
Abstract
Comorbid personality disorder (PD) occurs in up to 70% of inpatients [1–4] and in 30–60% of psychiatric outpatients [5–7]. Rates may be lower in older patients [8] and in the community where the prevalence of PDs has been estimated to be between 6 and 10% [9].
Reported effects of comorbid PD on the outcome of Axis I disorder are varied. The severity of the personality dysfunction may be more influential on outcome than the existence of PDs per se, emphasizing the need to assess the severity as well as the presence of personality disorder [10]. Young adults have been found to have more complex PDs (abnormal traits across many dimensions) than older adults and might be expected to have worse outcomes [4]. Also, although treatments for Axis I disorders, e.g. for depression, are efficacious in people with PD, those with PD have more severe symptoms at the beginning of treatment and this difference persists so that they still have a higher level of symptoms than equivalent patients without PD at the completion of treatment.
While several reviews have concluded that the presence of PD adversely affects outcomes of Axis I disorders, the majority of these focused on anxiety and depression [11]. Part of the difference between outcomes for PD and non-PD patients may result from increased dropout rates in the PD group and poor interpersonal interactions in therapy [12] and their need for longer, more intense multimodal therapies [13].
Other studies report no difference or differential effects depending on the treatment [14]. Hirschfeld [15] did not find that personality disorders impeded treatment for depression but treatment of the depression could lead to improvement in the PD. Mulder reported no overall effect of PD on depression outcome except in patients with Cluster B PD who responded less well to tricyclics [16]. Increased lengths of stay in patients comorbid for PD have been reported by some [17] but not others [18]. Increased rates of readmission have been reported [19].
The interaction of age and PD on Axis I disorder outcome has received less attention. Agbayewa found that young PD inpatients had longer episodes of their Axis I disorder and poorer family relationships whereas the older inpatients had more severe episodes [20]. In a study of late life depression, people with PD were more likely to be admitted than those without PD [21]. PD may affect the frequency and mode of expression of Axis I disorders [22]. Reasons for these differences include different ways of measuring outcome, different populations, differing severity of the PD, different types of PD, different Axis I disorders, and defined age groups. All studies so far have examined discreet age cohorts and none has yet compared outcomes across age groups.
The aim of this paper was to examine the impact of comorbid PD on the outcome of a range of Axis I disorders in a sample of psychiatric inpatients aged 18 to 100. Our hypotheses were that PD comorbidity would be detrimental to outcome as regards symptoms, function and well-being, and that this effect would be more pronounced in the young. Additionally, we hypothesized that PD would be associated with an increased length of stay and greater rate of relapse and readmission.
Method
Sample
Participants were 238 consecutive consenting competent adult psychiatric inpatients (89 male, 149 female) admitted to an acute adult psychiatric unit or a psychogeriatric unit in one of two public hospitals. Adults aged less than 65 years (n = 134, range 18 to 64 years) were patients admitted to a 24 bed adult psychiatric unit located in Westmead Hospital, Sydney. Older participants (n = 104; age range 65 to 100 years) came from either of the eight bed psychogeriatric units located at Westmead Hospital or Prince of Wales Hospitals in Sydney where as a rule all older adults are admitted to the psychogeriatric units. The Westmead Unit is in a middle-class/working-class area and the Prince of Wales Unit caters for a more socio-economically diverse population with more patients from professional backgrounds. As equal numbers of patients came from each psychogeriatric unit there was a wide socio-economic distribution of patients. Admissions to public hospital psychiatric units are determined by geographical catchment area and are free. Private facilities in both areas admit patients of all ages and were not included in this study. For the purposes of this study participants were categorized into 3 age groups, young (18–40), middle-aged (41–64), and old (65+ years).
Participants were excluded from the study if they had a Mini-Mental State Examination (MMSE) score of less than 24, or showed significant cognitive dysfunction on the General Practitioner Cognitive Assessment instrument (GPCOG), Frontal Assessment Battery (FAB) or clock drawing tests, suffered from severe physical illness, were not proficient in English, were respite patients or had a length of stay (LOS) less than 3 days (details and references follow).
