method as described by Ottenbacher. 19 Additionally power calculations to inform a potential future controlled clinical trial were undertaken.
Results
Ten metre walking test (10MWT)
Results for changes in walking time across the 18 weeks of the evaluation, were mixed, although a pattern could be identified. Figure 2 (left side) illustrates performance trends for walking time for all eight subjects across the three phases of the trial. An overall reduction (i.e., improvement) in walking time values leading up to and/or during the intervention phase is suggested. A reduction in walking time suggests that the subject is more controlled and walking within their base of support. Some subjects' values increased (i.e., worsened) when the intervention was withdrawn, although there were variations in this pattern.
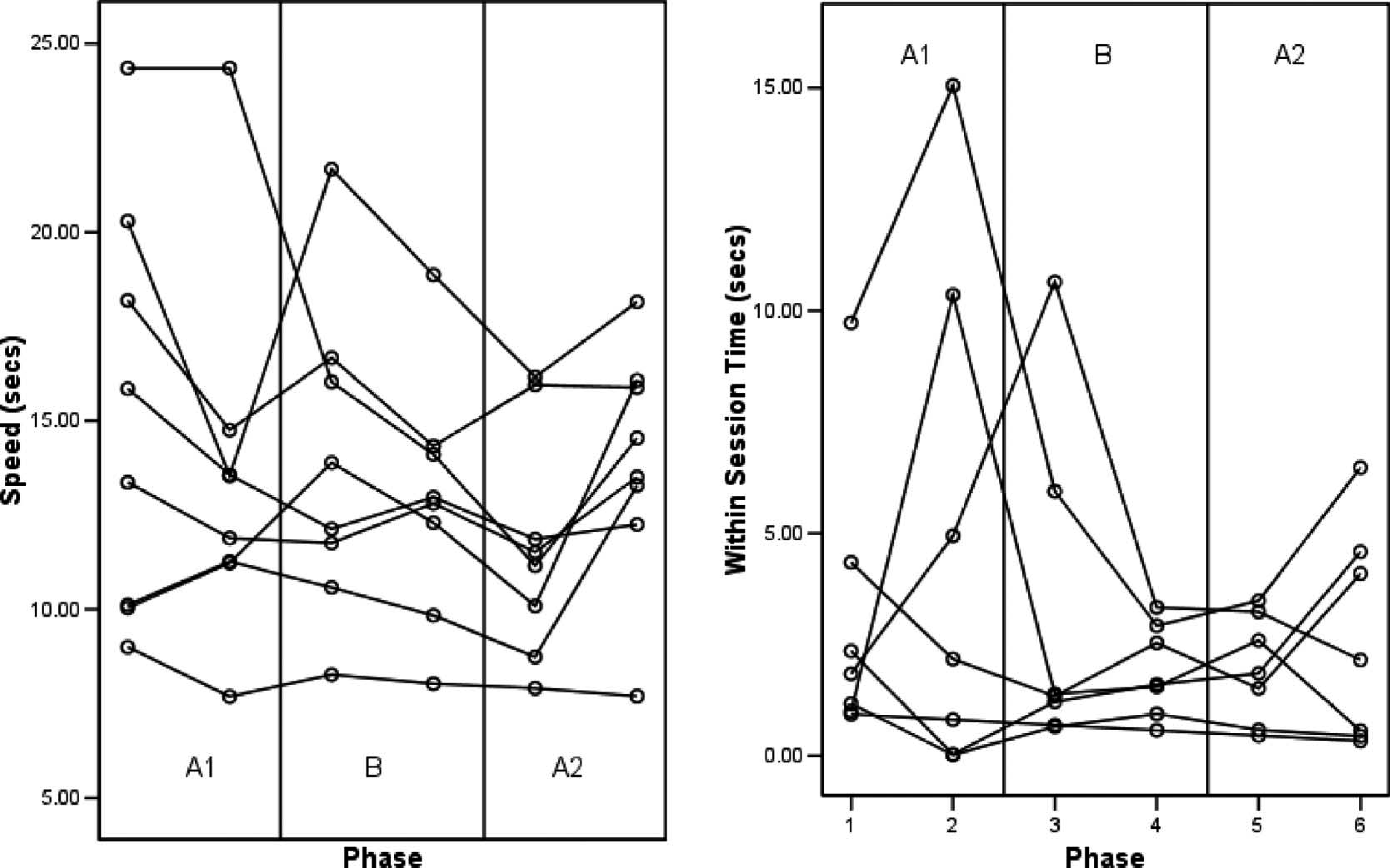
This shows the time taken to complete the 10MWT (left side) and shows that all participants changed when the leggings were applied; however, the changes are not uniform. The within test variation (right side) shows a reduction in the variance values over the three walks suggesting.
