
Abstract
Recent epidemiological studies have revealed very high rates of antipsychotic, antidepressant and anxiolytic and sedative-hypnotic drug use among Australians [1–3]. These large-scale analyses supplement previous data across a number of settings demonstrating higher rates of use in those over 60 years, with highest rates in those 80–95 years of age (Figure 1). This issue is of growing concern, given the increasing size of the elderly population and the greater vulnerability of older people to adverse effects of drugs and to interactions among the multiple drugs often prescribed. On the basis of these new data and significant previous findings, we argue for the urgent need to review psychotropic prescribing among the elderly on the grounds of safety and cost [4].
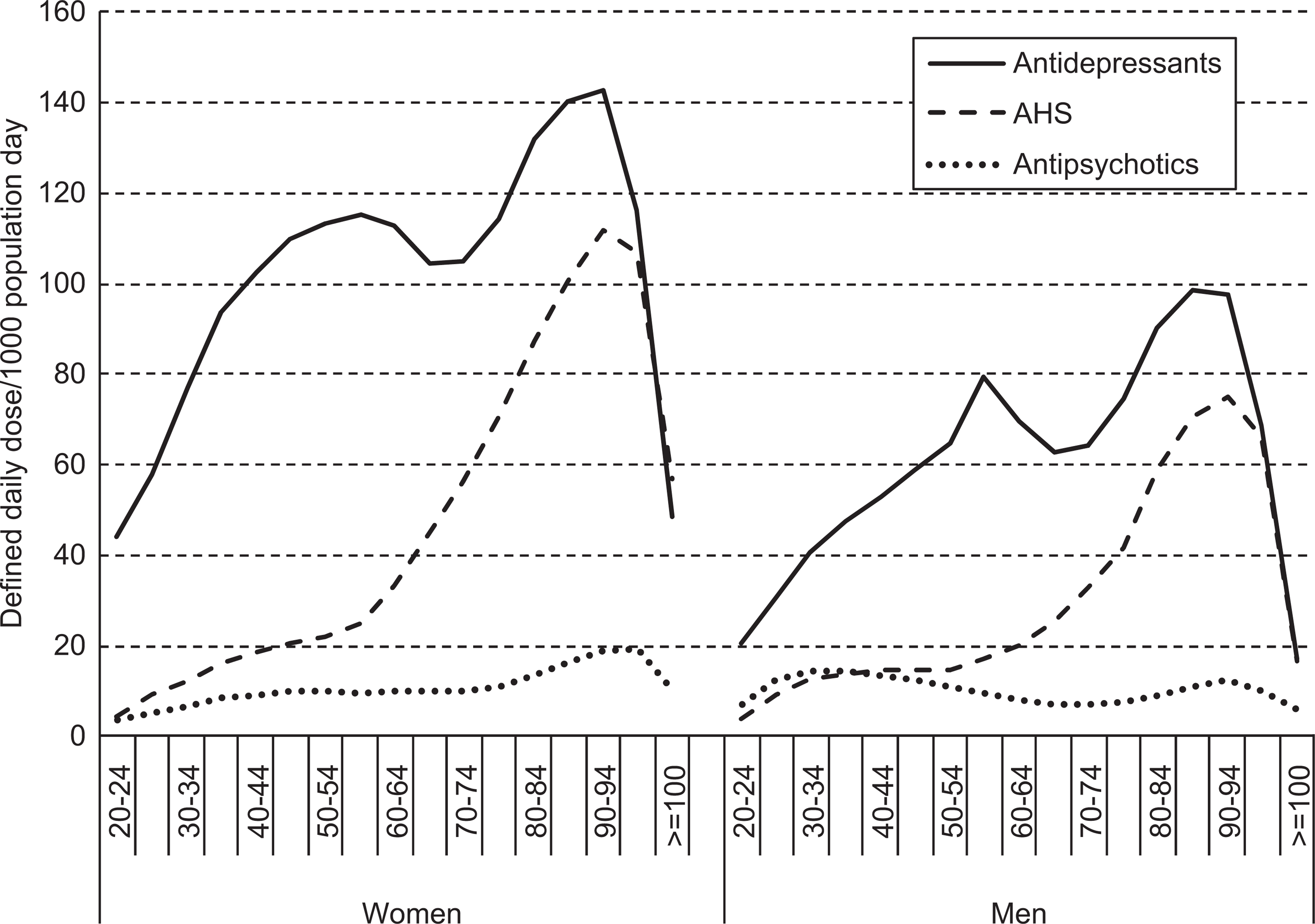
Dispensed use (define daily dose/1000 population/day) of antipsychotics, antidepressants and anxiolytic, sedative-hypnotic (AHS) drugs by gender and age.
We examined dispensed prescription data from Medicare Australia for three main drug classes. The amount of drug supplied was standardized using the defined daily dose (DDD) per 1000 population per day for all drugs with an anatomical therapeutic chemical code starting with N05A, N05B, N05C or N06A. The DDD is established by the World Health Organization Collaborating Centre for Drug Statistics Methodology [5]. It corresponds to an estimated mean daily dose of the drug when used for its main indication in adults. The number of Australians in each gender and five year age group was used to standardize the DDD by population.
