
Abstract
Ambulation on stairs presents a significant challenge for lower extremity amputees and increases the risk of falling and sustaining a serious injury. This study aimed to compare foot placement and foot clearance during stair ambulation in a group of transtibial amputees and a group of able-bodied subjects. Three-dimensional motion analysis was used to determine foot positioning and to calculate temporospatial parameters during stair ascent and descent of 10 transtibial amputees (mean age = 56) and a control group consisting of 10 healthy able-bodied individuals (mean age = 26.7). No significant difference was observed in foot positioning and foot clearance between the amputee and control groups. Temporospatial data revealed a number of significant differences between the groups, particularly during stair ascent. Amputees were observed to walk with a slower velocity and cadence (p < 0.01), to increase the time spent in stance phase and double support (p < 0.01) and to increase their step width during both stair ascent and descent (p < 0.01). Results suggest that foot placement and clearance are not factors that would contribute to a stumble or fall on stairs in established amputees but that balance related issues, such as relative motion of the centre of mass, require further investigation.
Introduction
Lower limb amputees have been demonstrated to be at an increased risk of falls and fall related injuries. 1 Negotiation of stairs and raised surfaces presents as a significant challenge for lower extremity amputees and increases the risk of trips and falls to an even greater extent. In order to reduce the risk of falls from stairs it is first necessary to identify gait characteristics that differ between amputees and able-bodied persons. Foot positioning on the step and foot clearance of the swinging limb are variables that have not previously been investigated in this population and may provide insight as to why amputees are at a greater risk of falling from stairs than when walking on a flat level surfaces.
Previous research has indicated that specific foot placement strategies when negotiating obstacles are a key determinant of safety during ambulation. 2 The risk of falling or tripping on stairs has been linked to foot placement relative to the edge of the step by the target foot and foot clearance by the trailing leg. 3 It has also been demonstrated that unwanted foot contact is more likely during stair descent. 3 Recent literature involving elderly adults has examined foot placement strategies while negotiating stairs and raised surfaces. These studies have demonstrated that this population, who have previously been demonstrated to be at an increased risk of falls, place the feet closer to the edge of the step during both ascent and descent when compared to a young healthy population and that they clear the step by a lesser margin. 2,3
Safety during ambulation has also been linked to temporospatial variables. It has been suggested, for example, that gait velocity is linked to the ability to recover stability after a loss of balance as a faster moving centre of mass can enable a person to quickly catch up with a forward slipping foot. 4 Additionally, an increased step width and a decreased cadence have been noted in subjects who present with compromised stability. 5,6
Investigations of transtibial amputees have examined kinematic compensations made during stair ambulation. 7,8 These findings suggest that the limited range of ankle motion in the prosthesis forces the amputee to make kinematic compensations at more proximal joints. While this information could be used to infer differences in foot placement strategies and clearance of the swinging limb between transtibial amputees and able-bodied subjects, to date there is no literature quantifying if this is actually the case.
The goal of this study was to investigate the foot placement strategies used by amputees during stair ascent and descent and compare them to a healthy able-bodied population. A secondary goal was to compare temporospatial parameters of gait during stair ambulation. Specific temporospatial parameters under investigation included; velocity, cadence, base of support, stance duration, swing duration and double support time. We hypothesized that during stair descent amputees would place their prosthetic stance limb closer to the edge of the step to facilitate rollover of the prosthetic foot. We further hypothesized that reduced proprioceptive feedback from the prosthetic side would result in the amputee clearing the step with the swinging limb to a greater extent than the able-bodied subjects. Amputees were expected to ambulate with a reduced velocity and cadence, to walk with a wider base of support and to increase the time spent in stance and double support.
Methods
Subjects
An amputee sample including 10 transtibial amputees and a control group consisting of 10 able-bodied subjects were recruited for the study. Median age of the amputee group was 56 (range 33–67 years). The mean latency since amputation was 19 years (range 5–48). Median age of the control group was 26.7 years (range 20–37). Amputees were selected on the basis that they were active and established prosthetic users, scored a minimum of 12 on the Stair Assessment Index, 9 typically use a reciprocal gait pattern during stair ascent and descent and had not suffered any physical or neurological injury that may affect their ability to ambulate safely. Controls were selected on the basis that they had no physical or neurological problem that may affect their ability to ambulate stairs safely. All protocols were approved by the regional ethics board in Linköping, Sweden, prior to commencement of the study.