Additional post hoc analysis of the 10MWT data gave further indications of possible treatment effects. Analysis of within-session walking time variation values, across all assessment sessions, indicated a small treatment effect: Figure 2 (right side) illustrates the trends for the amount of variation in walking time on each occasion of testing, for all eight subjects. The within-session walking time variation was calculated from the difference between the slowest and fastest times recorded of the three 10 m walks required to obtain the PCI value. The subjects became increasingly more consistent in their performance (i.e., less variability in walking time), by the end of the intervention phase. A carry-over of this effect into the next (A2) phase, when the intervention was withdrawn was also identified.
Both of these data sets were subject to interferential statistical analysis using the celeration line method, common in single case design studies. Five of the participants showed statistically significant changes (p < 0.05) in walking time between the A1 and B phases. Four of the participants showed statistically significant changes (p < 0.05) in walking time variation between the A1 and B phases.
Visual Analogue Scale (VAS)
Figure 3 (left side) illustrates a trend for cumulative perceived improvement in walking performance, as scored by seven of the subjects' main carers. The anticipated static and level scores of the initial baseline (A1) phase were increased for these subjects when the intervention was introduced, suggesting an improvement in gait performance.
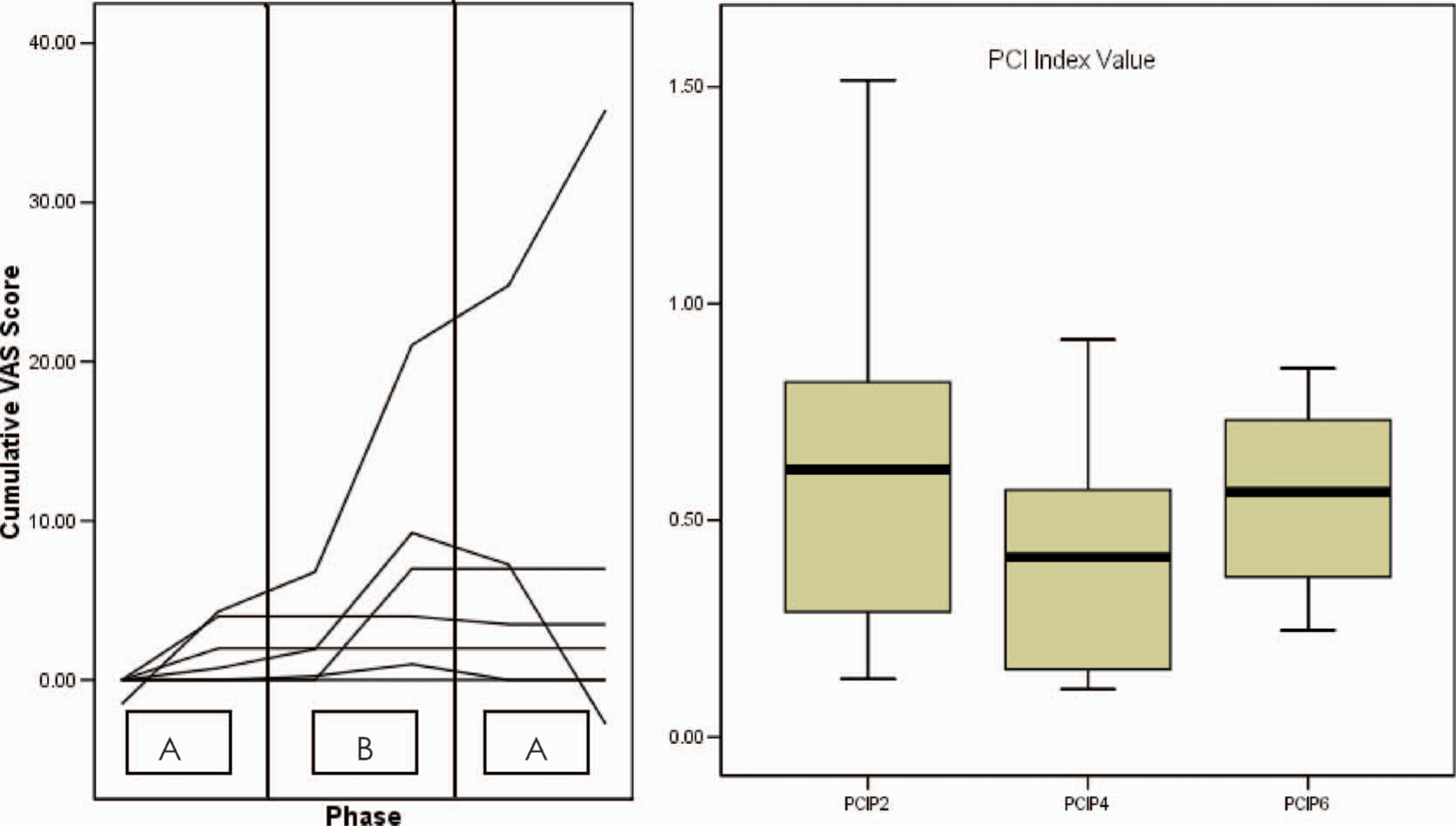
This shows the perceived change in gait (left side), when the leggings were applied. The Physiological Cost index values (right side) indicate the overall effect of the legging intervention in the ‘B’ phase. The median line shows a reduction in the index value, due to the intervention.
Physiological Cost Index (PCI)
PCI values were calculated for each subject, based on the final assessment of walking time at the end of each of the three phases of the study. Figure 3 (right side) summarizes these PCI values across all eight subjects at each of these three points in time. A broad range of values is shown by the end of the initial (A1) baseline phase. Values are less variable as well as lower (i.e., improved) across the group by the end of the intervention (B) phase. PCI values increased slightly (i.e., worsened) during the second baseline (A2) phase, although were less variable across the group than in either of the preceding phases. These data suggest an intervention effect, specifically that the orthosis had a positive influence on the physiological cost of walking. This effect is indirectly reflected in Figure 2 (right side), wherein walking velocity is seen to be progressively more consistent with time.
