
Abstract
The objective of the study was to assess the measurement properties of an indirect volumetric measurement using segmental circumferential measurements fitted into a formula of a truncated cone (Sitzia's method) in long-term transtibial amputees.
Twenty-eight participants with a transtibial amputation >1 year participated in the study. Two observers measured stump volume twice, two weeks apart, using both Sitzia's method and the water displacement volumetric method (criterion standard test). The mean differences and upper and lower limits of agreement between the water displacement volumetric method and Sitzia's method, between the first and second assessment, and between both assessors were calculated. Intra-class correlation coefficients (ICCs) were derived from random-effects two-way analysis of variance.
Inter-observer agreements of both methods were high and ranged from 86–96%. Intra-observer agreement ranged between 57% and 71%. In both methods the inter- and intra-observer differences were not significant. ICCs ranged from 0.88–0.99 and were better for inter-observer compared to intra-observer reproducibility. Lower stump volumes were observed in Sitzia's method compared to water displacement volumetric method, with high ICC's (0.92–0.95) between both methods.
Although Sitzia's method systematically underestimates stump volume, it is a reliable and feasible alternative to the criterion standard test. To determine its validity to detect (longitudinal) differences in stump volume, follow-up research is needed in participants with recent amputations.
Introduction
Changes in stump volume influence the rehabilitation process in patients with lower-extremity amputations. 1,2 In the early phase of wound healing changes in volume rapidly occur due to oedema and atrophy. 1,2 These changes complicate the process of fitting a permanent prosthesis. The optimal time point to prescribe a permanent prosthesis is considered the moment at which the residual stump volume stabilizes. 1,3 Lilja and Öberg 3 revealed that this stabilization occurs at nearly four months after the initial amputation. However, valid studies on the time point of stabilization of stump volume are scarce and suffer from heterogeneity in technical methods, methodology, and patient characteristics. 1,3 In the chronic phases after amputation, measurements of stump volume are important if there are problems with prosthetic fit. Medical insurance companies ask for objective and quantitative data on volume changes before refunding adaptations. Moreover, to obtain results that can be compared among studies, reliable and valid data on stump volume are required as well.
Different methods to measure stump volume are available. As yet, the water displacement volumetric method is considered the criterion standard test. 4 A criterion standard test is a test or measure that is widely accepted and considered the best available at that time. 5 This method is based on Archimedes' principle and determines stump volume through the amount of water displaced when the amputated limb is placed into a pail of water. This method is reliable, valid, and non-expensive. 1,5–8 It is, however, time-consuming and cannot be used when the wound has not yet healed. 7,9,10 The second method, the one most often used, is segmental measurements of stump circumference. Circumferences of the stump are measured at different, predetermined, segments of the upper and lower part of the limb, usually 4 cm apart. 7,9,11,12 This method is easy to perform, applicable in any location, non-expensive, and convenient for the patient. There is, however, no consensus on its performance, and reliability and validity data are missing. More important, however, these are measurements of circumference, not of volume. Third, new technical instruments, such as computerized tomography, Magnetic Resonance Imaging, and laser techniques can be used as well. 6,13–18 These methods are not generally available, expensive, and rarely used in clinical practice.
Reliable methods to measure stump volume that are valid, feasible, and cost-effective are urgently needed. Meijer et al. 19 described an indirect volume measurement in patients with upper-extremity oedema. In this method segmental circumferential measurements were performed with a measuring tape with constant pull force. Next, the data were fitted into a formula of a truncated cone. 12 Compared to the water displacement volumetric method, this method was able to reliably and validly measure arm volume. If it is applicable and able to reliably and validly measure stump volume in the lower extremity as well, it might be the instrument clinicians are looking for.
Recently, Boonhong et al. 20 compared the water displacement volumetric method with the indirect volumetric measurement in transtibial amputees. The authors concluded that the indirect volume measurement is a reliable and valid method to measure stump volume in transtibial amputees. They, however, did not assess inter-observer reliability, although this is important in clinical practice where results should be interchangeable between therapists. Moreover, measurements were performed using the tibial tubercle as the start point of the circumference measurements. As such, they did not include the knee, whereas most below-knee prostheses do enclose the knee.
The aim of this study was, therefore, to determine the inter-observer reproducibility of the indirect volume measurement according to Sitzia's method in lower leg amputees, using a measurement tape with constant pull force. Measurements were performed in a standing position and included the knee. As such, intra-observer reproducibility and the validity of this indirect measurement were determined as well.
Patients and methods
Participants
From a hospital population of 149 adults with a transtibial amputation known at Rehabilitation Centre Tolbrug in ‘s-Hertogenbosch, The Netherlands, those fulfilling the Indirect volume measurement in transtibial amputees 21 inclusion criteria were selected. Inclusion criteria were: (i) A transtibial amputation for more than one year, and (ii) able to stand upright with or without support for at least 2 min. Patients with a recent operation, wound, or infection of the amputated leg were excluded. Patients with contractures of hip and/or knee were excluded as well. Written informed consent was obtained. The study was approved by the ethical board of the Rehabilitation Centre Tolbrug, ‘s-Hertogenbosch.