Data collection
An experimental staircase was constructed consisting of five steps in total with a rise of 17 cm, a run of 29 cm and a 2-m walkway extension at the top. The dimensions of the stairs were based on guidelines proposed by SÜVA 10 and were constructed to be typical of most stairways in Sweden.
Reflective markers were placed on the top edges of the third step to mark the support surface. Markers were also placed on the participants' shoes at a height of 1.5 cm from the floor on the posterior aspect of the heel counter, the estimated position of the 1st metatarsal (Mt1) and the estimated position of the 5th metatarsal (Mt5). Positions of Mt1 and Mt5 on the prosthetic foot were determined by estimating the position from the sound side. An additional marker placed at the level of the sacrum was used to calculate walking velocity. Subjects were requested to walk along a 3-m level walkway and then to ascend the stairs. After a short pause they were then requested to descend the stairs. All stair-climbing activities were performed at a self-selected walking velocity. For safety reasons, subjects were informed that they may use the hand-rail if needed; however, no subjects chose to do so. In order to collect data from both the left and right feet as they contacted the third step, subjects were requested to alternate their starting foot on the first step.
A six-camera motion analysis system (Qualisys Medical AB) was used to capture data concerning the position of the foot relative to the third step together with temporospatial data as the subject ascended and descended the staircase. Cameras were calibrated to a volume of 3 m3. All calibration errors were below 1.5 mm. Kinematic data was sampled at 60 Hz. For each of the walking conditions (ascending and descending), one representative trial from each foot was selected for analysis. Marker position data was lowpass filtered using a second order Butterworth Bidirectional Filter with a cut-off frequency of 6 Hz.
Visual 3D software (C-Motion Inc) was used for data processing. Figures 1 and 2 show the specific foot position variables extracted for analysis for stair ascent (Figure 1) and stair descent (Figure 2). During stair ascent, variables extracted for analysis included the horizontal distance of the heel marker of the stance foot from the edge of the stair when the foot was flat on the ground (a), the vertical distance of the Mt1 marker and the heel marker of the swinging limb as it passed over the edge of the stair (b & c) and the horizontal distance of the Mt1 marker of swinging limb from the edge of the stair at the point in time that the stair marker and the Mt1 marker are at the same vertical height (d). During stair descent variables collected for analysis included the horizontal distance of the Mt1 marker from the edge of the stair when the foot was flat on the ground (e), the vertical distance of the Mt1 marker and the heel marker of the swinging limb as it passed over the edge of the stair (f and g) and the horizontal distance of the heel marker of the swinging limb from the edge of the stair at the point in time that the heel marker and the stair markers are at the same vertical height (h). When determining foot placement data from the stance foot it was possible that the foot was not fully placed on the step and that the heel (during ascent) or toes (during descent) would be hanging over the edge of the stair. To control for potential errors associated with this, measurements were taken at the point in time at which a line joining the heel and toe markers was parallel to the Y axis of the laboratory and to the top surface of the step.