Patient Specific Functional Scale (PSFS)
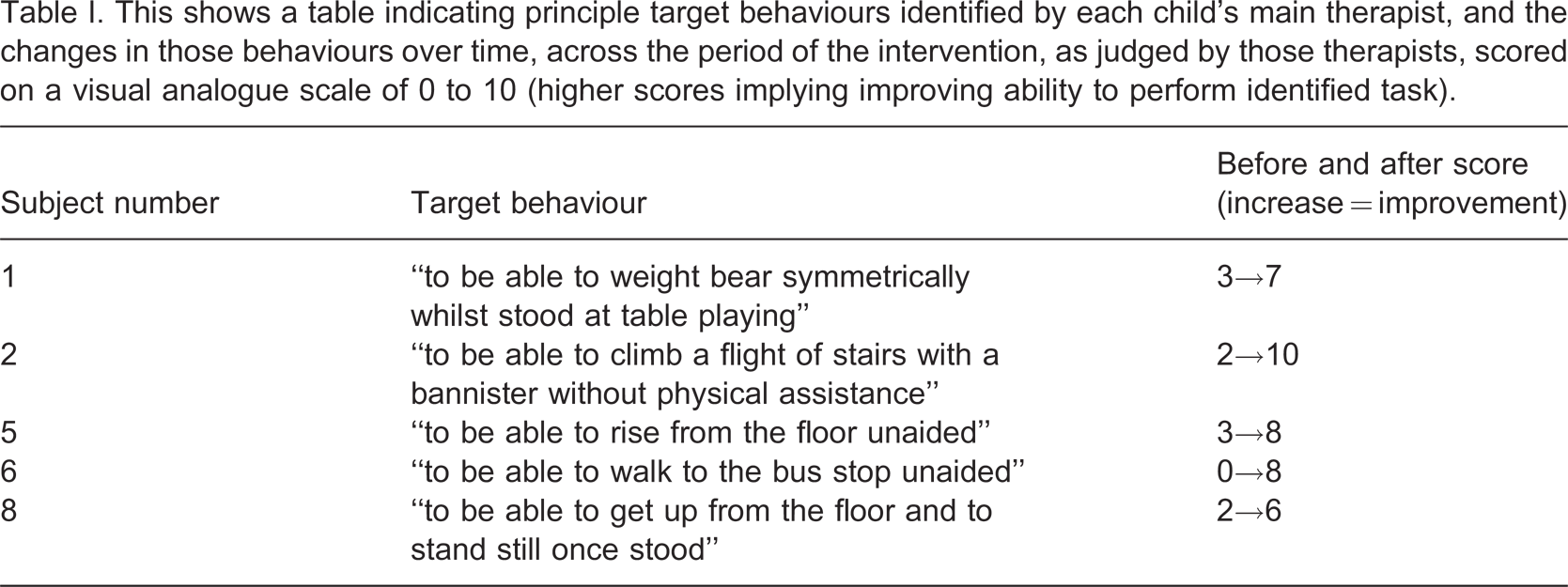
PSFS assessment was carried out for five of the eight subjects. (Clinicians in one of the three study centres chose not to use this outcome measure with their three subjects, because of time constraints.) Table I illustrates the primary target behaviours selected for each subject, together with the scores given by his/her primary physiotherapist, before and after the intervention. The median VAS change was 5 points with a range of 4 points (minimum 4 points, maximum 8 points). In all five instances the subjects were judged by their physiotherapists to have improved in their ability to perform their identified functional task.
This shows a table indicating principle target behaviours identified by each child's main therapist, and the changes in those behaviours over time, across the period of the intervention, as judged by those therapists, scored on a visual analogue scale of 0 to 10 (higher scores implying improving ability to perform identified task).
Daily diary reports
Seven of the subjects' carers maintained daily diaries relating to gait function and orthotic wear during the trial. Content analysis of diary comments was carried out. 20 Themes of change, identified in the data from the intervention (B) and withdrawal (A2) phases, included alterations in gait and altered confidence levels. Perceived changes in fatigue level, improved gait and confidence corroborated the results of the PCI and thus appeared to endorse a treatment effect. A limited number of comments were made on soreness to thighs from increased heat and difficulty in don and doff of leggings.
The mean number of hours the leggings were worn per day across the eight participants was 6.9 h (range 2.6–11.6 h).
Power calculation
The PCI and 10MWT values were used to undertake power calculations for a larger controlled group study. A difference between the ends of the A1 and B phases of 0.22 of the PCI index with a standard deviation of 0.50 indicated that 43 subjects would be required to obtain 80% power at the 5% significance level. Within-session performance variation values obtained from the 10MWT indicated a difference between the ends of the A1 and B phases of 0.28, which with a standard deviation of 0.50 indicated that 30 subjects would be required to obtain 80% power at the 5% significance level.