Experimental methods
Two different techniques to measure stump volume were applied in random order:
Segmental measurements of circumference with a special tape with constant pull force (Gulick measuring tape®, Creative Health Products, part number M22-C, 150 cm); Water displacement volumetric measurements.
Prior to the study, all measurements were standardized, to ensure that both observers assessed the participants equally. Randomization was based on a single sequence of random assignments using shuffled envelopes. 21
Circumferential measurements using a Gulick measuring tape
Because a prosthesis is most often used in the upright position, the participants were asked to stand upright with their hips and knees extended. A point 10 cm above the medial knee joint was marked. Therefore, the knee was first positioned in a comfortable, flexed position. Next, the medial knee joint was located by palpating the medial most proximal point of the tibial bone. While palpating this bony landmark, the knee was extended and a point 10 cm above was marked. This landmark equals the upper edge of a Kondylenbettung Münster (KBM)-prosthesis. From this landmark the lower leg was marked with pen dots every 4 cm downwards. Each observer marked the stump with a pen using a 50 cm fabricated ruler containing holes at every 4 cm. Segmental circumferential measurements with a Gulick measuring tape were performed at these marks, starting 10 cm above the medial knee joint. The measuring tape was placed below each pen dot. After performing the measurements, the dots were removed with an alcohol sponge.
To obtain the stump volume from the circumferential measurements Sitzia's formula,
12
derived from the formula of a truncated cone, was used:

Water displacement volumetric measurement
For the water displacement volumetric method, the participants were asked to stand with their amputated leg above the volumeter (Sammons-Preston, DeLuxe Partial Leg Volumeter®, 6 inches W × 24 inches D × 13 inches L). A plateau with the volumeter was raised through a hydraulic, smooth technique until the water reached the landmark at 10 cm above the medial knee joint. The water had a pleasant temperature. The water displaced by the transtibial amputation stump was collected separately in a cup with 10 cc calibration.
Both observers performed the water displacement measurement and the segmental circumferential measurements with a Gulick tape. Observer sequence was random. Randomization was based on a single sequence of random assignments using shuffled envelopes. 21 The observers were blinded for each other's measurements. To determine the intra-observer variability, the measurements were performed at the same time of the day on two different days. The time period between the two measurements was two weeks. The data were analyzed by a third person, not present during the measurements.
Statistical analysis
Reproducibility.
Reproducibility of the measurements between the first and second assessor (inter-observer) at the first and the second assessment, as well as the reproducibility of the measurements between the first and second assessment of both assessors (intra-observer) were calculated for both Sitzia's method and the water displacement volumetric method.
To quantify reproducibility, two different types of measurements can be distinguished with different interpretations: Measures of agreement and measures of reliability. Measures of agreement refer to the absolute measurement error (presented in units of the measurement of the instrument) that is associated with one measurement from one individual patient. 22 Measures of agreement provide insight into the ability of the two observers (or assessments in case of intra-observer reproducibility) to achieve the same value.
Measures of reliability refer to the relative measurement error, i.e., the variation between participants in relation to the total variance of measurements. They provide information on the ability of both observers (or assessments in case of intra-observer reproducibility) to differentiate between subjects in a group. 22,23
Agreement
The inter-observer agreement was quantified by calculating the mean difference between the two observers (1st–2nd observer) and the standard deviation (SD) of this difference. The intra-observer agreement was quantified by calculating the mean difference between the two assessments (1st–2nd assessment) and the SD of this difference. Subsequently, the 95% limits of agreement were calculated according to the method of Bland and Altman, 23 defined as the mean difference between two observers (or two assessments)±1.96 ∗ SD of this difference. These limits represent the range in which 95% of the differences between two observers (or two assessments) fall. In this situation the choice of extracting 1–2 or 2–1 is arbitrary. As such, the signs are irrelevant and should be ignored when interpreting the results. For the interpretation of the measurement error, the largest limit of agreement (either upper or lower limit) is most relevant.
In addition, the percentage of measurements between observers (or assessments) within the 5% difference of the stump volume was calculated. A difference of 5% stump volume or more was considered clinical significant because adding a stump socket gives an extra volume of approximately 5%. 1,3
Reliability
To quantify the intra- and inter-observer differences, paired sampled t-tests were performed. The level of significance was set at p < 0.05. Intra-class correlation coefficients (ICCs) were derived from random-effects two-way analysis of variance. By means of analysis of variance the variation in measurements is partitioned into the potential sources of variation: Observer differences, patient differences and random error. An ICC of at least 0.70 is considered to be satisfactory for group comparisons, and a value 0.90–0.95 for individual comparisons. 24
Validity
Validity is the degree to which a test (Sitzia's method) measures what it was designed to measure (in this study: stump volume). The stump volume measured by Sitzia's method was compared to the water displacement volumetric method (criterion standard test). 4 Validity was quantified by calculating the mean difference (a–b) between Sitzia's method (a) and the water displacement volumetric method (b) and by the standard deviation of this difference. Subsequently, the 95% limits of agreement were calculated. Paired sampled t-tests were performed to quantify the observed differences. The level of significance was set at p < 0.05. ICCs were derived from a random-effects two-way analysis of variance. All statistical analyzes were performed in Statistical Package for the Social Sciences (SPSS)®, version 12. 25
Results
From a hospital population of 149 adults with a transtibial amputation known at Rehabilitation Centre Tolbrug in ‘s-Hertogenbosch, The Netherlands, those 71 patients fulfilling the inclusion criteria were selected. Thirty-two patients gave their written informed consent, the other 39 refused to participate. Four participants dropped out before the study started (one died, one was amputated on the other side, and two participants were lost to follow-up). As a result, 28 patients finally participated. The patient characteristics are listed in Table I.