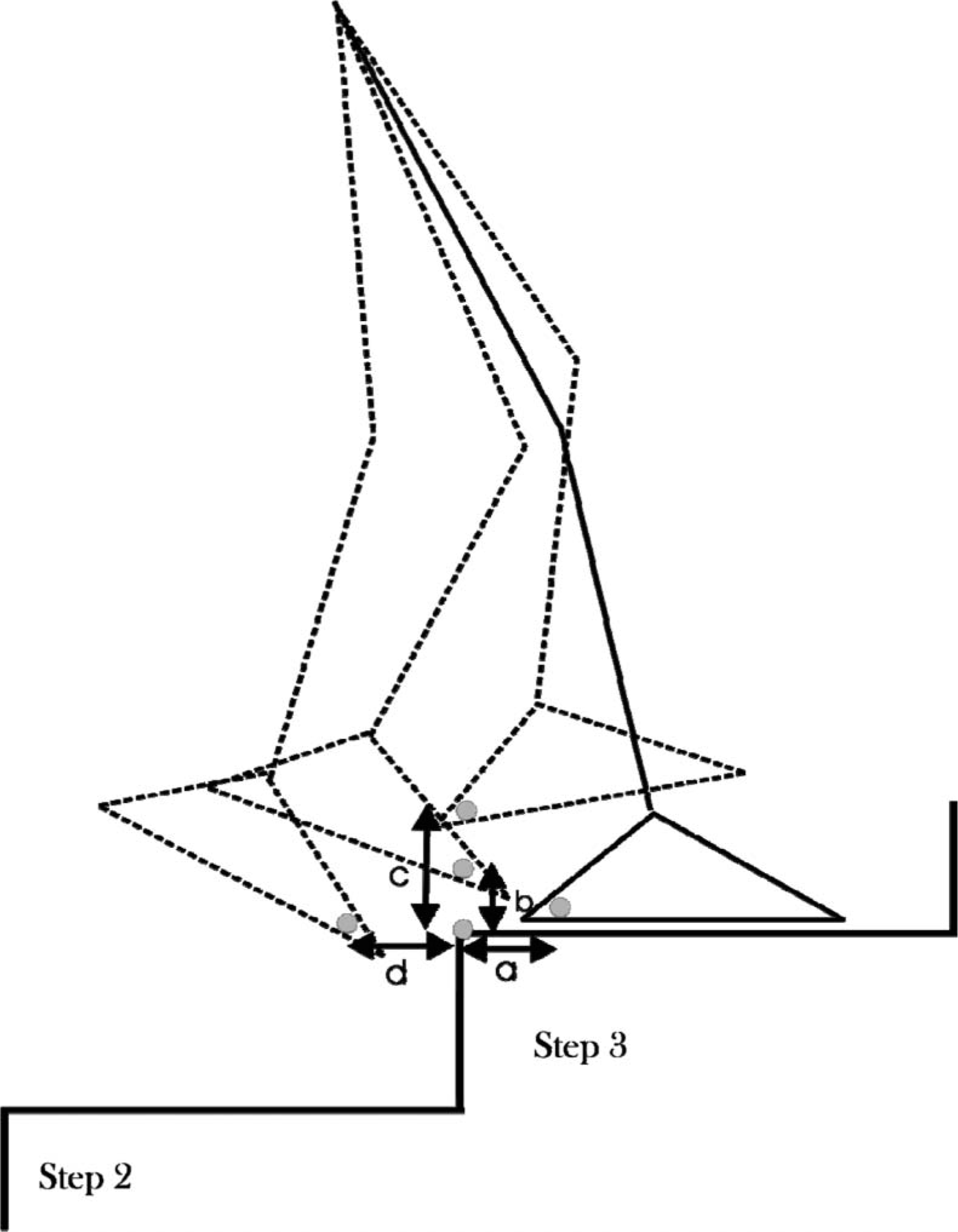
Diagram showing the outcome variables for the stair ascent condition. Solid line depicts stance foot and dashed line depicts swinging limb. (a) Horizontal distance of stance foot heel marker from the step edge markers. (b and c) Vertical distance of Mt1 marker (b) and heel marker (c) as they pass over the step edge markers; and (d) horizontal distance of Mt1 marker from the step markers when both markers are at the same vertical height.
