
Abstract
The numbers of lower limb amputees participating in recreational activity date back more than 25 years. Previous studies have shown that 60% of lower limb amputees participated in recreational activities, including sports. To date, research in The Netherlands into sports participation of this specific amputee population is insufficient. The purpose of the reported survey was to investigate the sports participation habits of lower limb amputees in the Province of Drenthe, The Netherlands, using a self-constructed questionnaire. A total of 105 lower limb amputees responded (36%), a large proportion of whom were traumatic amputees (31%). Of the respondents, 34 (32%) participated in some form of sport. Results indicated that participation in sport before the amputation was a predetermining factor for amputees to participate in sports whilst the level of amputation, age and etiology were not predetermining factors of participation in sports after a lower limb amputation.
Introduction
A total of 56% of adults with disabilities in the United States do not engage in any leisure-time physical activity compared to 36% among adults without disability. 1 These results are consistent with the notion that, on average, people with a disability are more inactive than the general population. 2,3 There are cultural differences between the United States and The Netherlands in sports participation. 4 It has been shown that while the average American person is inundated by sports and very much involved in sports participation, the Dutch population is more reserved in their participation in sports. 5 However, in The Netherlands, participation in sports activities continues to gain popularity. 6 Recent surveys revealed that over 60% of the total Dutch population (18–79 years old), including disabled individuals, participated in sports 12 times or more per year. 6,7 From the disabled population substantially fewer people participated in a sport, with the percentages ranging from 39–1.4%. 6,8 This wide range of percentages demonstrates that it is difficult to attach an exact figure to the number of people with a disability participating in sports.
The apparent difficulty in estimating the amount of people with a disability participating in sports is likely due to difficulties in defining the terms ‘disability’ and ‘sports participation’. According to the World Health Organization (WHO), disability serves as an umbrella term for impairments (problems in body function or structure such as a significant deviation or loss, such as amputation), activity limitations (difficulties an individual may have in executing activities) or participation restrictions (problems an individual may experience in involvement in life situation). 9 The WHO defines physical activity as any bodily movement produced by skeletal muscles that requires energy expenditure. 10 As such, it includes sports but also physical activities such as playing, cleaning the house, dancing or climbing stairs. 2 In accordance with the Dutch norm for healthy exercise, 11 for the current study sports is defined as an activity involving physical exertion with or without a game or competition elements, with a minimal duration of half an hour, and where skills and physical endurance are either required or to be improved.
Physical inactivity is one of the most important health risk factors. Inactivity contributes to early death by heart and coronary diseases and other chronic conditions. 1–3,6,8 Physical activity on the other hand, including sports, provides positive effects on the physical, physiological and social wellbeing of all people with or without a disability. 6,12–15
The most recent information about sports participation of lower limb amputees dates back more than 25 years. In the United States two studies took place concerning recreational activities (including sports) of people with a lower limb amputation. 16,17 The results of both studies showed that 60% of the amputees (n = 134 16 and n = 10016) participated in a recreational activity which included participation in sports as defined in the present study. 16,17 Recent information about sport participation of lower limb amputees in The Netherlands does not exist.
The incidence of lower limb amputations in The Netherlands is 20 per 100,000, resulting in 3,200 amputations annually. 18 In view of these considerable numbers and because of the beneficial health effects of sport participation, the purpose of the present survey was to investigate the sports participation habits of lower limb amputees in the Province of Drenthe, The Netherlands. The key outcomes of interest were the age of the participant (age), how long since amputation (post-amputation time), where the limb was amputated (level of amputation), the etiology underlying the amputation (etiology), and the history of sports participation of the lower limb amputees.
Methods
Amputees living in the Province of Drenthe, The Netherlands (population 486,903 19 ) were approached through the OIM (a group of orthopedic workshops). The database of these orthopedic workshops contains the details of all the amputees living in the Province of Drenthe who have been prescribed with a prosthesis. Inclusion criteria for participation in the study were age (from 18–80 years) and level of amputation (proximal to a Syme amputation, such as transtibial, knee disarticulation, transfemoral, hip disarticulation and hemipelvectomy amputations). Amputees who were admitted to nursing homes, and amputees who were not prescribed with a prosthesis were excluded from this study.
