
Abstract
The aim of this pilot study was to investigate the feasibility of applying the combination of Dynamic splinting (DS) and Neuromuscular electrical stimulation (NMES) in order to improve wrist and elbow function, and range of motion, in children with upper limb contractures due to Cerebral palsy (CP). Six children aged seven to 16, with contractures at the wrist or elbow, were recruited. Following a 12-week baseline period all participants underwent a 12-week treatment period where DS was used for one hour per day and combined with NMES for the second half of the 1-h treatment. A 12-week follow-up period then ensued. Upper limb function was assessed with the Melbourne assessment, physical disability with the Paediatric Evaluation of Disability Index and the Activity Scale for Kids, and quality of life with the Pediatric Quality of Life Scale. Passive and active range of motion at the wrist and elbow were measured using manual and electrical goniometers. The technique of using combined NMES and DS was demonstrated to be feasible and compliance with the intervention was good. There was an increase in passive elbow extension in two participants treated for elbow contractures, although no accompanying change in upper limb function was demonstrated. Wrist range of movement improved in one participant treated for wrist contracture.
Introduction
Cerebral palsy (CP) affects one child in 400 live births. 1 Around half the children with CP have upper limb involvement (30% have hemiplegia and 20% have quadriplegia) and a resulting upper limb posture with flexion at the elbow, wrist and fingers, usually accompanied with ulnar deviation at the wrist and forearm pronation. A review of the management of spastic hemiplegia reported that in a group of 90 patients half had elbow flexion contractures and that tightness at the wrist and fingers was common. 2
Contractures are caused by shortness of contractile tissue, intramuscular connective tissue, and connective tissue parallel to a joint. Contractures can develop such that the limb is functionally restricted. This means that in hemiplegia, for example, the affected limb may only be able to assist the non-plegic side at best. This can cause problems with mobility, function, hygiene, cosmetic appearance, and sometimes pain, affecting the quality of life of both patients and carers.
Current treatments for contractures include surgical correction, anti-spasticity medication, physiotherapy, serial casting and passive splinting. 3 All these approaches have limitations: Some have time limited effects; some tend to show regression when predisposing factors persist. There is a need for long-term management of such contractures, and so dynamic orthoses have been designed that apply a mechanically generated torque to a joint to stretch the contracted tissue. These orthoses apply a controlled stretch through the whole range of joint motion. They can be removed to aid hygiene and they promote patient independence and autonomy as the orthoses can be used at home. 4 This Dynamic Splinting (DS) can be used with other complementary modalities to apply stretch to gain range of motion without long-term immobilisation and muscle atrophy. 5
Neuromuscular electrical stimulation (NMES) of the upper limb has been used for patients with a variety of neurological conditions, 6–9 although few studies have been conducted on its use on the upper limb of children with CP. Carmick published two case reports, both of them reporting qualitative functional improvements following varying amounts of NMES of wrist extensors. 10,11 Two children with CP, aged 11 and 12, who followed a programme of EMG-initiated NMES of wrist extensor muscles, three sessions a week for eight weeks, demonstrated functional improvements but no changes in range of movement. 12 In another study, cyclic NMES was used on the wrist extensor muscles of a group of eight children (five boys, three girls) with hemiplegic CP (mean age 10 years). 13 The intervention showed an improvement in active wrist extension range of motion and function in children with CP, but not for those children with contractures. Contractures may limit the effectiveness of NMES, whilst daytime splinting regimes tend to reduce functional use of the hand. 2 A recent study investigating the application of NMES to wrist flexors and extensors in eight children, aged five to 15 years, with CP 14 demonstrated improvements in active wrist extension range of movement and isometric wrist extension torque.
In a study by Scheker et al., 19 participants with CP, aged four to 21 years, were treated daily with combined DS and NMES for between three and 43 months. All participants moved up by one to three levels in the Zancolli classification of hand posture and showed improvement in upper limb function. 15 Ozer et al. also applied NMES and DS to treat spasticity at the wrist and elbow of eight children with CP, one hour a day for six months. 16 Another group of eight children in this study received only NMES while a third group of eight children received only DS. Significant improvements in upper limb function measured with the Melbourne Assessment, grip strength and the Zancolli classification were demonstrated in the group that had received the combined intervention. However, although the subjects studied by Schecker and Ozer did not have full active movement, no mention is made of them having fixed joint contractures that prevented full passive motion. The DS in Ozer's study comprised a combined wrist and elbow unit and was manufactured by Ultraflex. A LODE 400 ElectroMed Systems NMES device was used in conjunction with this. The aim of this study was to investigate the feasibility of applying a custom-made DS, in conjunction with NMES, to the wrist or elbow joint (or both) of six children with CP who had fixed joint contractures that prevented full passive motion.