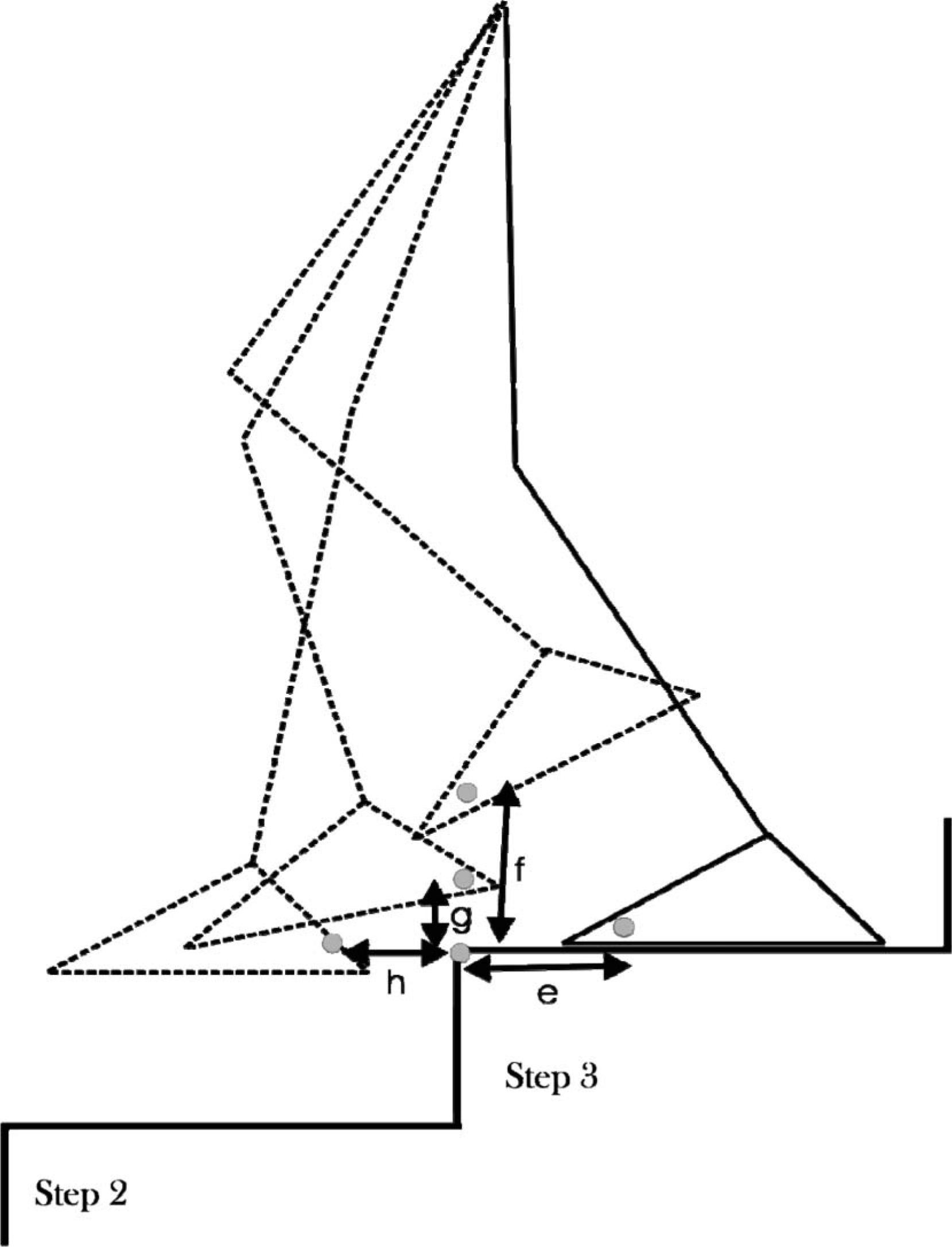
Diagram showing the outcome variables for the stair descent condition. Solid line depicts stance foot and dashed line depicts swinging limb. (e) Horizontal distance of stance foot Mt1 marker from the step edge markers. (f and g) Vertical distance of Mt1 marker (f) and heel marker (g) as they pass over the step edge markers; and (h) horizontal distance of heel marker from the step markers when both markers are at the same vertical height.
Gait cycle duration was determined as the time from initial contact of the foot on the third step to the subsequent initial contact of the same foot on the next step. Cadence was calculated as the number of steps per minute. Stance phase duration was determined as the time from initial contact to the point in time at which the foot was determined to leave the step. Swing phase duration was calculated as the time between toe off to the instant in time when the same foot contacted the next step. Both stance and swing phase were expressed as a percentage of the total gait cycle duration. Double support time was defined as the proportion of the gait cycle in which both feet were in contact with the stairs. For ascending trials, toe markers were used to determine when the foot was contacting and leaving the step. For descending trials, when it was possible that the toe marker was hanging over the edge of the step, the heel marker was used to determine when the foot contacted and left the step. Step width was calculated as the distance between the left and right heel markers when the foot of interest was contacting the third step and the contralateral foot was in contact with the subsequent step.