Instrument
The instrument used in this study to investigate the sport participation habits of lower limb amputees was a questionnaire (24 questions, see Appendix). This self-constructed questionnaire was partially based on previous studies. 21–23
Procedures
Questionnaires were mailed to the 290 lower limb amputees that met the criteria as set out above. An accompanying letter explained the purpose of the questionnaire and assured the participants that responses would remain confidential and treated anonymously. Participation was voluntary. The amputees were asked to complete and return the questionnaire within three weeks.
Design and variables
The following questions were addressed in this study: What is the relationship between the level of amputation and sports participation?; What is the relationship between and sports participation?; What is the relationship between the etiology resulting in the amputation and sports participation?; How many of the respondents participated in sports before their amputation?; How many of the respondents participate in sports at the time of filling in the questionnaire (present participation)?; Is there a difference between the post-amputation time of presently non-participating and presently participating amputees?; How many of the respondents have complaints about their prosthesis?, and, Do the complaints hinder their participation in sports?; How many respondents have co-morbidity?, and, Does co-morbidity hinder sports participation?; How many of the respondents who participated in sports before their amputation are presently participating in sports?; What are the reasons to participate in sports?; What are the reasons for not participating in sports?
In order to facilitate the data analysis the variable, level of amputation, was divided into three categories: Above the knee; knee-disarticulation; and below the knee. The above the knee category was subdivided into the levels hemipelvectomy, hip disarticulation and transfemoral, and the below the knee category into the levels transtibial and ankle disarticulation.
Data analysis
Data were analyzed using the Statistical Package for Social Sciences 14 (SPSS). A Mann-Whitney test was used to test the differences between the variables age and post-amputation time between presently participating and presently non-participating amputees. Crosstabs and Pearson Chi-square tests were used to test the expected relationships between the variables of age with present participation, level of amputation with present participation, etiology with present participation and the history of participation in sports with present participation. Significance in this study was preset at the 0.05 level of probability.
Ethical approval
The study was approved by the Medical Ethical Committee of the University Medical Center Groningen.
Results
Participants
The questionnaire was sent to 290 lower limb amputees, 107 of whom responded (37%). Two of the respondents were left out of the data analysis because they appeared to have a partial foot amputation and hence did not meet the inclusion criteria. Of the 105 remaining respondents, 71 were male (66%) and 31 were female (29%) (three missing values). As shown in Table I, 34 (32%) were participating in some form of sport. The age range of the respondents was 23–79 years. The mean age of the sports-participating respondents was 55.5 (SD = 11.5) years while the mean age of the non-sports-participating respondents was 60.2 (SD = 13.1) years (U = 842.000; p = 0.034; r = −0.21). The mean post-amputation time of the sports-participating respondents was 198.9 (SD = 207.8) months and of the non-sports-participating respondents 150.4 (SD = 213.9) months. This difference between the sports-participating and the non-sports-participating respondents in mean post-amputation time was not significant (U = 845.000; p = 0.059; r = −0.19). Four respondents (4%) were amputated bilaterally, 59 respondents (55%) were amputated on the left side and 42 respondents (39%) were amputated on the right side (two missing values).
Frequencies of age, level of amputation, etiology and history of sports participation, for presently participating amputees in sports.