Methods
Participants
Six children aged between seven and 16 years with the following inclusion criteria were recruited: A diagnosis of spastic CP, restricted range of movement at either the wrist, elbow, or both due to fixed contracture, and visual, cognitive and behavioural ability to allow full compliance with the assessment procedures and treatment regime. Children with dystonia, uncontrolled epilepsy and those who had undergone any upper limb surgery or anti-spasticity treatment in the previous six months were excluded. Ethical approval for the study was obtained from the local research ethics committee (ref: 05/Q2008/57). Each child was assessed upon recruitment, in order to determine which joint would be treated with the dynamic splint.
Orthotic devices
Electrical stimulation was applied through surface electrodes (PALS, Axlegaard) using a Microstim MS2 battery powered stimulator (Odstock Medical Ltd, Salisbury, UK). An asymmetric biphasic waveform at a frequency of 40 Hz was used (pulse width 330 μs, ramp up and down 2 s, on:off ratio 10:10 s). The stimulation intensity was set to a level that elicited a contraction sufficient to cause movement at the joint, whilst remaining tolerable for the participants. Figure 1 shows electrode positions for the elbow extensors and the wrist extensors.
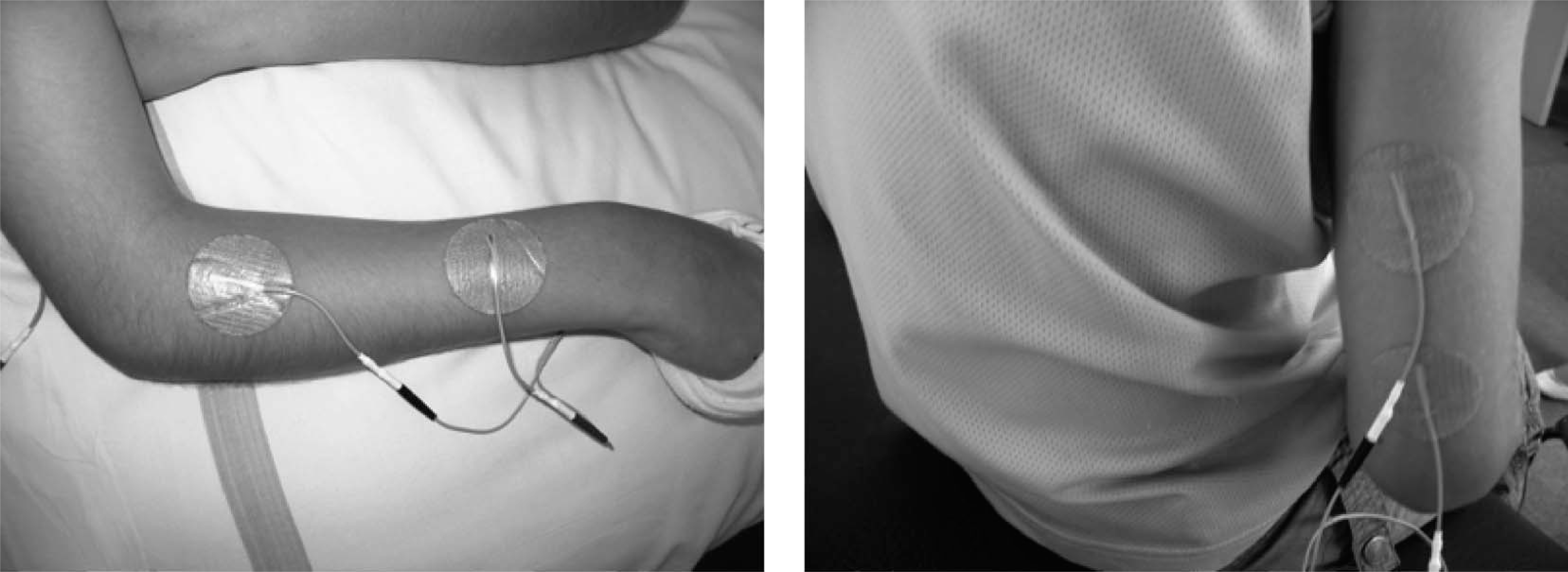
Electrode positions for the wrist extensors (left) and elbow extensors (right). The active electrodes were those placed proximally with the indifferent electrodes placed distally.
The DS comprised custom moulded polypropylene sections connected by a hinge. The orthoses were powered by concentric adjustable torsion units (Ultraflex Systems, Pottstown, PA, USA). These units employ a clockwork spring design that can produce an almost constant torque across the functional range of the splint. Figure 2 shows a participant wearing a DS about the elbow joint together with the stimulator. In the case of those participants with only elbow contractures the DS applied an extension torque to the elbow joint and the NMES was applied to the triceps. In the participants with wrist contractures the DS applied an extension torque to the wrist and NMES was applied to the wrist extensors. The appropriate torque setting for each participant was determined by a local orthotist. This was set at a level that was tolerable to the participant but that could be overcome with effort.