Main characteristics of the participants (n = 28).
SD = standard deviation.
Reproducibility
Agreement
Table II summarizes the results of the inter-observer agreement of both Sitzia's method and the water displacement volumetric method. Overall, the percentage of agreement between both observers exceeded 85%. At the first assessment, the percentage of measurements with inter-observer differences within 5% stump volume was larger for Sitzia's method compared to the water displacement volumetric method (96% and 89%, respectively), whereas at the second assessment this percentage did not differ between both methods (87% and 86%, respectively). Despite the high percentage of agreement the inter-observer differences in stump volume could be as large as 243.4 ml (14% of mean stump volume) for Sitzia's method, and 158.9 ml (9% of mean stump volume) for the water displacement volumetric method.
Inter-observer agreement. Mean and standard deviation (SD using either Sitzia's method or the water displacement method according to observer 1 and 2, followed by the mean differences between both observers, and the percentage of measurements within 5% of the stump volume.
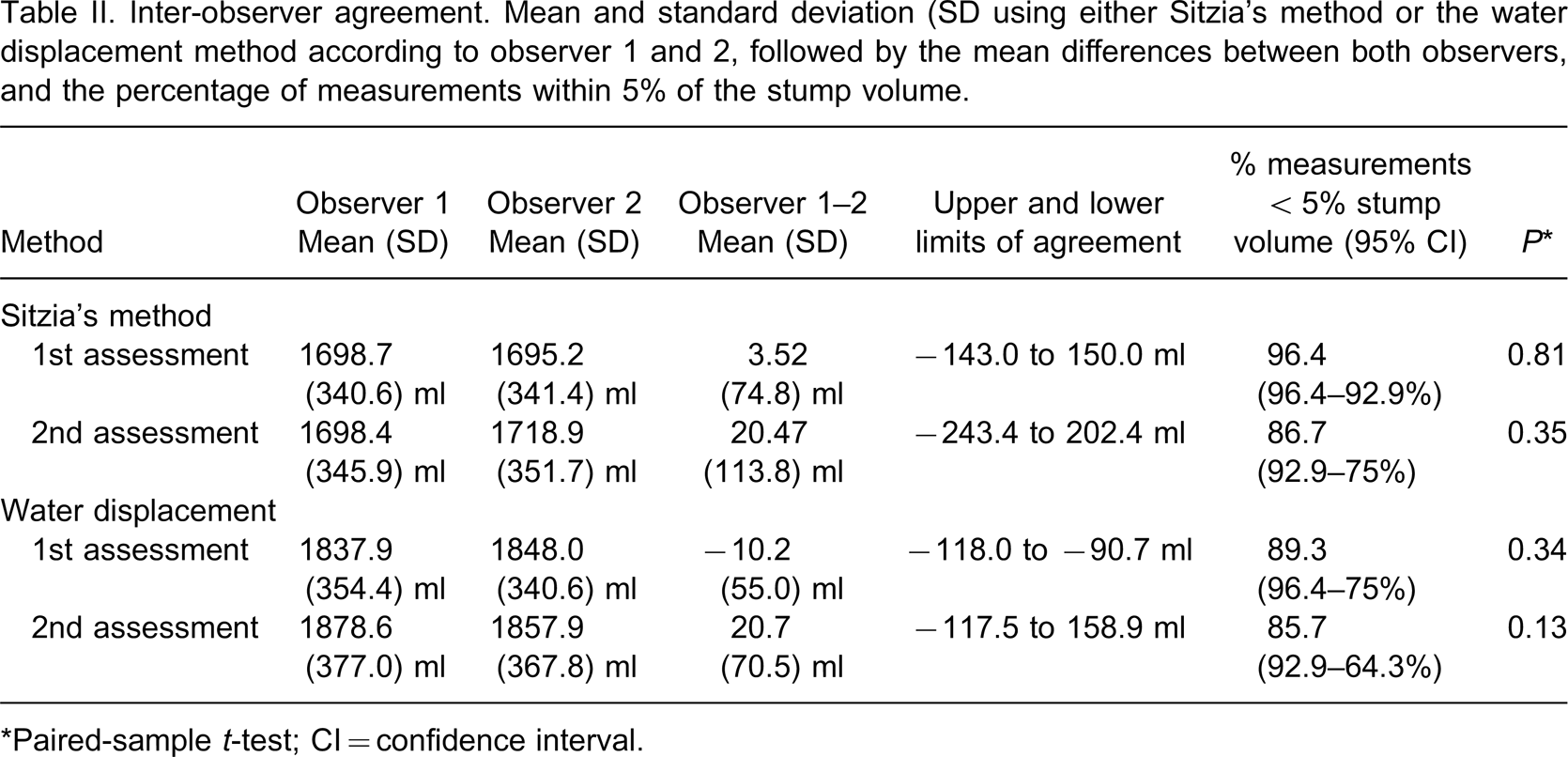
∗Paired-sample t-test; CI = confidence interval.