Measures
Psychiatric diagnoses were established using the Structured Clinical Interview for DSM-IV Axis I disorders [23]. The SCID-I has demonstrated reliability in adults [24] and has been used in older adult studies [25]. Cognitive evaluation included the Mini-Mental State Examination [26], the Frontal Assessment Battery [27], GPCOG [28], and the 10-point clock test [29]. Presence of a personality disorder was determined using the Structured Clinical Interview for DSM IV Axis II (SCID-II) Personality Disorders Personality Questionnaire [23], a semi-structured diagnostic interview for assessing the ten DSM IV (American Psychiatric Association, 1994) Axis II personality disorders, as well as depressive and passive aggressive personality disorders. Categorical diagnoses of specific personality disorders required participants to satisfy a certain number of criteria at an agreed level of severity from the 119 questions. The PDs are grouped into three clusters, Cluster A (‘odd, eccentric’) comprises paranoid, schizoid, and schizotypal; Cluster B (‘dramatic, erratic’) comprises antisocial, borderline, histrionic and narcissistic; and Cluster C (‘anxious’) comprises obsessive–compulsive, avoidant and dependent personality disorders. This questionnaire has demonstrated reliability and construct validity against DSM-IV criteria [30]. It includes all of the diagnostic criteria aligned with each PD type, ensuring no features are missed, as happens with a clinical diagnosis and accounts for the higher rates of PD when an instrument is used [31]. This instrument defines cases as subjects who fulfil sufficient criteria at sufficient intensity for a specific PD or PDs. Assessment of inter-rater reliability, performed between the two raters on 20 patients, was high: r = 0.85.
Outcomes were determined using measures of symptom severity, the Symptom Checklist-90 Global Symptom Index (SCLGSI)[32], function, the Global Assessment of Function (GAF)[33], physical and emotional morbidity, the SF-12 [34], and well-being, the Personal Well-being Index (PWI) [35]. The Sarason Social Support Questionnaire was used to measure the number of social supports (SSQ-N) as well as satisfaction with social supports (SSQ-S) [36]. The expanded version of the Brief Psychiatric Rating Scale [37,38] was used to assess psychiatric symptoms. Coping behaviour was measured using the brief COPE [39]. Relapse was defined as meeting criteria for Axis I disorder after at least eight weeks of recovery and readmission as admission to a psychiatric facility within the 12 month period after discharge.
Protocol
After complete description of the study to the subjects, written informed consent was obtained. Participants were assessed four times, shortly after admission and prior to discharge using structured interviews conducted by an experienced psychiatrist, and again at 6 and 12 months. The follow-up interviews were conducted by a research psychologist who was blind to all previous data. On admission participants were screened to make sure they met the inclusion criteria, the cognitive battery was completed and the SCID-I was administered to establish Axis I diagnoses. In order to avoid state effects on personality, the SCID-II was administered shortly before discharge when the Axis I symptoms had largely resolved, by the same psychiatrist. Relapse and readmission data were gathered from the subjects at the 6 and 12 month follow-up interviews and from hospital records.
Analyses
The statistical program SPSS 17 (Chicago, IL) was used to analyse the data. Two-sided tests with a significance level of 5% were used throughout. The distributions of categorical variables by age group were compared using chi-squared tests. Repeated measures analysis of variance was used to assess the joint effects of PD, age group and time (baseline, discharge, follow up) on the symptom and function scores. Linear regression models which adjusted for the effect of baseline scores were used to quantify the difference between PD and non-PD groups in key outcome variables at discharge and follow up. Multiple linear regression analysis was used to determine the relative contribution of significant variables to symptomatic outcome, functional outcome and readmission.
Ethics
The protocol was approved by the ethics committees of Westmead and Prince of Wales Hospitals and Sydney University.
Results
Demographics and relevant clinical baseline data are shown in Table 1. There was a high prevalence of PD across the spectrum of Axis I disorders with 67.2% of all patients being so diagnosed. When this was analysed by age, younger patients were far more likely to have complex PDs (39% versus 10% of old) while older patients were more likely to be free of PD (40% versus 26% of young). Of 116 patients with a primary Axis I diagnosis of mood disorders, 71 (61.2%) had a PD. Corresponding rates were: for schizophrenia 31/55 (56.4%), drug and alcohol abuse 11/13 (84.6%), anxiety disorders 4/4 (100%), eating disorders 13/14 (92.9%), and other disorders 30/36 (83.3%).