Photograph of child wearing dynamic splint and stimulator.
Design
A longitudinal single participant study design was used. 17 Figure 3 shows the timeline of the study and the outcome measures used in each assessment. At the first assessment, the participants were cast for the DS. The DS was supplied at the second assessment, six weeks later, but was not used therapeutically during the baseline period. The participants were encouraged to wear the DS for up to an hour per day with the torque set to zero during this time. This allowed them to become accustomed to the DS and ensure that it was comfortable. A 12-week treatment period followed when the participants wore the DS for one hour per day, and combined this with NMES for the second half of the one hour treatment. The participants attended the clinic twice during the treatment period (at 4 and 8 weeks) to check the torque settings and general fit of the DS and to ensure that the stimulator was producing a satisfactory muscle contraction that resulted in appropriate movement of the joint. Torque settings were reviewed at each assessment throughout the intervention phase of the trial and altered if necessary. During the 12-week follow-up period the participants continued with their conventional therapy regimen. Descriptive statistics for single-case and small-n designs were used to analyze the data. 17 Data were compared within each participant to determine changes over time.
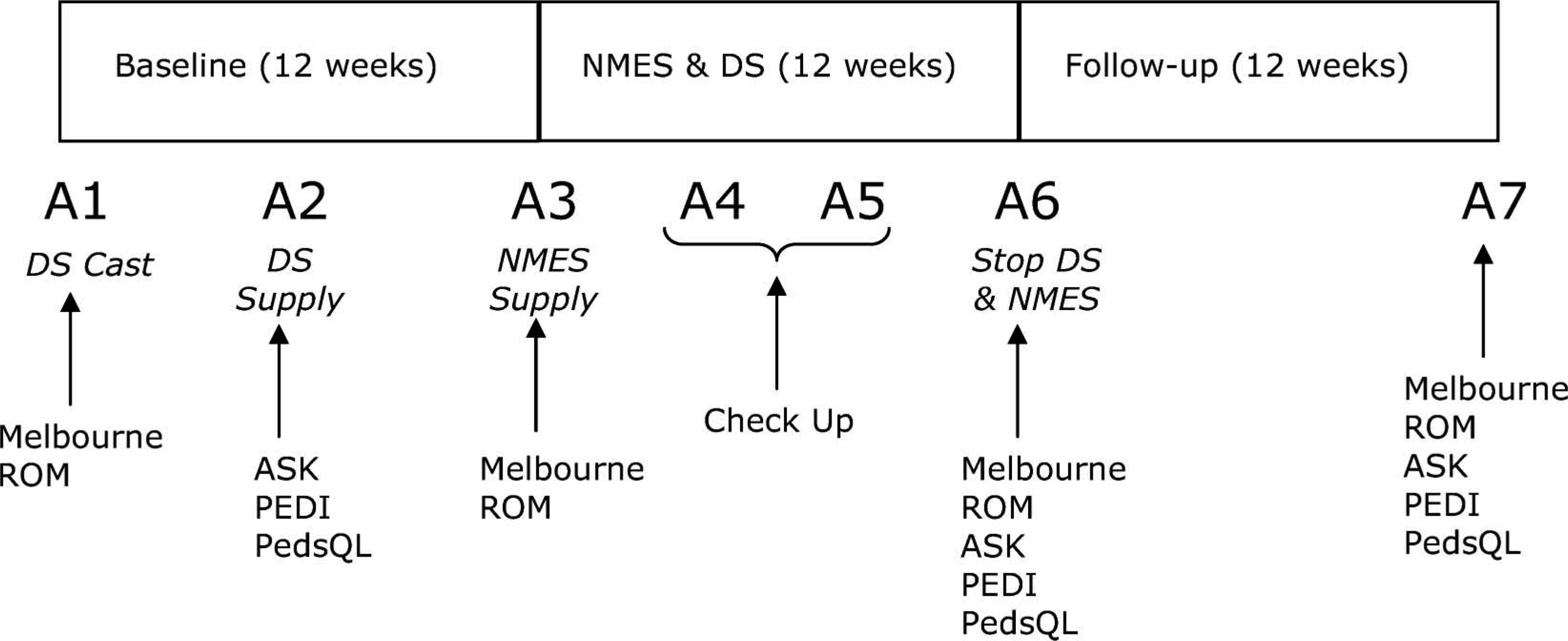
Timeline of study and outcome measures used in each assessment.