Table III summarizes the results of the intra-observer agreement of both Sitzia's method and the water displacement volumetric method. Overall the percentage of measurements with intra-observer differences within 5% stump volume was larger for Sitzia's method (71%) compared to the water displacement volumetric method (respectively 57% for observer 1 and 61% for observer 2). Intra-observer differences can be as large as 286.1 ml (17% of mean stump volume) in Sitzia's method and 392.5 ml (21% of mean stump volume) in the water displacement volumetric method. Overall, in both methods the intra-observer agreement was less compared to the inter-observer agreement.
Intra-observer agreement. Mean and standard deviation (SD), using either Sitzia's method or the water displacement method at the first and at the second assessment, followed by the mean differences between both assessments, and the percentage of measurements within 5% of the stump volume.
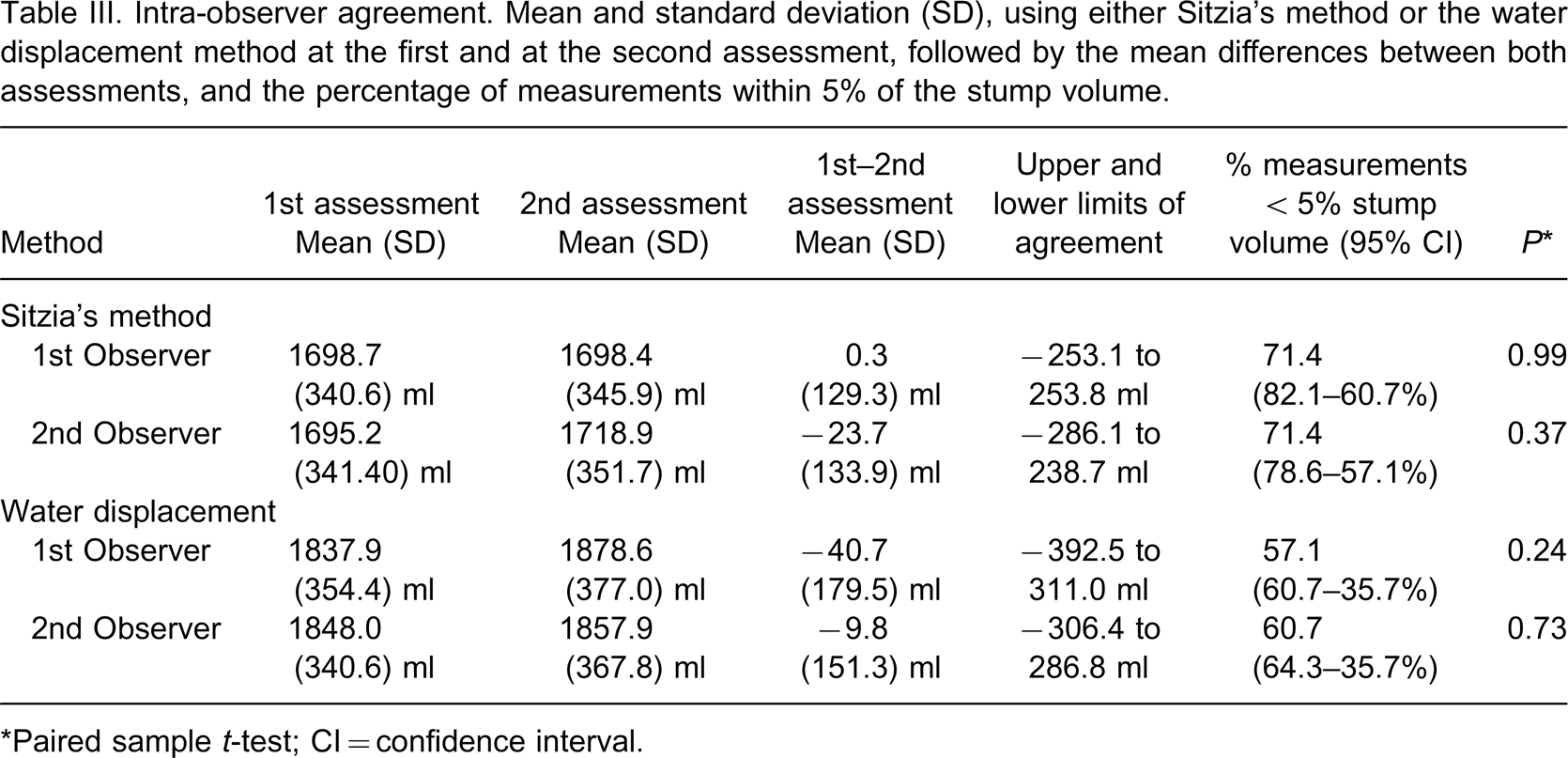
∗Paired sample t-test; CI = confidence interval.