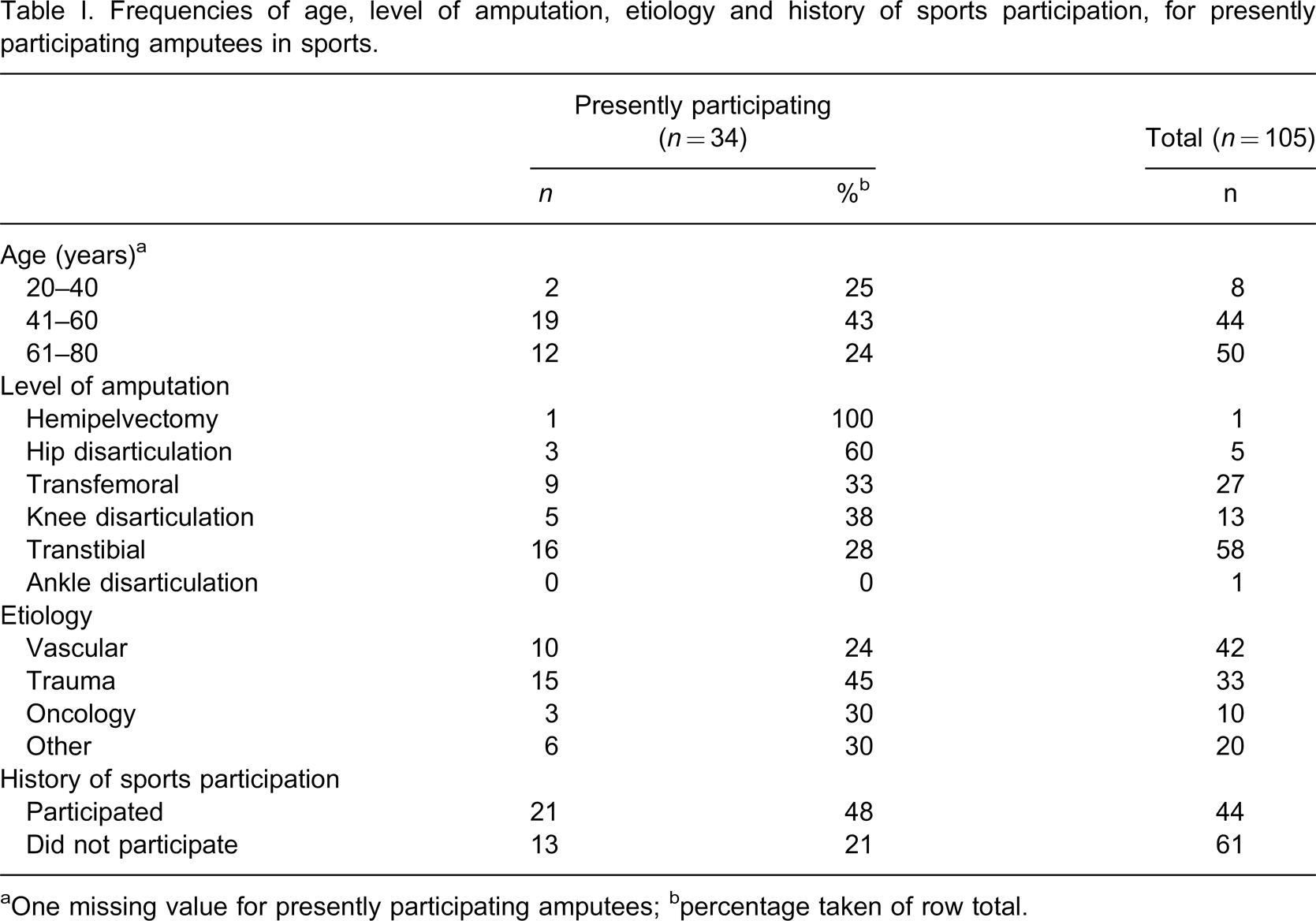
aOne missing value for presently participating amputees; bpercentage taken of row total.
Present sports-participation
Further analysis of the data showed that age, level of amputation, and etiology could not predict sports participation after a lower limb amputation. None of the effects of age (χ2 = 4.149, df = 2, p = 0.126), level of amputation (χ2 = 1.707, df = 2, p = 0.426) and etiology (χ2 = 4.063, df = 3, p = 0.255) on present participation reached significance. On the other hand, the history of sports participation (participation in sports before the amputation) served as significant predictors (χ2 = 8.146, df = 1, p = 0.004). These results imply that when a lower limb amputee participated in sports before the amputation there was a higher likelihood that the participation in sports after the amputation compared to when the lower limb amputee did not participate in sports before the amputation.