Outcome measures
Upper limb function was assessed using the Melbourne Assessment of Unilateral Upper Limb Function. 18 Passive range of movement at the wrist and elbow was measured using a protractor goniometer. Active range of motion was measured using twin axis electrogoniometers (Biometrics Ltd, Gwent, UK). To measure active range at the elbow joint the participants were instructed to flex and extend their elbow as far as possible, starting from a position of maximum flexion. This was then repeated for the wrist joint. One passive and one active measurement were taken at each assessment. The following criteria were applied to determine if there had been a change in range of movement: The value at the end of the treatment phase must be 5° greater than the largest of the two baseline values, or 5° smaller than the smallest baseline value. 19
The Pediatric Evaluation of Disability Index (PEDI), 20 and the Activity Scale for Kids (ASK) 21 were used to assess physical disability. Quality of life was assessed with the Pediatric Quality of Life Scale (PEDSQL). 22 Participants were asked to keep a diary of their use of the DS and NMES to monitor compliance.
Results
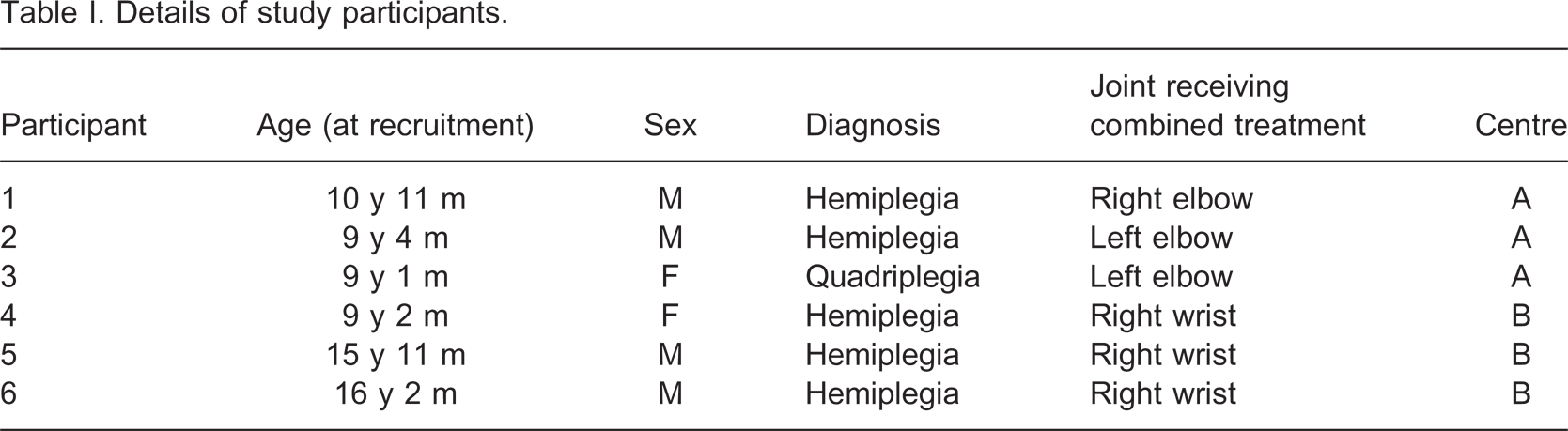
Six children aged between seven and 16 years with a diagnosis of spastic cerebral palsy took part in the study. Three children were recruited from regular paediatric clinics at both of the two participating centres. Informed consent was obtained from all the participants and their parents or guardians prior to entry into the study. Details of the participants are given in Table I. In three participants the predominant contracture was at the elbow, while in the remaining three participants the predominant contracture was at the wrist. In each case this was the joint treated with the combination of the DS and NMES. The technique of applying DS in combination with NMES was seen to be feasible in this population.
Details of study participants.
The torque setting on the DS for participant 1 remained at 2.5 Nm throughout the treatment period. Participant 2 had his torque setting increased from 1.5–3 Nm at week 4 of the treatment period. The torque setting for participant 3 was increased at week 4 (from 1.0–1.2 Nm), and increased again, to 1.5 Nm at week 8 of the treatment period. The initial torque setting for participant 4 was 0.3 Nm, which was increased to 0.7 Nm at week 8 of the intervention period. Participants 5 and 6 both had their torque settings increased from 0.7–1.2 Nm at week 8 of the intervention period.
Four participants returned completed diaries indicating good compliance in three cases; however, compliance for participant 3 was only just above 50%. Two participants did not return their completed diaries, but gave verbal confirmation of compliance with the protocol. The opinion of participants and parents on the intervention was gauged by informal discussions. The feedback was generally positive, and three of the children voluntarily continued with the treatment after the end of the study.
Melbourne Assessment scores are displayed in Figure 4. The raw scores were converted to percentages. A higher score indicates better limb function, with 100% indicating unimpaired function. There was no change in function measured by the Melbourne Assessment in those participants whose elbow contractures were treated. There were small increases in the Melbourne Assessment score for participants 4 and 6 following treatment, though these were not large enough to be considered clinically significant. 18 The Melbourne Assessment score for participant 4 increased by 6.5% above the larger of the two baseline values, and the score for participant 6 increased by 4.9% above baseline. In the case of participant 6 this was maintained after the follow up period. There was no change in limb function for participant 5.