Reliability
The inter- and intra-observer differences of both the water displacement volumetric method and Sitzia's method did not reach statistical significance (Tables II and III). The results of the analysis of variance for the inter-observer reliability are presented in Table IV, whereas the results of the intra-observer reliability are presented in Table V. ICCs ranged from 0.88–0.99. Overall, the ICCs for the intra-observer reliability were less (0.88–0.93) compared to the inter-observer reliability (0.95–0.99).
Inter-observer reliability; results of the analysis of variance.
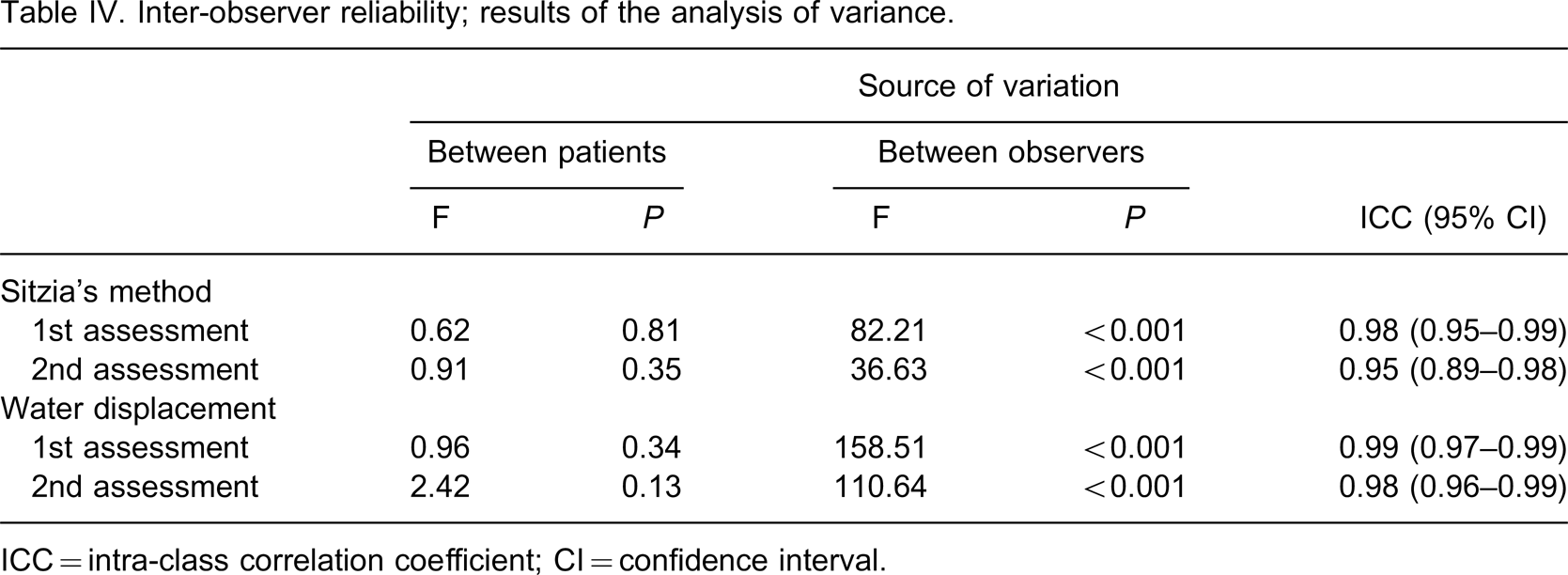
ICC = intra-class correlation coefficient; CI = confidence interval.
Intra-observer reliability; results of the analysis of variance.
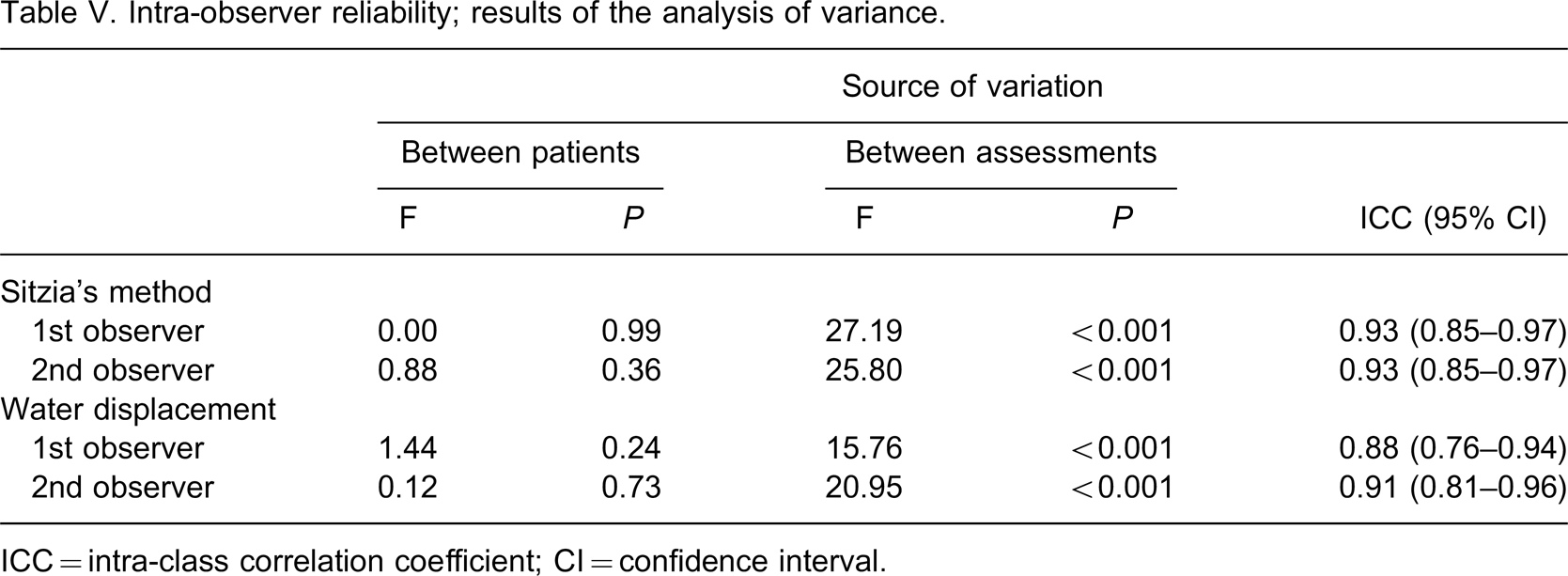
ICC = intra-class correlation coefficient; CI = confidence interval.