Demographic and clinical details of sample
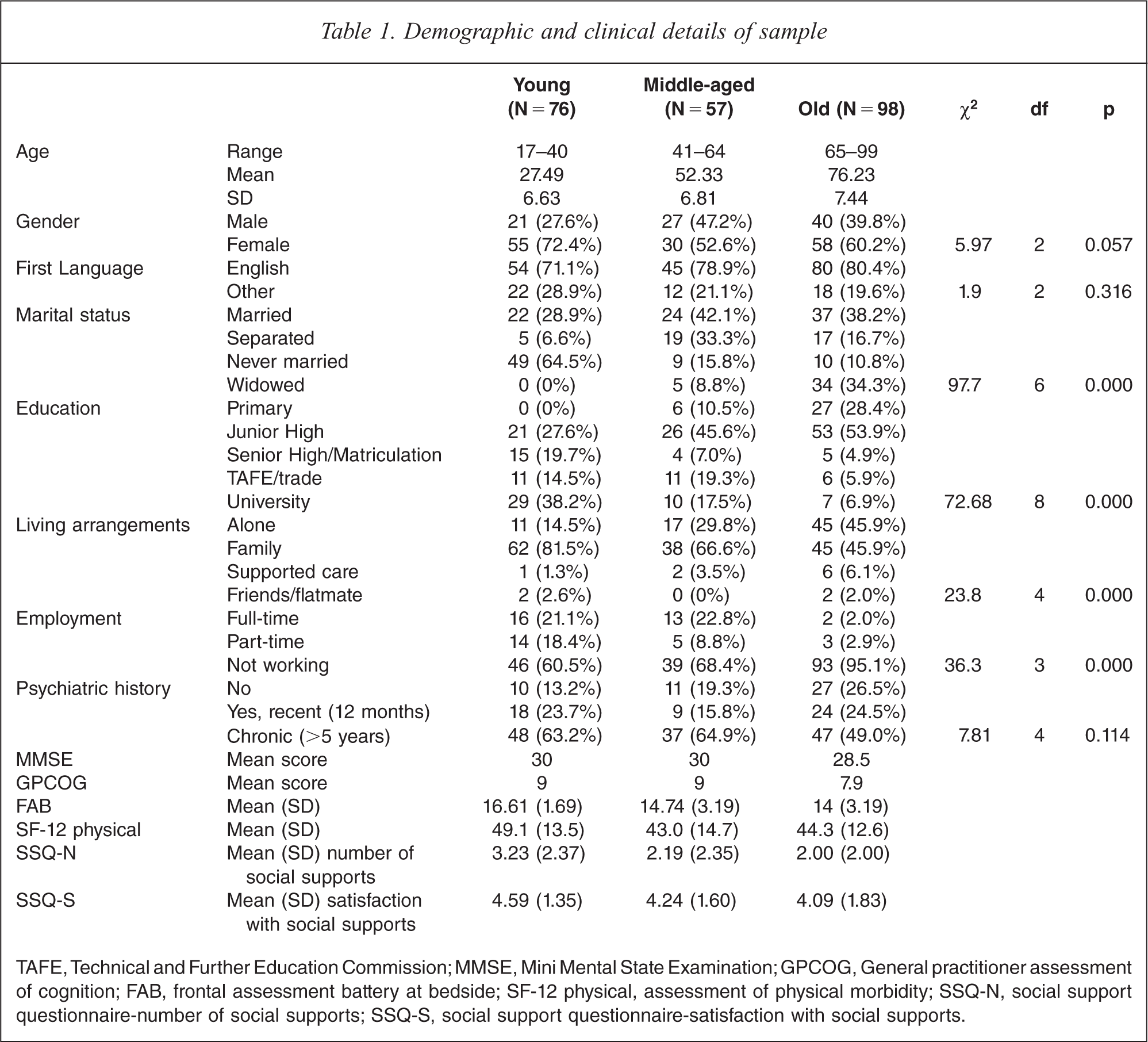
TAFE, Technical and Further Education Commission; MMSE, Mini Mental State Examination; GPCOG, General practitioner assessment of cognition; FAB, frontal assessment battery at bedside; SF-12 physical, assessment of physical morbidity; SSQ-N, social support questionnaire-number of social supports; SSQ-S, social support questionnaire-satisfaction with social supports.
Symptoms
Symptom outcome by age
Scores on all outcome measures improved over time for patients in each age group whether or not they had a PD (see Table 2) and all age groups improved at the same rate.