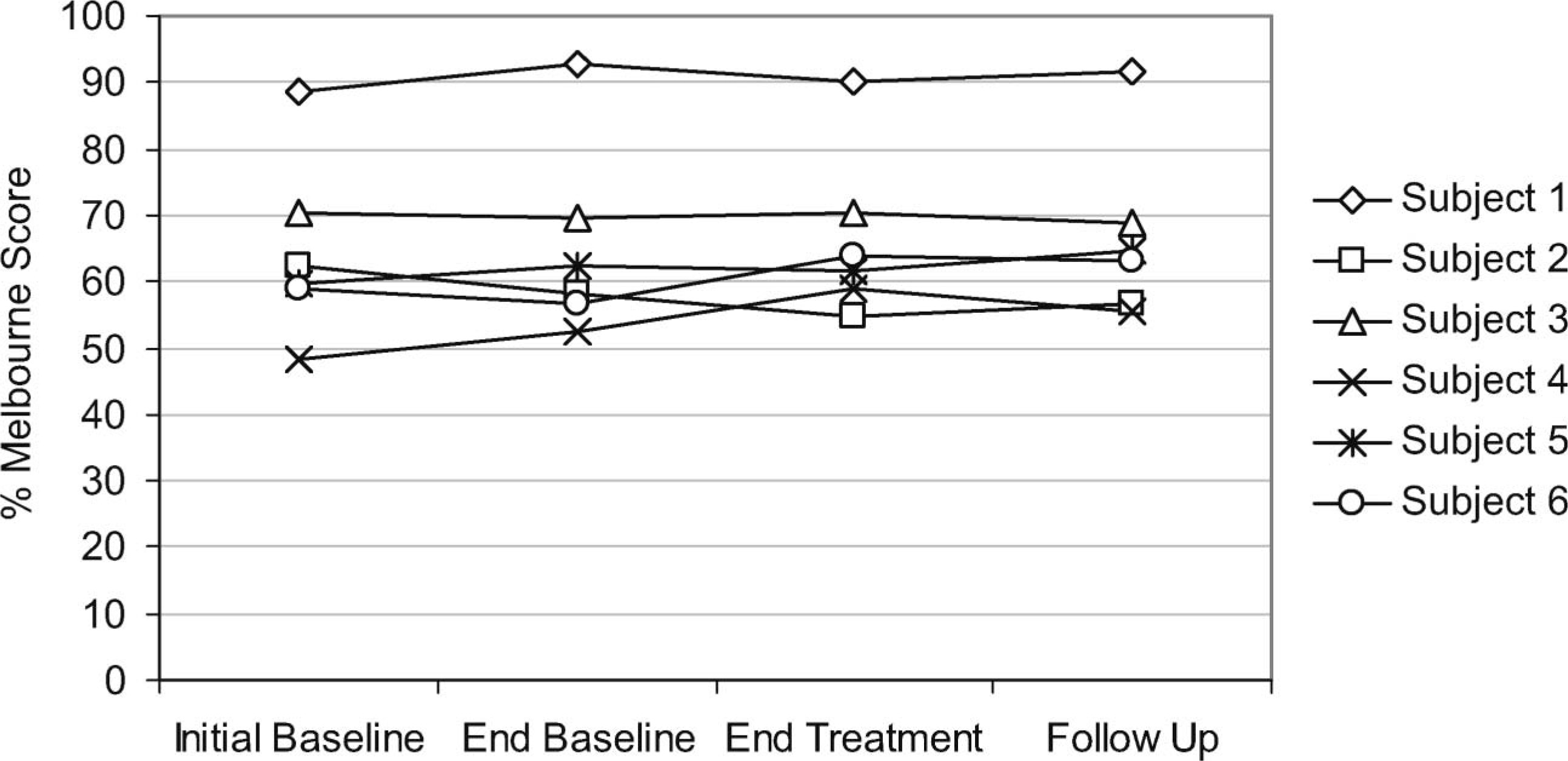
Melbourne Assessment scores for each participant throughout the study.
Figure 5 shows the ASK scores recorded at each assessment, also given as percentages. There was no change in the ASK score for participants 1 and 2. The scores for participants 3 and 4 increased after the treatment, but this was not maintained after the follow-up period. There was no change ASK score for participant 5, but there was an increase for participant 6 after the follow up period.