Validity
Table VI summarizes the results of the comparison between the Sitzia's method and the water displacement volumetric method, whereas Table VII shows the results of the analysis of variance. Although ICCs ranged from 0.92–0.95, the stump volume measured by Sitzia's method was consistently less compared to the volume measured by the water displacement volumetric method.
Mean, standard deviation (SD), and range of the first and second observer according to the volume measurement of Sitzia's method and the water displacement method, followed by the mean differences between both methods, and the paired sampled t-test.
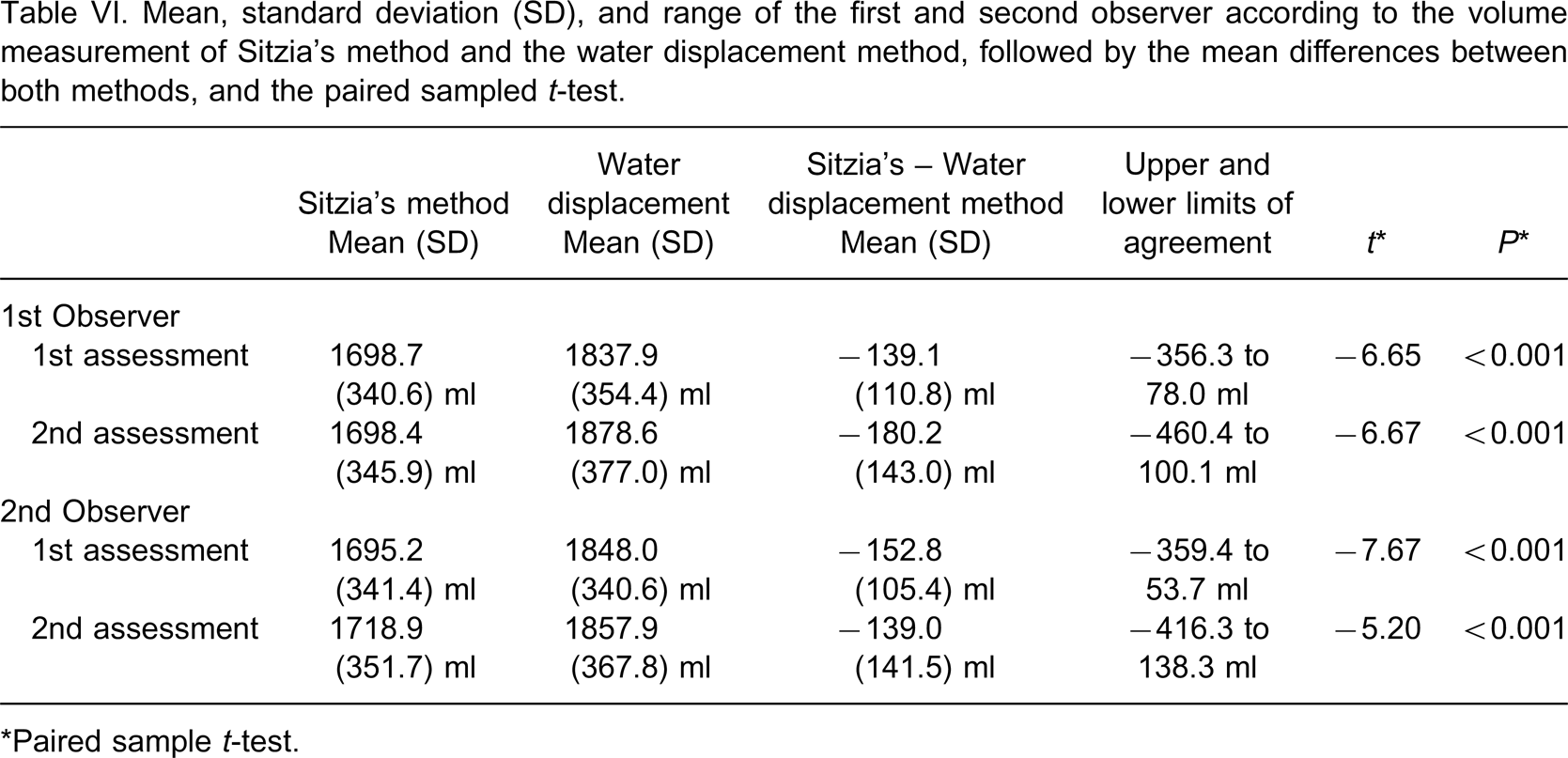
∗Paired sample t-test.
