
Abstract
Keywords
Access to, and utilization of, relevant information sources is essential in order to make informed decisions about health threats. However, there is a dearth of research exploring how people with schizophrenia obtain information on health matters. There are also high rates of comorbid physical illness and reduced longevity in people with schizophrenia [1–9]. A 13-year follow-up study [1] found a standardized mortality ratio of 298 for people diagnosed with schizophrenia. Most of the excess deaths were accounted for by recognized medical disorders, especially cardiovascular disease. People with schizophrenia also have poor access to primary health care and exhibit poor adherence to general medical treatment [1,7,9]. Numerous studies have examined lifestyle factors as possible contributors to comorbid medical illness and found that, compared with the general population, people with schizophrenia are more likely to consume a diet higher in fat and lower in fibre, take less exercise, smoke cigarettes, be overweight, and have harmful levels of illicit substance use [2,10–13]. Therefore, there is a critical need for people with schizophrenia to receive evidence-based and appropriately communicated health information.
In this initial study we aimed to broadly explore the amount of health information people with schizophrenia obtain from various sources and the level of trust they invest in those sources, compared with people attending a general practice setting who did not report a diagnosis of schizophrenia.
Methods
Participants
Participants in this cross-sectional survey (n = 309) were part of a larger study (n = 382) we carried out examining a range of health issues, including pandemic influenza risk perception. This paper reports on results related to participants’ use of, and trust in, health information sources. Volunteers between the ages of 18 and 65 (inclusive) were recruited from mental health settings in the Australian Capital Territory (ACT) and 13 general practices (purposively selected on the basis of geographic diversity of location in the ACT) over a four month period (July to October 2009). The mental health settings included two inpatient psychiatric units, four community mental health centres, two private psychiatric practices and a residential psychiatric rehabilitation unit. Flyers and information brochures describing the study were placed in foyer areas and waiting rooms, and patients were invited to participate in the study. Those who were not capable of providing informed consent or not having the capacity to complete the questionnaire were excluded from the study.
The study discussed in this paper involved two groups of participants: (i) people attending mental health settings who had been diagnosed with schizophrenia (SCZ) by their treating psychiatrist (who was contacted by the researchers), and (ii) people attending a general practice (GP) setting. No participants in the GP group reported suffering from schizophrenia.