Scores for all subjects irrespective of PD status, comparing rates of change for three age groups (young, middle, old)
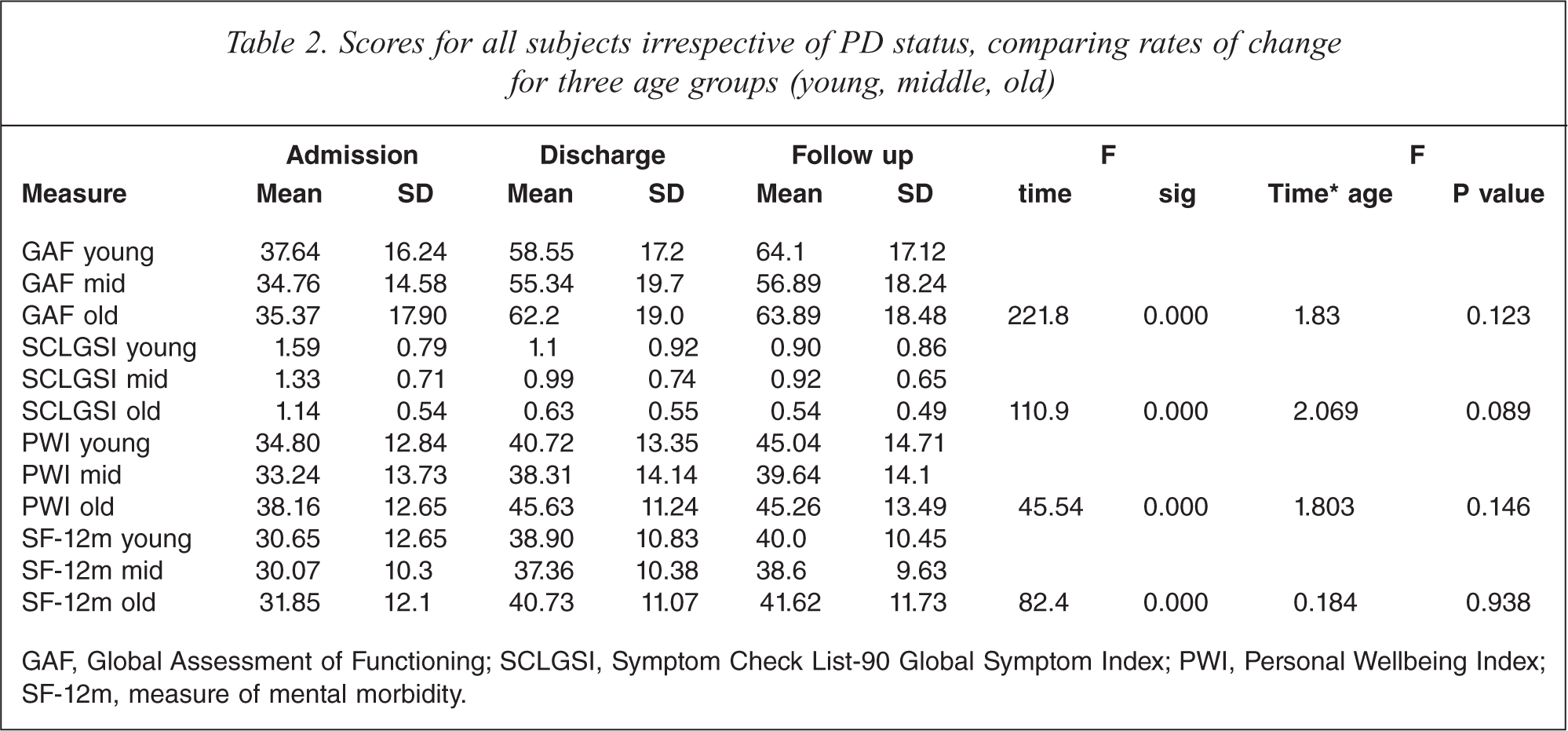
GAF, Global Assessment of Functioning; SCLGSI, Symptom Check List-90 Global Symptom Index; PWI, Personal Wellbeing Index; SF-12m, measure of mental morbidity.
Symptom outcome by PD
Over time both comorbid and non-comorbid groups improved in response to treatment as demonstrated by comparison of discharge and follow-up scores after controlling for admission scores (Tables 3 and 4). In absolute terms, for the whole group, PD patients fared worse over time on the SCLGSI than those without PD (F (2,454) = 4.08, p < 0.05) and after taking baseline scores into account, discharge and follow-up scores were worse in the PD group (at discharge, β = 0.186, t = 4.23, p < 0.001; at follow up, β = 0.277, t = 5.03, p < 0.001).