Sports
The most common sports the respondents participated in after their amputation were swimming (n = 10), fitness (n = 9), cycling (n = 6) and walking (n = 4).
Reasons for participation in sports (multiple answers were possible)
The mean reasons given by the respondents for participating in sports were: good for health (n = 27), good feeling (n = 20), need to participate (n = 13), social contacts (n = 13), and doctor's advice (n = 8).
Reasons for non-participation in sports (multiple answers were possible)
The reasons given by the respondents for not participating in sports were: absence of needs (n = 29), fear (n = 7), no facilities (n = 6), disease (n = 5), problems with prosthesis (n = 4), age (n = 4), and skin lesion (n = 4).
Complaints, co-morbidity and costs
Of the 105 respondents, 44 had complaints about their prosthetic device or sports organization. Eighty percent (80%) of these respondents found these complaints hindering their sports participation. Some 56% of the 57 respondents who had answered that they had co-morbidities indicated that these were a hindering factor. The costs of the prosthetic devise hindered the sports participation of 14% of all the respondents.
Discussion
The results of the current study indicate that age, level of amputation, and etiology of amputation were not related to sports participation after a lower limb amputation. On the other hand, the history of sports participation before the amputation could be reliably related to participation in sports after a lower limb amputation. These results suggest that if an amputee is participating in sports before his amputation it is more likely that the amputee will be participating in sports after his amputation.
There was a significant difference between the mean age of the present sport-participating respondents and the mean age of the present non-sport-participating respondents. As maybe expected, the respondents of the highest age-category (61–80 years) participated less than respondents of other age-categories (Table I). However, the differences between the percentages of participation of the high age-category and the youngest age-category were non-significant (24% versus 25%; 12 out of 50 respondents of high age, and 2 out of 8 youngest respondents, participated in sport). The studies of Kegel et al. 16,17 show larger differences between the mean age of the recreational active and recreational non-active participants. Kegel et al. 16 reported in the first study a mean age of 44 years for the recreational active respondents and a mean age of 65 years for the recreational non-active respondents, but this difference was not statistically tested. In the second study of Kegel et al. 17 the mean age of the recreational active respondents was also lower than the mean age of the recreational non-active respondents, respectively, 36 years and 61 years of age, but again this difference was not statistically tested.
In the present study the authors did not find a relationship between the age at the time of amputation and sports participation. The only other known reported relationship between age at the time of amputation and being presently participating in sports was reported by Kegel et al. 17 They found a mean age at time of amputation of recreationally active respondents of 25 years and a mean age at time of amputation of 50 years of respondents that were not recreationally active. This difference was not statistically tested.
The current results showed no relationship between the level of amputation and sports participation. That is, no differences could be established between the amounts of present sport-participating respondents with an above the knee amputation (hemipelvectomy, hip disarticulation and transfemoral amputation), with a below the knee amputation (transtibial amputation and ankle disarticulation) with a knee-disarticulation. It was observed that a higher percentage of the respondents with an above the knee amputation participated in sports compared to the percentage of respondents with a below the knee amputation. This is in line with the results of the second study of Kegel et al., 17 where 60% of each group of respondents with different level of amputation (below or above the knee amputation or bilateral amputations) were recreationally active. This in contrast to the first study of Kegel et al. 16 where level of amputation appeared to play a role in determining whether amputees were being recreational active. This is also contrary to the expectation that above the knee amputees will participate less in sports because they have a higher energy consumption than below the knee amputees. 23–25
No significant differences were found between the amount of present sport-participating respondents with a lower-limb amputation caused by a trauma and the amount of present sport-participating respondents with a lower-limb amputation caused by a vascular disease. Kegel et al. 17 did find that the most recreational active amputees were those who had their amputation as a result of a trauma (43 of the 57 amputees); however, they did not statistically test for the significance of this difference.