Discussion
Overall the results of this small exploratory study of eight subjects provide provisional support that DEFO leggings can have beneficial effects on the gait of some children with spastic diplegia. Positive changes in walking time and physiological cost were identified in the gait of some subjects. Intervention-related positive changes were reflected in carers' subjective ratings of performance, as well as in ratings of changes in mobility provided by the physiotherapists. Daily diary accounts maintained throughout the study provided further corroborative information.
The design of the study has provided a relatively in-depth evaluation of changes seen in each of the subjects. Although a somewhat limited range of outcome measures were used, data from two measures have permitted power calculations to be undertaken which support the feasibility of a larger controlled study.
The daily activities of each child over the period of study were not constrained in any way. Identification of changes in gait and mobility in a natural clinical setting were the explicit target of the intervention. Participants were not blinded to treatment delivery, which would require a sham orthosis as part of a more complex intervention. It is acknowledged that effects of expectation and motivation may have an influence on the functional changes observed during data collection and the changes identified by physiotherapists' subjective scoring of functional change. There is a growing evidence base for effectiveness of upper limb and trunk orthoses on movement control 2 through a number of probable effect mechanisms which include an elongation of shortened soft tissues 21 combined with a torsional corrective effect on inappropriately aligned limb and body segments; 7 an external supportive ‘exoskeleton’ effect in instances of muscle weakness and inadequate muscular control and motivational, educational and sensory effects.
It seems probable that DEFO leggings contributed some degree of supportive, facilitative and educational influence on the movement patterns of those involved in this study, resulting in some of the changes noted. Further specific research is needed to endorse these findings. Utilizing an objective evaluation of visible changes in movement quality during intervention could be considered, although quality of movement remains difficult to quantify objectively 22 in a natural clinical setting. Evaluation of child height and weight to calculate body mass index (BMI) values for participants could explore potential relationships that may be suggested by an additional observation that subject age/size appeared to have some influence on the nature of the changes seen in walking velocity and movement efficiency during treatment.
In clinical practice, orthotic treatment of spastic diplegia typically forms part of a sophisticated complex intervention delivered by a therapeutic multi-disciplinary team. Physical treatment may include a combination of targetted exercise and training, advice, orthotic prescription, and surgical intervention where required. This study sought to establish preliminary proof of concept with respect to orthotic intervention. The effectiveness of strengthening exercises in CP management is increasingly recognized, 23 specifically in the treatment of spastic diplegic crouch gait. 24 Evidence for the effectiveness of targetted dose-specific physiotherapy is also emerging. 25 The extent to which DEFOs might achieve enhanced clinical effectiveness when applied as part of an ongoing multi-faceted intervention therefore also merits further investigation.
Conclusion
The outcome measures along with the subjective observations of participants, carers and physiotherapists together suggest that wearing DEFO leggings can have a clinical effect on the gait of children with spastic diplegia. This exploratory study adds to the growing body of evidence to support continuing investigation of the efficacy of DEFOs for movement disorders. ‘Proof of concept’ evaluation has been carried out to propose that further work is needed now to evaluate the use of leggings in the management of diplegic gait in children with cerebral palsy to identify definitively the contribution of this intervention to their neuro-motor development.
Footnotes
Acknowledgements
Thanks are extended to the children, parents, carers and clinicians who agreed to participate in this study, D.M. Orthotics Ltd (who provided the leggings free of charge), Dr Allan Clark, (medical statistician) and Drs Penny Butler, Richard Reading and Fiona Poland for their support throughout the research.
Acknowledgements
∗Physiological Cost index was calculated by dividing the heart rate immediately after the 10MWT exercise minus heart rate at rest by m per min. 15
†D.M. Orthotics Ltd, Tescan Units, Wilson Way, Pool Industrial Estate, Redruth, Corwall, UK.