Admission, discharge and follow-up scores of key variables for three age groups for Personality Disorder (PD) and no Personality Disorder (No PD) groups
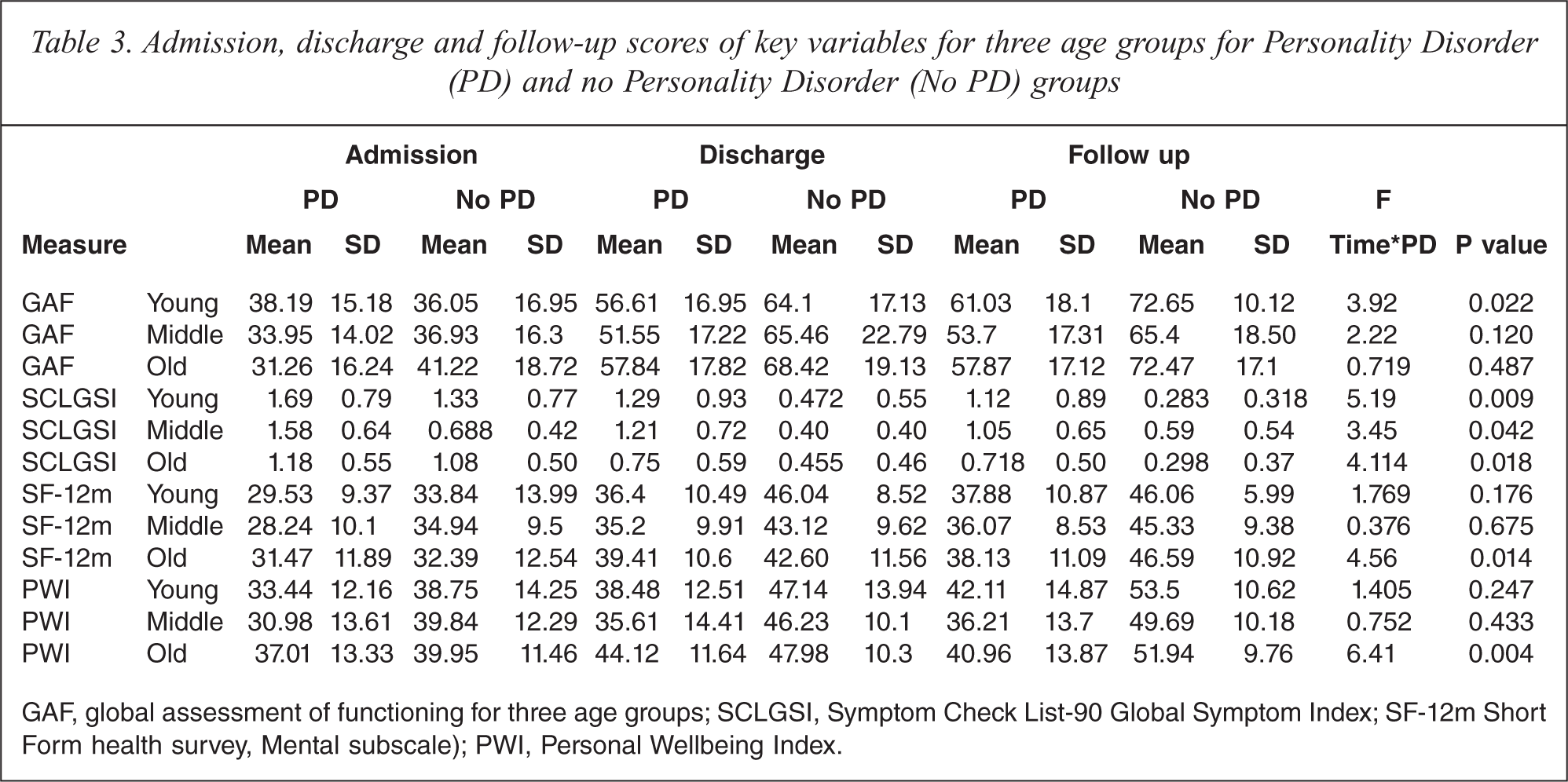
GAF, global assessment of functioning for three age groups; SCLGSI, Symptom Check List-90 Global Symptom Index; SF-12m Short Form health survey, Mental subscale); PWI, Personal Wellbeing Index.
Mean difference and standard error in scores between PD and non-PD groups adjusted for the effect of baseline scores by age group and overall
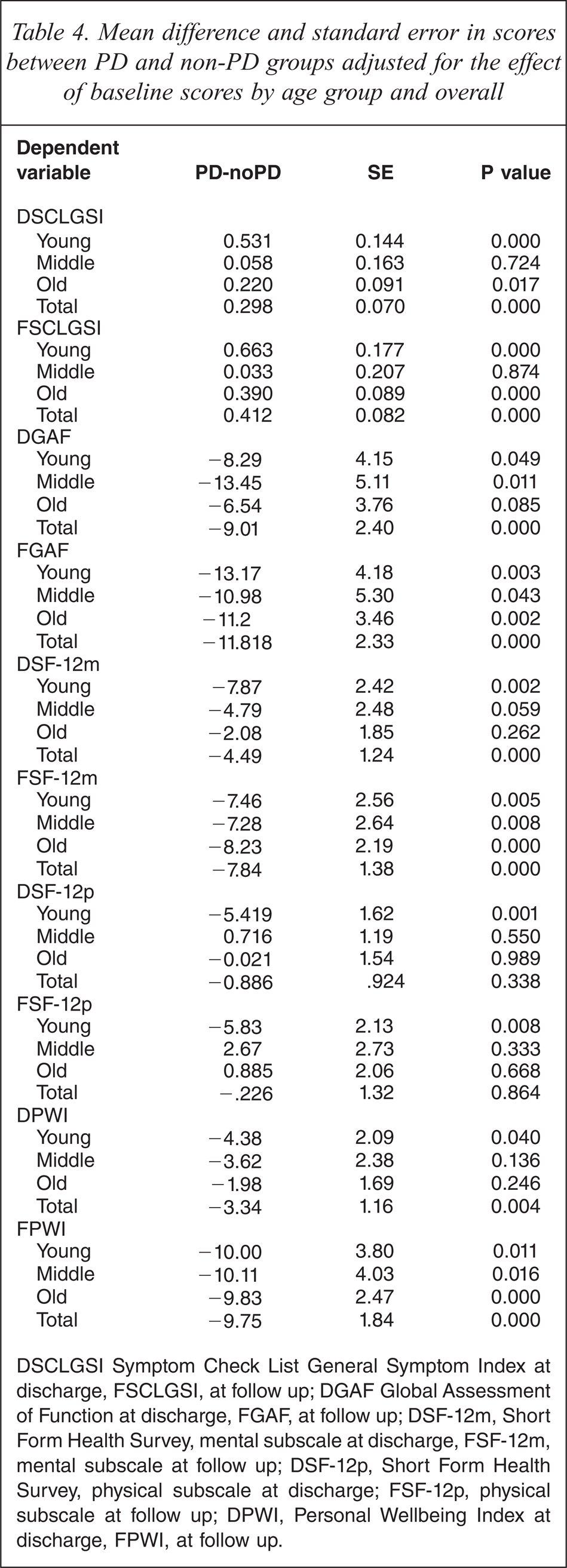
DSCLGSI Symptom Check List General Symptom Index at discharge, FSCLGSI, at follow up; DGAF Global Assessment of Function at discharge, FGAF, at follow up; DSF-12m, Short Form Health Survey, mental subscale at discharge, FSF-12m, mental subscale at follow up; DSF-12p, Short Form Health Survey, physical subscale at discharge; FSF-12p, physical subscale at follow up; DPWI, Personal Wellbeing Index at discharge, FPWI, at follow up.
Symptom outcome by age and PD
In all three age groups at all time points symptoms were more severe and function was lower in the personality disordered group. In the young and the old, symptoms as measured by the SCLGSI improved significantly less over time in PD than in non-PD patients. The middle aged group with PD also improved less over time but this was not as significant. When the interaction of PD, time and age was included in the analysis it was found to be non-significant for all measures except SCLGSI (F (4,446) = 4.53, p < 0.005).
Function
Function by age
Function, measured using the GAF, improved in the whole cohort over time (mean = 35 on admission to 58 on discharge to 63 at follow up) and there was no significant difference between age groups (F (4,452) = 1.83, p = 0.123).
Function by PD