Validity; results of the analysis of variance.
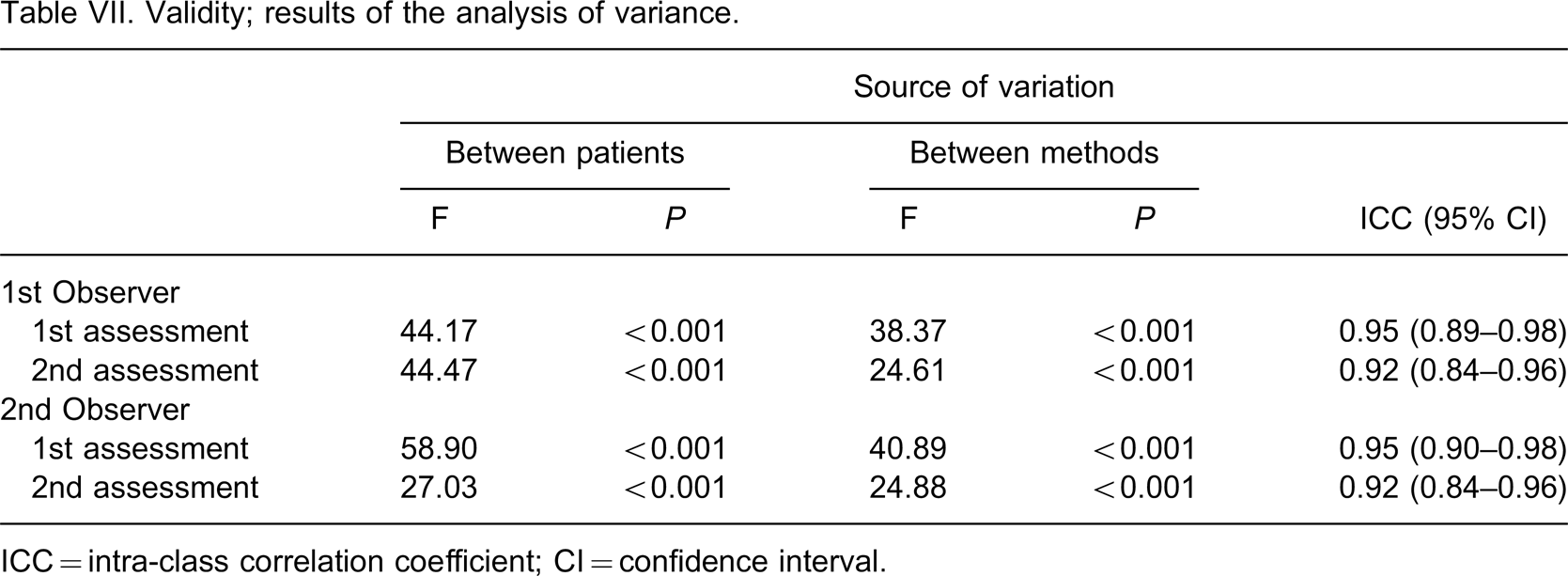
ICC = intra-class correlation coefficient; CI = confidence interval.
Discussion
In this study, stump volume in transtibial amputees was assessed using the indirect volumetric measurement according to Sitzia's method. The inter- and intra-observer reproducibility were determined and compared with the criterion standard test.
Inter-observer reproducibility
Although inter-observer differences of both the water displacement volumetric method and Sitzia's method were not significant, the limits of agreement showed that, if participants are assessed by two different observers, the differences in volume can be as large as 243.4 ml (14% of mean stump volume) for Sitzia's method and 158.9 ml (9% of mean stump volume) for the water displacement volumetric method. However, in 87–96% of the indirect volume measurements and 86–89% of the water displacement volumetric measurements, differences between observers did not exceed 5% stump volume. Considering the high percentage of agreement within 5% of stump volume, there must have been a few participants with large, clinically relevant, inter-observer differences. Analysis of the results showed that in five participants inter-observer volume differences exceeded 300 ml (= 5% of the mean stump volume). In these participants, a different amount of circumference measurements fitted into Sitzia's formula between both observers was responsible for the observed differences. After standardization of the amount of circumferences measurements, inter-observer differences did no longer exceed 5% stump volume.