Data processing and statistical analysis
Data was tested for violations to the assumption of normality using the Shapiro-Wilk test. A paired t-test was used to compare results obtained from the amputees' sound and affected sides while an independent t-test was used to compare amputees to the control group. Statistical analysis was performed using SPSS statistical analysis software (version 14.0 for Windows). The alpha level for determining statistical significance was p < 0.05.
Results
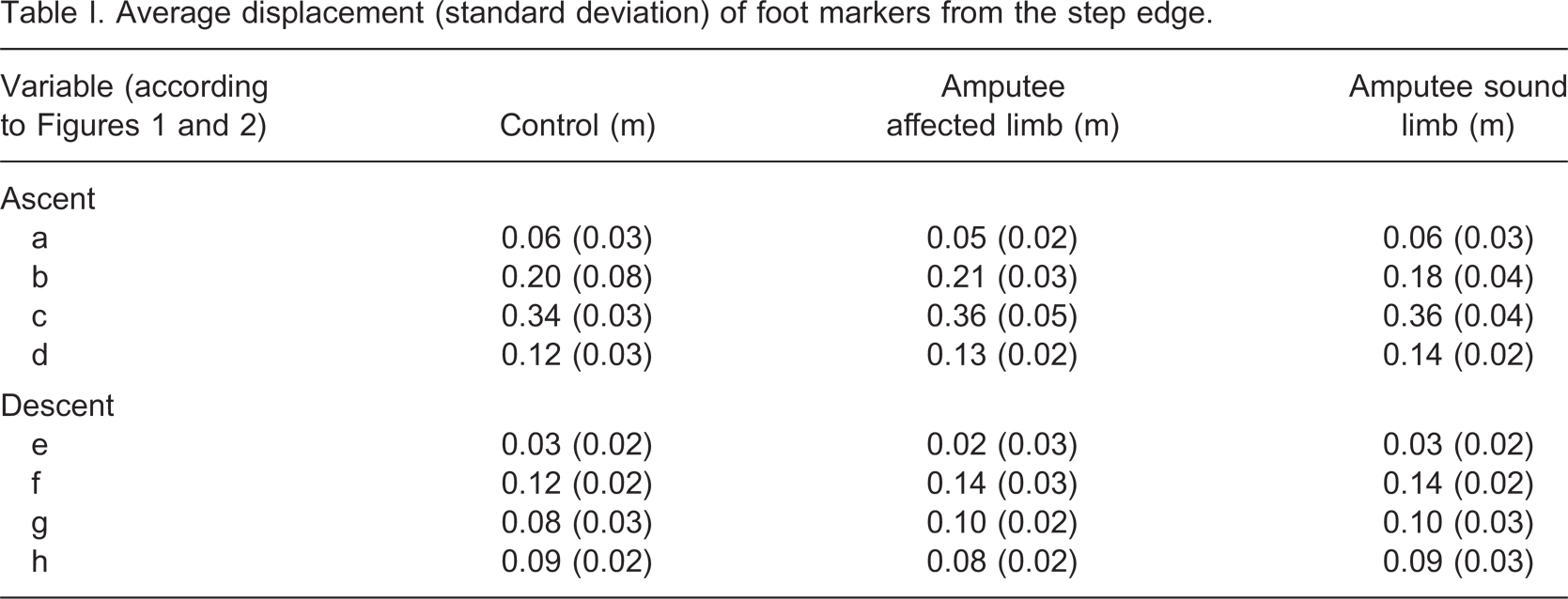
No significant deviations from normal distribution were found. A paired t-test revealed no significant difference in foot placement and clearance between the control group's left and right legs (p > 0.05). As a result, only the right leg of the control group was included in comparisons of foot placement and clearance between amputees and controls. Average results for foot position and step clearance data are presented in Table I. A paired samples t-test revealed no significant differences regarding foot position or foot clearance between the amputees' sound and affected sides (p > 0.05). Independent t-tests were used to compare the amputees' affected side to the control group and the amputees' sound side to the control group. No significant differences were observed for any of the comparisons made (p > 0.05).