Taking the whole group, PD patients’ function improved significantly less than the non-comorbid group (F (2,454) = 5.37, p < 0.05).
Function by PD and age
In the young and the old, rate of change was less, and discharge and follow up scores were worse for PD than non-PD groups. In the middle age group, rate of change over time was not significantly different but the PD group showed significantly worse function at discharge and follow up (Tables 3 and 4).
Morbidity and well-being
On the SF-12 mental sub-scale all subjects improved over time from a baseline mean score of 31 to 38 on discharge to 40 on follow up and with no statistical difference between age groups (for the SF-12m, F (4,452) = 13.2, p = 0.938). Likewise for the PWI, mean scores improved from 35 to 40 on discharge which was maintained at follow up. There was no difference between age groups (F (4,420) = 1.8, p = 0.146). When comparing PD and non-PD groups well-being was significantly poorer in the PD group (for SF-12m, F (2,454) = 5.53, p < 0.05; and for PWI, F (2,422) = 6.43, p < 0.005).
Age, PD and morbidity
In the young, change over time was not significantly different between PD and non-PD groups but the PD group had significantly worse discharge and follow up scores. In the middle age group change over time was no different for PD and non-PD groups but the outcome was worse in the PD group at follow up for both measures. In the elderly, there was less improvement for the PD group in the SF-12 mental subscale and PWI and both were worse at follow up.
Severity of PD
Comparisons were made between simple (1–2 PDs) and complex (PD diagnoses in all three clusters) PDs on all outcome measures and in all but physical well-being there was a gradient with no PD having better outcomes than simple PD and complex (qua severe) PD having the worst outcome (Figure 1).