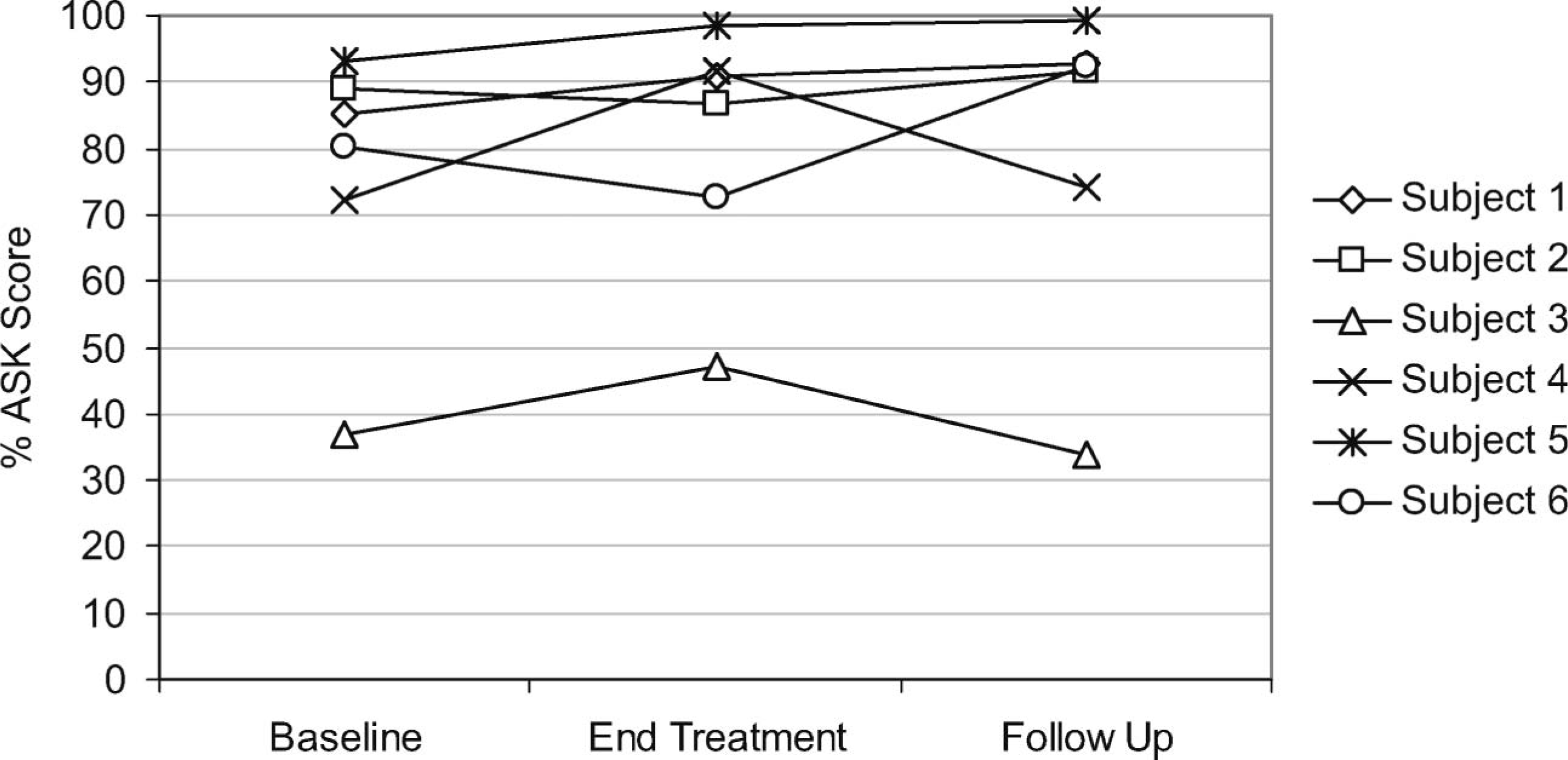
ASK scores for each participant throughout the study.
Passive and active ranges of movement at the treated joint are shown in Figures 6 (elbow) and 7 (wrist). Passive elbow extension increased at the end of the treatment period for participants 1 and 3; however, active elbow range of movement did not change. Passive wrist extension increased for participant 4 but active range of movement did not change. Both active and passive range of movement decreased following treatment in the case of participant 5, and there was a subsequent increase in range after follow-up. There was no change in range of movement for participant 6 following treatment, but active range of movement increased after the follow-up period.