Average displacement (standard deviation) of foot markers from the step edge.
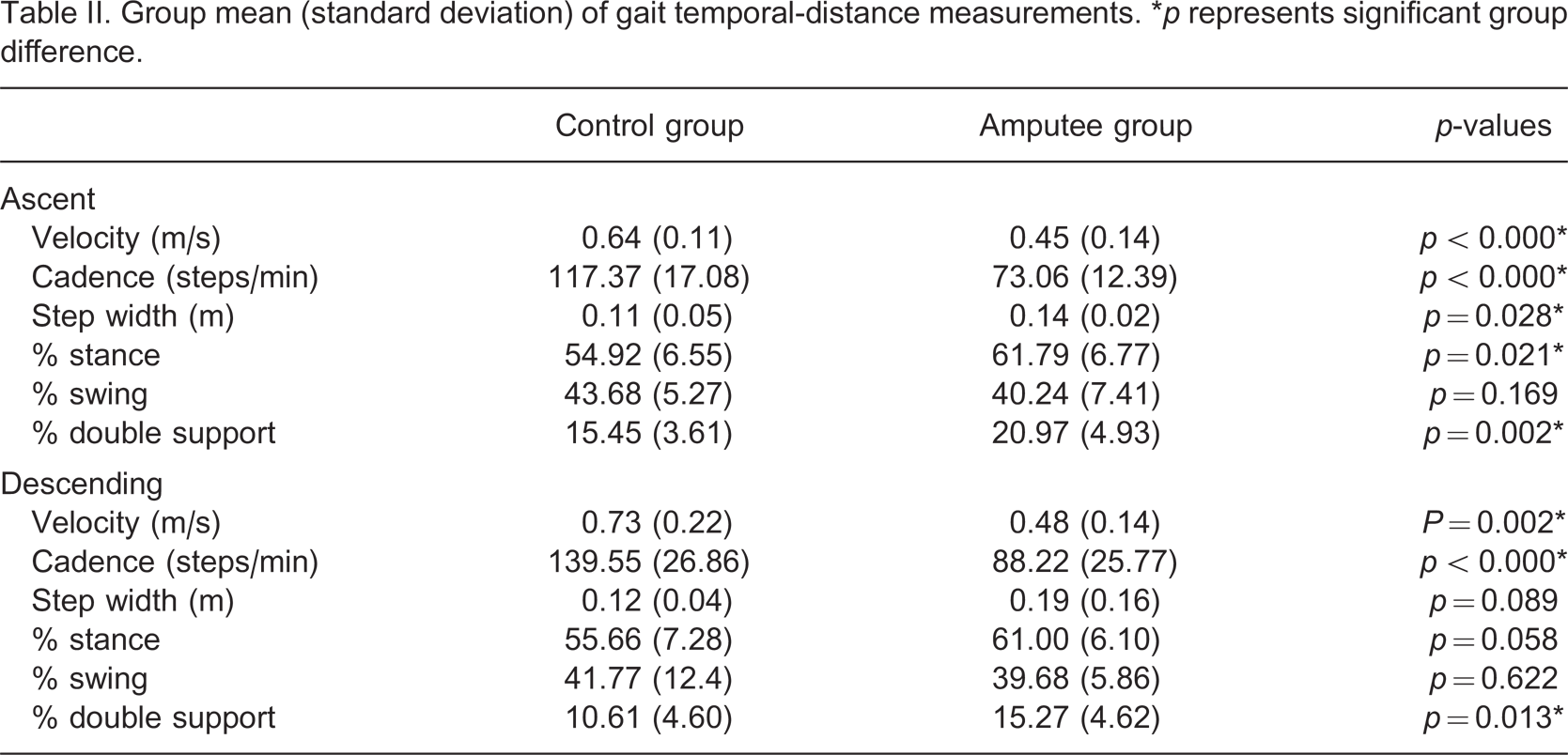
Temporospatial data is presented in Table II. Results demonstrate that the amputee population chose to ambulate at a significantly slower velocity than the control group in both stair ascent and descent (p < 0.05), had a slower cadence in both stair ascent and descent (p < 0.05), increased step width during stair ascent (0 < 0.05), spent a significantly greater proportion of the gait cycle in stance phase during stair ascent and spent a greater portion of time in double support for both stair ascent and descent (p < 0.05). Both amputees and controls were shown to spend a greater proportion of the gait cycle in double support during stair ascent (amputee = 20.9%; able bodied = 15.4%) as opposed to stair descent (amputee = 15.3%; control = 10.6%) (p < 0.01).