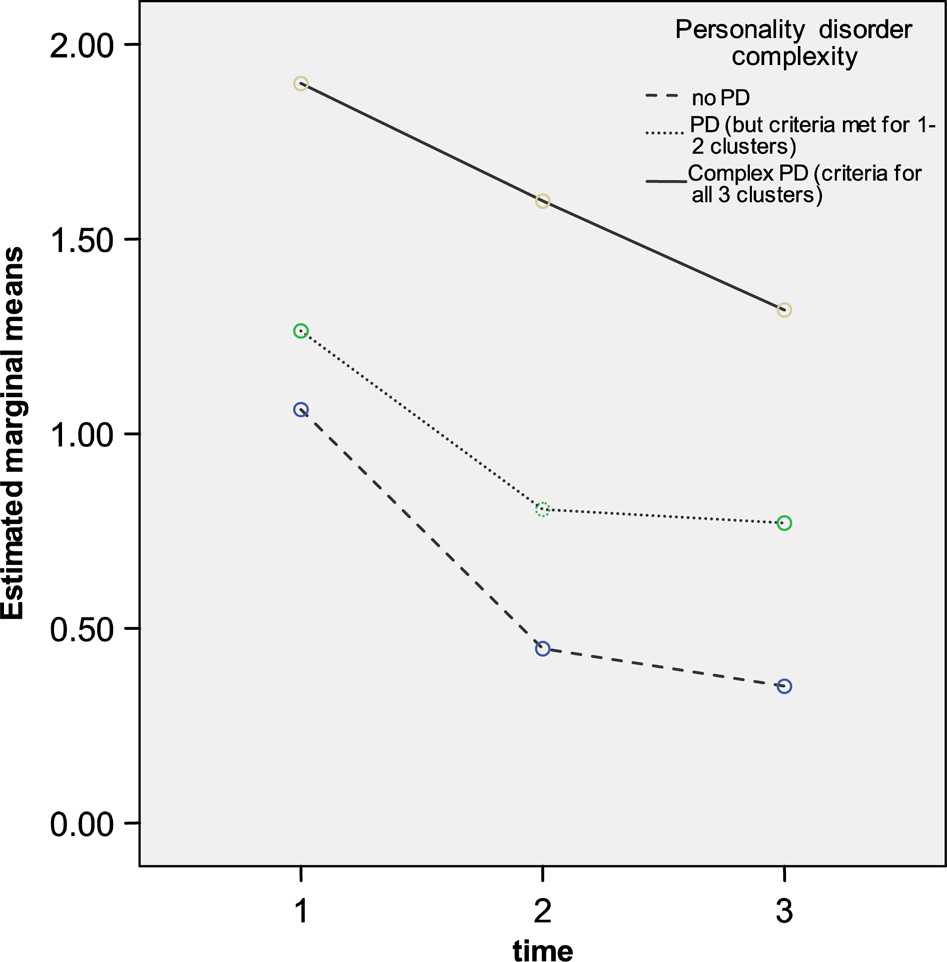
Change over time for SCLGSI of total population comparing no PD (N = 77), simple PD (N = 99) and complex PD (N = 53). Time 1, admission; time 2, discharge; time 3, 6 months. Significant difference between test conditions (F (4,452) = 3.44, p < 0.05).
Social supports
Satisfaction with social supports was significantly worse in the PD groups in all age groups (young age group (t = 2.2, df = 72, p < 0.05), middle age group (t = 3.5, df = 55, p < 0.001), old age group (t = 2.4, df = 102, p < 0.05)); the number of social supports was also significantly lower in young (t = 2.03, df = 72, p < 0.05) and older (t = 2.6, df = 102, p < 0.05) PD patients.
Relapse and readmission
Unexpectedly, the presence of a personality disorder made no difference to the length of stay for the sample as a whole as well as each age group independently. There were higher rates of relapse (47% versus 26%, p < 0.005) and readmission in the PD group (33% versus 19.2%, p < 0.05) as a whole than in non-PD patients. Readmission rates for PD patients were higher for each age group but this was only significant for older patients (t = − 2.90, df = 102, p (2-tailed) < 0.05).
Confounding variables
We considered the influence of age, gender, education, primary Axis I diagnosis, baseline BPRS, PD, physical comorbidity, chronicity, social supports and coping strategies on the findings.
A regression was performed with these as independent variables and follow up SCLGSI as the dependent variable. Only PD complexity predicted (worse) outcome (F (2,212) = 24.7, p < 0.001). When this was repeated with follow up GAF as the dependent variable, PD (F (2,212) = 14.8, p < 0.001), Axis I diagnosis (F (2,212) = 3.6, p < 0.05), and less education (F (4,212) = 3.02, p < 0.02) predicted worse outcome. With readmission as dependent variable only chronicity (B = 1.35, df = 1, p = 0.006) and Axis I diagnosis (B = 0.994, df = 1, p = 0.016) predicted readmission.