With regards to etiology, the current results show that the distribution of responses on etiology is not in agreement with the epidemiology of lower-limb amputees given in other studies. 18,26 Some 31% of the respondents had a lower-limb amputation as a result of a trauma in contrast to 3% of the general lower-limb amputee population in industrialized countries. 17,26 A possible explanation could be the presence of a large trauma centre in the University Medical Centre Groningen, which could have resulted in a larger proportion of trauma related amputees in this study. On the other hand, the percentage of respondents amputated following a vascular disease in the current study is much lower than that of the general population of lower-limb amputees, 40% against 94%. 17,23 This difference can be explained by the selection process of the 290 lower limb amputees who were asked to fill in the questionnaire. They were approached through the orthopedic workshop and included in the study on the basis of their use of a prosthesis. Some 15% of the people with a lower limb amputation due to a vascular disease cannot be successfully fitted with a prosthesis. 18 Hence, these lower limb amputees were either not selected to fill in the questionnaire or otherwise excluded from the study. The main reasons for some amputees not to be fitted with a prosthesis are poor wound healing and problems with their general condition. 18 These co-morbidities can play an important role in not wearing the prosthesis and not participating in sports.
Since the response rate was 37%, the results and conclusions of the current study should be regarded with caution. One explanation for this low response rate may be the design of the study. Response rates are found to be low in studies based on postal questionnaires. 27 Similar response rates were found in other studies with lower limb amputees. 16,17,28–31 A second explanation for the low response rate may be that lower limb amputees were invited to participate in a study concerning sports activities. It can not be ruled out that lower limb amputees who did not participate in sports at the time of invitation were less inclined to fill in the questionnaire because they did not feel the topic to be relevant to them.
It is likely that being physically active and participating in sports resulted in a higher response rate than when being less physical active and not involved in sports.
Also, the respondents may have been more positive about their sport participation because their involvement in sports or they may have given socially desirable answers.
We would have liked to compare the characteristics of responders, such as age, level of amputation, etiology, and post amputation time as well as history of sports participation, with those of non-responder participants. However, the amputees were approached by the orthopedic workshops and we only received information of the responders, and were not allowed to contact the non-responders.
The results of the current study showed firstly that the older population participated in sports more than expected, and secondly that the likelihood of participation in sports is increased when the respondents participated in sports before their amputation. Physical activity provides positive effects on the physical, physiological and social wellbeing of a person with or without a disability. 6,12–15 In the current study the number of amputees participating in sports (32%) was substantial less than the number of the general Dutch population participating in sports (60%). It is therefore concluded that members of the rehabilitation team should put much greater effort into encouragement of amputees in participation in sports and physical activity.
Footnotes
Acknowledgements
Appendix: Questionnaire
21a. Did you have any complaints or injuries over the past six months? When this was the case, what was the complaint or injury? When you did not have any complaints or injuries you can proceed to question 22a.
……………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………
21b. Does the complaint/injury hinder your participation in sports?
□ No □ Yes
22a. Do you have (beside the reason for the amputation stated at question 6) one or more of the following conditions?
□ No, go to question 23
□ Yes
When yes:
□ Rheumatism
□ Cardio-vascular disease
□ Erosion of the joints
□ Bronchitis
□ Kidney disease
□ Other, namely:…………………………………………………………………………………………………………
22b. Does this condition hinder your participation in sports?
□ No □ Yes
23. Do you think you have enough information about the available possibilities of sports participation for amputees?
□ Yes,
because………………………………………………………………………………………………………… …………………………………………………………………………………………………………………… ……………………………………………………………
□ No,
because………………………………………………………………………………………………………… …………………………………………………………………………………………………………………… ……………………………………………………………
24. How did you get into contact with the sports that you participate in?
□ Internet
□ Fellow amputees
□ Attended doctor
□ Rehabilitation centre
□ Orthopaedic workshop
□ Other,
namely:………………………………………………………………………………………………………… …………………………………………………………………………