ICCs were large for both Sitzia's method (0.98 and 0.95) and the water displacement volumetric measurement (0.99 and 0.98). As a result, volume measurements performed by two different observers can be used for group comparisons (ICC > 0.70), as well as for individual comparisons (ICC 0.90–0.95). 24
Considering the high percentage of measurements within 5% stump volume (>85%) and the large ICCs in chronic, stable, lower-extremity amputees, it should be possible to distinguish stump volume changes from measurement errors even if patients are assessed by different observers. However, both methods should be optimized through better documentation and standardization of performances (e.g., such as standardizing the amount of measurements), leading to even smaller limits of agreement.
Intra-observer reproducibility
Overall, the intra-observer reproducibility was less compared to the inter-observer reproducibility. Although the intra-observer differences did not reach statistical significance, differences in stump volume can be as large as 286.1 ml (17% of mean stump volume) for Sitzia's method, and 392.5 ml (21% of mean stump volume) for the water displacement volumetric method if participants, who are considered to have stable stump volumes, are assessed two weeks apart by the same observer. The intra-observer differences in stump volume were not clinically significant (i.e., did not exceed 5% of the initial stump volume) in 71% of Sitzia's volumetric measurements and in 60% of the water displacement volumetric measurements.
Variation in stump volume in six long-term amputees was responsible for the observed differences. These participants showed clinically significant changes in stump volume (>5% of their initial stump volume 1,3 ). Five of these participants cancelled their second assessment and were assessed 1–2.5 months later. Although none of these participants cancelled their second assessment due to stump problems (e.g., wounds, ulcers), these participants might have had changes in their mobility status affecting stump volume. Another participant appeared, after checking his medical record, to be formerly known with unexplained changing stump volumes. After removing these participants from the analysis, intra-observer differences did no longer exceed 5% stump volume (95 ml for Sitzia's method and 98 ml for the water displacement method). In contrast to the lower levels of agreement, both methods showed high ICCs (Sitzia's method 0.93; water displacement volumetric method 0.88–0.91), indicating that these methods can be used for both group comparisons and individual comparisons, but only in populations with stable stump volumes over time.
Validity
In line with former studies, 7,10,20 a strong relation was found between both methods. However, Sitzia's method consistently underestimated stump volume with volumes ranging between 139.0 and 180.2 ml. Considering the water displacement volumetric measurement as the criterion standard test, this means that Sitzia's method does not represent the actual stump volume in transtibial amputees. This is in agreement with the studies of Meijer et al. 19 and Kaulesar Sukul et al. 11 Both authors reported a slight underestimation of volume if Sitzia's method was used compared to the water displacement volumetric method. Other studies reported an overestimation of 2.5–11% of the actual volume by the indirect volumetric measurements. 9,10,20 However, only the study of Boonhong et al. 20 was performed in transtibial amputees. These authors, however, did not include the knee in their measurements. Moreover, measurements were performed while patients were seated. In this position, circumferential measurements in a horizontal plane at a right angle to the vertical axis of the lower leg are difficult to perform. As such, this might have affected the accuracy of their measurements. However, the underestimation of stump volume of Sitzia's method in our study may be due to our method of measurements as well. The lowest part of the stump was not included and, hence, did not contribute to the stump volume calculation in the formula. Moreover, the formula for calculating the volume of the stump, including the stump end, might be improved by approximating the stump end as a half ellipsoid. Approximating the stump end as a segment of a sphere might be less appropriate as some stump ends are too pointed for this approximation. More (mathematical) research is needed to define the best formula to determine the actual stumpvolume. As such, more research is also needed to study whether the formula of the indirect volume measurement technique can be adapted to different shaped stumps, e.g., bulbous or flabby stumps.
Nonetheless, our study indicates that Sitzia's method underestimates stump volume consistently and, hence, can still be valid to measure differences in stump volume. To determine the validity of the indirect volumetric measurement to measure differences in stump volume, future research should concentrate on longitudinal follow-up of patients with a recent transtibial amputation.
Twenty-eight participants were included in this study. The small sample size could have affected the precision of the limits of agreement and the standard deviations as well. Due to this small sample size it was not possible to determine the actual importance of all factors together. Such a four-way analysis of variance (with patient, observers, days and methods as the main variables and 11 interaction terms) can only be performed in much larger cohorts. Moreover, in view of the large standard deviation in both the intra-observer and inter-observer reliability it can be questioned if the water displacement method should be regarded the criterion standard test. However, as yet it is a widely accepted measurement and considered the best available at this time. 26
Conclusion
Although the indirect volumetric measurement according to Sitzia consistently underestimates stump volume, it is as reliable as the water displacement volumetric method. Moreover, it is easier to perform in clinical practice. Inter-observer agreement of both methods was large (>85%) and inter-observer differences not significant. As a result, volumetric measurements can be performed by two different observers, although there is a need to optimize inter-observer agreement by more extensively defining and standardizing its performance (e.g., standardizing the amount of measurements included in the formula).
Although large ICCs indicate that both methods can be used for group and individual comparisons, it was difficult to achieve the same stump volume at different assessments (main difference between two assessments > 0) in chronic transtibial amputees, leading to large limits of agreement. Due to this poor repeatability of both methods, both methods may have difficulty to measure small volume changes over time. However, more longitudinal research is needed to define its validity to detect changes in volume over time.
Footnotes
Acknowledgements