Regressions were repeated for each of the three age groups. Symptomatic outcome (SCLGSI) at follow up was predicted only by the presence of a PD in young (F (1,64) = 7.76, p < 0.05) and elderly (F (1,83) = 14.8, p < 0.005) but not in the middle group. Functional outcome was predicted by chronicity in the young (F (2,64) = 3.4, p < 0.05), and middle (F (2,41) = 4.9, p < 0.05) and schizophrenia in the old (F (2,83) = 4.5, p < 0.02), and by PD in young (F (1,64) = 3.5, p < 0.05) and old (F(1,83) = 18.7, p < 0.000) age groups. In the elderly PD was a significant factor predicting worse outcome on all three measures of outcome. Data are available on request.
The Axis I diagnosis of schizophrenia and to a lesser extent depression predicted readmission in all age groups (B = 1.01, df = 1, p < 0.02); chronicity predicted readmission in young (B = − 21, df = 1, p < 0.000) and old (B = − 2.74, df = 1, p < 0.03); and PD predicted readmission in the elderly (B = − 1.6, df = 1, p < 0.05).
Discussion
We confirm the literature that comorbid personality disorder is common in the inpatient population though slightly less so in the older group [2]. Comorbidity is particularly common in certain groups such as those with drug and alcohol abuse, and eating disorders; however, it is seen in all diagnoses and across the demographic spectrum. Severe personality disorders were more common in the young group, and the old group had a higher proportion of patients without comorbid personality disorders. Outcomes for the middle group were less affected by the presence of the PD. This lends weight to reports that personality disorder tend to ‘mellow’ with age and that the old are less likely to meet criteria for more than one personality disorder [40] although this has not been confirmed by others [41], though how older age is defined varies, often as low as fifty [42].
In all three age groups symptoms and function were significantly worse in the PD groups at all time points, confirming our hypothesis. Moreover, the more severe the PD, the worse the outcome. Importantly, this did not mean that PD patients were less responsive to treatment. In some instances responses paralleled the non-PD group, as evidenced by change scores, but they remained more symptomatic and never reached the level of recovery of the non-PD group. These effects might explain the conflicting results of different studies, some reporting no effect of PD and others reporting a negative effect. However, when taking account of the baseline scores there was still a significant difference between the comorbid and the non-comorbid groups on several measures, especially post discharge. In addition, when other possible determinants of outcome were entered into a regression analysis PD was found to be the most significant determinant of outcome, with Axis I and chronicity making lesser contributions.
Our outcome results suggest that there is a more significant effect of personality disorder on symptomatic and functional outcomes in the young and to a lesser extent in the older groups than in the middle age group. Our findings fit with descriptions of waning of effects of personality in middle age [1] and a slight re-emergence in old age [43]. Perhaps the answer is that patients with personality disorders have more resources in middle age but start to lose them as they become older. While the number of social supports as measured by the SSQ-N in young and old comorbid patients was lower in those with PD than in non-PD patients, numbers were similar in the middle aged.
We confirmed that the negative effect of PD in all age groups was more pronounced following discharge, when previously non-significant differences became significant [44]. This is also seen in our relapse and readmission data where all PD patients, especially older PD patients, were significantly more likely to relapse and be readmitted to hospital. That Molinari and Marmion [45] found no difference in relapse rates between PD and non-PD elderly patients might be explained by their focus purely on affective disorders.
These effects were seen over a wide variety of diagnoses, not just the mood disorders. The absence of significant social support particularly in the young and the elderly PD groups may account for some of their deterioration post discharge where the presence of personality disorders certainly has a significant effect [44]. Our young and elderly PD groups had fewer social supports and less satisfaction with social supports than the middle group.
Contrary to our hypothesis, length of stay was not affected by the presence of PD. This is likely due to other factors such as the preference of the treating consultant, comorbid physical illness, severity of Axis I disorder, and accommodation availability.
Strengths of this study are that it was prospective, longitudinal, incorporated a battery of structured interviews, and included a moderately large patient population. Limitations include bias in the number of patients who were excluded or who refused, and by there being more women in the sample. Reasons for admission may differ by age, the young being more likely to be admitted purely for psychiatric disorders and the elderly for a combination of psychiatric and physical morbidity. Also, patients may have been readmitted to other facilities, but this is unlikely as public patients are only admitted to the hospital in their own area and all patients were interviewed regarding readmission at 6 and 12 months. Medication variables were not controlled for and scales were devised for young adults and have not been validated in the elderly. Finally, the same interviewer made both Axis I and II diagnoses. However, structured interviews reduced the risk of bias, and subsequent interviews were completed by blind raters. It could not be discounted that on discharge when the SCID-II was completed that some residual symptoms of the Axis I disorder could still be influencing the diagnosis of PD. However, it was felt to be minimal, moreover research has found that a diagnosis of PD even in the presence of Axis I pathology has significance [46].
Footnotes
Acknowledgements