Group mean (standard deviation) of gait temporal-distance measurements. ∗p represents significant group difference.
Discussion
The primary purpose of this research was to compare foot placement and swinging limb clearance of amputees and able-bodied subjects while walking up and down a staircase. We hypothesized that reduced ankle motion and reduced proprioception in the amputee's affected limb would result in significant differences in foot placement and foot clearance as compared to the control group and as compared to their own sound side. Our results however, did not support this hypothesis and demonstrated no difference in the foot placement and clearance strategies used by the amputee and control groups.
Previous studies involving elderly populations have demonstrated that older adults utilize a foot placement strategy that involves less vertical and horizontal clearance than young adults and that they place their foot closer to the edge of the step. 2 While these results could account for the increased risk of falls in elderly populations, results of the present study do not support this as a cause of increased risk of falling in an amputee population. As foot placement and foot clearance during stair ambulation is so similar between able-bodied and amputee subjects it is unlikely that the incidence of falls from stairs in an amputee population could be significantly reduced by altering gait training protocols to emphasize foot placement strategies beyond that which is already done.
If foot placement and clearance are unlikely to be a cause of the increased risk of falls from stairs in an amputee population we must look to other variables that may increase this risk. Several temporospatial variables have been linked to an increased risk of falls during ambulation. These include a reduced gait velocity, 11 a wider step width 12 and prolonged double support time. 12,13 Temporospatial data from the present study has demonstrated that, during stair ambulation, amputees have a reduced walking velocity, step width and a prolonged period of double support when compared to an able-bodied population. While changes in temporospatial variables are a useful predictor of falls, 12 it is likely that they are secondary to underlying balance issues. This study did not aim to compare the balance of able-bodied and amputee subjects during stair ambulation; however, in light of the results we suggest that additional research into balance control during stair locomotion is warranted. This could be investigated, for example, by studying frontal and sagittal plane motion of the centre of mass during both stair ascent and descent. 14
One limitation of the present study is the characteristics of the amputee population involved. Amputees participating in this study were all established prosthetic users and relatively young compared to the transtibial amputee population in Scandinavia. 15 It is subsequently not possible to generalize these results to new prosthetic users and elderly amputee subjects who would be considered to be at an even greater risk of falls. The study is also limited by the fact that the control group was not age-matched to the amputee subjects under investigation. However, as the control group was younger than the amputee group one would have expected any group differences in foot placement and clearance to be even larger. As no differences were observed between the two groups, the age difference between them is less likely to have affected the results. The limited number of subjects and trials is a further limitation of the present study. Future investigations should aim to increase the power of the study with greater numbers of subjects and additional trials. The authors further recommend studying foot placement and clearance on all steps to determine if the variables under considerations are dependent upon the step that is being targeted.
Results from the present study may have been influenced by requesting subject to alternate the foot with which they contacted the first step. It is possible that this may have affected the kinematics during stair ambulation and it is recommended that future studies alter the subjects' start position rather than instructing them which foot they should target the first step with.
Conclusion
Results from the present study provide no evidence to suggest that foot placement strategies and foot clearance are contributing to falls on stairs by amputee subjects. Results indicate that established transtibial amputees utilize foot placement strategies that are similar to those of able-bodied subjects and provide no indication that tripping or poor foot placement would lead to an increased risk of falls in this population. The authors recommend continued research into balance and stability of amputees during stair ambulation to further investigate the issue of safety on stairs.
Footnotes
Acknowledgements
The authors wish to acknowledge the assistance of Bronte George and Patrick Muller who assisted in collection of control group data in this project.