Patterns of psychotropic drug use among older Australians
Antipsychotics
Atypical antipsychotic (AAP) prescribing to older Australians increased during the 2000s, with olanzapine and risperidone dominating [3]. Population-standardized use among women was almost double that of men in these older age groups. The DDD utilization rates for olanzapine were ten times greater among women aged 90–95 than those aged 20–25. Actual rates of use were probably even higher because people over 60 are more likely to be prescribed lower doses (2.5 mg and 5 mg olanzapine).
One possible explanation for these striking differences is that women are over-represented in aged care settings where psychotropic prescribing is common and often inappropriate [6] though this is subject to regional variation [7,8]. Age-related increases in prescribing parallel the exponential rise in dementia prevalence after age 60, with prevalence in many residential aged care facilities (RACF) exceeding the community rate ten-fold [9,10]. Despite increasing questions surrounding the risks and benefits of AAP use in the elderly [11,12], there has been an increase in their use in some aged care facilities, albeit at low doses [7,8].
Antidepressants
Antidepressant use increased 41% between 2002 and 2007 (SSRIs 44%, venlafaxine 75%) [1]. Utilization of antidepressants showed a bimodal distribution with an early peak among those in their late fifties. Their dispensed use exceeded the estimated prevalence and self-reported treatment of affective and anxiety disorders in the community. Of particular concern was the very high rate of prescribing among those over 80. Newer, more tolerable antidepressants are now the first line treatment and are possibly prescribed to treat symptoms of depression and/or anxiety that do not reach the threshold for a clinical diagnosis. Rates of prescription remain higher than prevalence would suggest, even if subsyndromal cases are included.
Depressive symptoms are common in people with dementia and among those in RACFs but the efficacy of antidepressants in these groups is not established. Antidepressants, including those introduced after the tricyclic ‘era’, are linked with significant side-effect issues in the elderly including falls and delirium [13]. Furthermore, among older patients admitted to nursing homes, the risks of death and femur fracture associated with typical antipsychotics, antidepressants and benzodiazepines are comparable to or greater than the risks associated with atypical antipsychotics [14].
Anxiolytics, hypnotics and sedatives
Use of anxiolytic, hypnotic and sedative (AHS) drugs was concentrated in those aged over 65 years highest in those aged 85–89 years and higher in women than men (after adjusting for age) [2]. The most commonly prescribed agents among older people were temazepam, nitrazepam, and oxazepam. Older people were generally prescribed lower dose formulations and use of temazepam and oxazepam reflects guidelines to use smaller doses of drugs with minimal hepatic oxidation. However, these patterns of use are inconsistent with recommendations for short-term use and the evidence for lower rates of anxiety disorders in older age groups [2].
Could insomnia explain this pattern? Rates of insomnia in the elderly are 30% higher than in the general adult population [15], whereas AHS use is 500% higher. Increased rates of benzodiazepine prescription (e.g. 20% [16]) among patients with dementia could explain some of this use. AHS use in older people is associated with cognitive impairment, delirium and an increased risk of falls and accidents [16,17].
Towards more rational psychotropic prescribing for older Australians
These studies align with results from other Australian studies in demonstrating very high levels of psychotropic drug prescribing among older people, particularly older women and those over 80 years of age. There are substantial doubts as to the efficacy and safety of these patterns of prescribing, which in the case of AAP and AHS appear to be inconsistent with evidence-based guidelines.
The financial cost of the use of these drugs is also considerable: the cost to the Pharmaceutical Benefits Scheme (PBS) was AU$702 million in 2007–2008, more than the Medical Benefits Scheme (MBS) costs for all mental health services combined ($551 million) [18]. If current patterns persist, these costs will rise with the increasing numbers of people with dementia in the Australian population. Direct and indirect health costs will also increase alongside adverse events (e.g. falls causing fractures), other medication-related morbidity and the potential for drug interactions.
We need a better understanding of the reasons why these drugs are used in older Australians. This would involve increased auditing in order to describe the characteristics of users and the reasons for use. Individualized drug utilization data would enable an examination of dose titration, drug switching and co-prescribing practices. It is likely that much of the increased usage occurs in residential aged care facilities, where poor prescription practice has been noted for decades. In these settings demand for antipsychotics is probably significantly driven by the high prevalence of behavioural and psychological symptoms of dementia (BPSD) [19]. Antipsychotics for BPSD can be safely stopped safely in most cases [12,20] and replaced by better care practices to reduce prescription rates [21]. Although the consensus is that non-pharmacological approaches, incorporating good nursing practice, are the cornerstone of good dementia care [22], major barriers to this standard are the cost and skills of the required workforce [23]. Existing reviews of psychotropic medication in many, if not most, facilities are too infrequent [21] to address safety and efficacy concerns, such as use in sub-syndromal states or failure to trial non-drug alternatives.
Quality use of psychotropics is also required in community settings to ensure the most cost-effective use of the mental health dollar. This involves education around appropriate indications for psychotropic drugs and realistic stopping rules for drugs that are no longer needed. We need to encourage review and cessation of unnecessary medication and better awareness of, and access to, non-pharmacological interventions.
In summary, when we consider the current level of psychotropic prescribing for older Australians, there is a pressing need to know more about the epidemiology, sociology and optimal use of medicines that in many cases may be unnecessary, costly or potentially harmful.
Footnotes
Acknowledgements