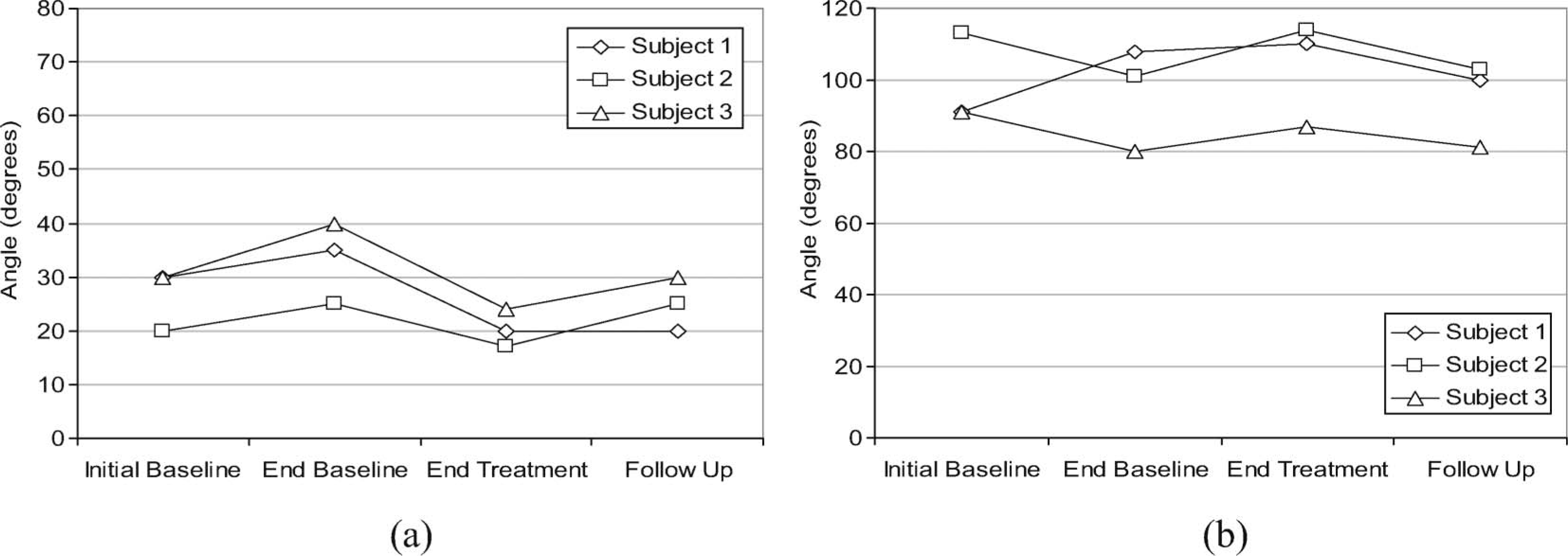
Passive extension (a) and active range of movement (b) at the elbow for participants treated for elbow contractures. For passive extension, 0° represents full extension and an increase in angle represents a decrease in passive extension.
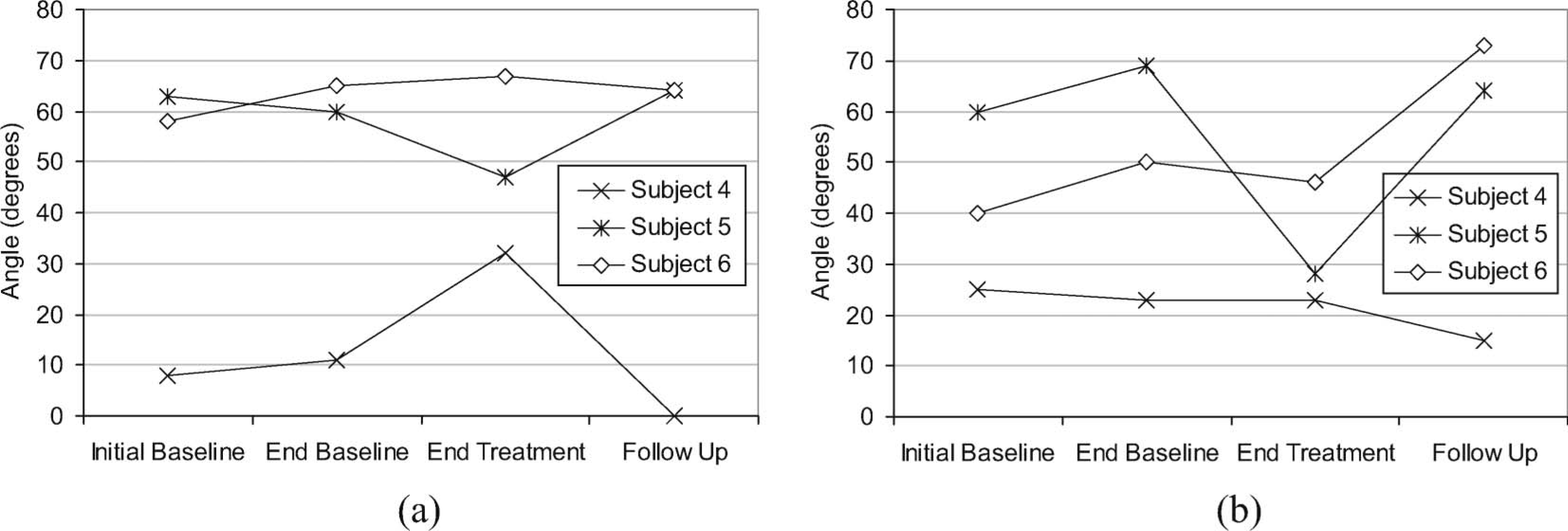
Passive extension (a) and active (b) range of movement at the wrist for participants treated for wrist contractures.
There was no change in PEDI scores for participants 1, 4, 5 and 6. The score for participant 2 increased following treatment, although there was also a subsequent increase after the follow-up period. For participant 3, the part of the index that related to care giver assistance increased following treatment implying that there had been some improvement in the participant's level of independence. There was a decrease in this score after the follow-up period. The PedsQL relating to daily activities score increased following treatment in participants 1 and 4; however, there was a reduction in the score for participants 2, 3 and 6. There was no change in the PedsQL score for participant 5.
Discussion
The technique of applying a customized DS system and NMES to the wrist or elbow joint of children with CP who had fixed joint contractures that prevented full passive range of motion was demonstrated to be feasible. Previous studies investigating the combined application of DS and NMES to the upper limb of children with CP have not reported on whether fixed joint contractures that prevented full passive motion were present. 15,16 Compliance with the intervention in this study was good. This combined intervention has the advantage that it can be self-administered by the patient with minimal assistance from carers, and thus has the potential to significantly increase the amount of therapy time devoted to upper limb impairments.
The intervention appeared to demonstrate a greater impact on upper limb function in those participants who were treated for wrist contractures, however, the changes in the Melbourne assessment score were small and a longer treatment period may be required for clinically significant changes to occur. The small increases in Melbourne Assessment scores for participants 4 and 6 were mainly related to the items in the assessment that involved the release of objects into a container. These were scored on range and quality of movement and accuracy of release.
Passive elbow extension increased at the end of the intervention period, although active elbow range of movement did not change, in those participants who were treated for elbow contractures. Improvements in upper limb function have previously been reported following NMES 10–13 or a combined DS and NMES intervention 15,16 applied to the upper limb of children with CP. However, no studies were found in the literature where improvements in passive range of movement had previously been reported following NMES or a combined NMES and DS intervention applied to the upper limb of children with CP.
The increase in passive extension of the elbow did not translate into an improvement in function. This may indicate that muscle weakness or lack of selective control remained a problem and the participants were unable to exploit the increased range of movement. The activities that comprise the Melbourne assessment may be more representative of wrist and finger function. Few of these activities require full, or near to full, elbow extension for adequate accomplishment. Other items score range of wrist extension during activity into categories. It is therefore possible that a small improvement in elbow or wrist extension would not influence the score significantly.
Participant 5 showed a decrease in both passive and active range of movement following treatment, although there was no change in the Melbourne assessment. It could be expected that such a large decrease in active range of movement in particular would have an effect on the Melbourne assessment. There was also a large discrepancy between the passive and active range of motion following treatment, which was not present during the other assessments. Whilst there may have been a genuine negative treatment effect, the inconsistency indicates that compliance with the measurement protocol for active range of movement may have been a problem for this participant.
We noted that difficulty with supination was one of the main reasons why participants failed some of the tasks in the Melbourne assessment. The intervention did not address this and thus could not be expected to have a positive effect on performance of these tasks. A DS that assists supination can however be fitted. Likewise it would be possible to achieve forearm supination through, for example, stimulation of biceps brachii, and so a combined NMES and DS intervention may be realised in future work. The Assisting Hand Assessment method, 23 used to assess the function of the affected limb in children with a unilateral upper limb problem, is an alternative measure of changes in function to the Melbourne assessment and could also be considered in planning future work.
The variability in response to the questionnaires for the PEDI and PedsQL assessments suggests that these indices may not be well suited to small studies and intra-subject designs. Alternative assessment tools may be more appropriate for future studies, such as an adaptation of the Canadian Occupational Performance Measure. 24
Determining which patients gain the most benefit will ensure that the intervention can be targeted more effectively. A dose response study would enable determination of the amount of treatment that is required for a clinically significant effect. This would lead to optimized treatment parameters that may make the intervention more user-friendly in terms of time commitment and also increase compliance.
Conclusion
The technique of using combined NMES and DS has been demonstrated to be feasible with the six children with CP in this study who had upper limb fixed joint contractures limiting passive range of movement. It appeared the most beneficial to upper limb function when targeted at the wrist joint and this may be an obvious area for future research. Improvements in passive range of movement were also demonstrated at the elbow joint following the application of this technique. It may be appropriate for future work to consider a combined DS and NMES intervention that assists supination as improved supination would support improved upper limb function. In addition, it may be expedient to conduct a dose response study in order to optimize treatment parameters.
Footnotes
Acknowledgements