There were 238 participants in the GP group. Out of a total of 144 participants recruited from the mental health settings, 71 had received a diagnosis of schizophrenia (50 from community mental health centres, 12 from one of the psychiatric inpatient units and nine from the rehabilitation unit). Socio-demographic characteristics are shown in Table 1.
Socio-demographic characteristics with statistical differences between SCZ and GP groups
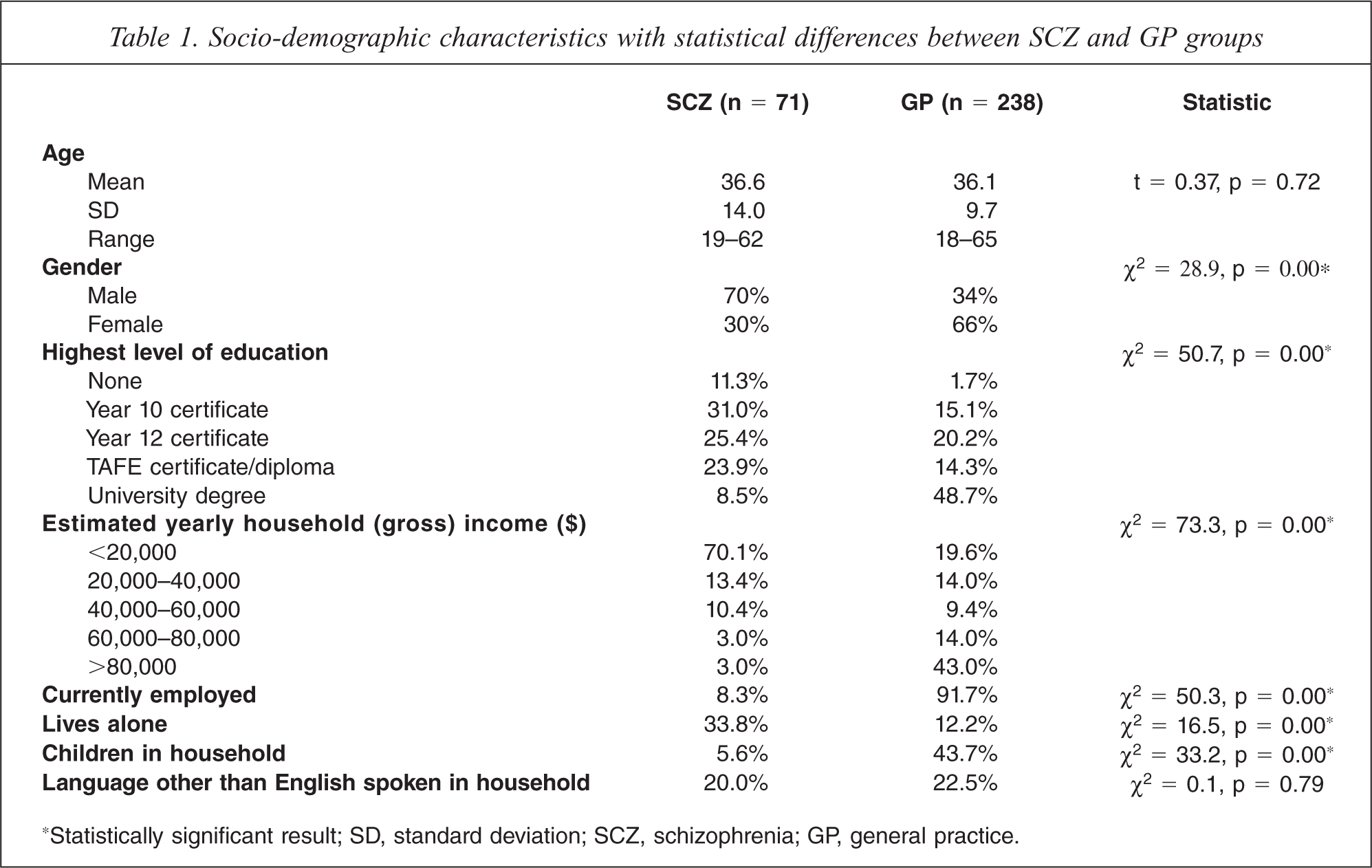
*Statistically significant result; SD, standard deviation; SCZ, schizophrenia; GP, general practice.
A naturalistic sample of patients with mental illness was sought for which an adequate comparator could be found. People with schizophrenia not linked with health services were seen as being less likely to be accurately diagnosed and more difficult to recruit. General practice attendees were viewed as a reasonable comparator group: accessible and likely to respond to the invitation to be involved in our study.
Participants in the SCZ group all had regular contact with a psychiatrist or psychiatric registrar. In the hospital inpatient unit this was at least several times a week, and not less frequently than third monthly in the community mental health centres and rehabilitation centre. The general practices were predominantly small urban group practices. Ascertainment of the precise nature and frequency of services accessed by participants in either group would require a further survey and this was seen as beyond the scope and focus of the current study, but could be the subject of future research.
Ethics approval was obtained from the Australian National University, ACT Health, and Calvary-ACT Health Human Research Ethics Committees.
Measures
Participants were invited to complete a questionnaire which included items on how much information on health matters they obtained from various sources including doctors, the Internet, television, radio, magazines, newspapers, and family and friends. They responded on a 5-point Likert scale. Possible responses included: 1 = none, 2 = a little, 3 = a moderate amount, 4 = a lot and 5 = an extreme amount. They were then asked to rate their level of trust in each of these sources as providers of health information, using the same scale. These measures are similar to those employed in other studies examining risk perceptions of outbreaks of respiratory infection, which have used 5-point Likert scales when assessing information sources accessed and levels of confidence in them [14,15].
Statistical analysis
All analyses were carried out using SPSS version 17. Preliminary analyses of the data were performed to ensure that there were no violations of the assumptions for the statistical tests employed. The data were examined for significant differences between the SCZ and GP groups using an independent t-test, chi-square test, Mann-Whitney U test and binary logistic regression. Odds ratios were obtained after Likert responses were dichotomized into either (i) ‘none or a little’ or (ii) ‘a moderate, a lot or an extreme amount’ of information obtained from, or trust in, a given source. Ordinal regression was not used because the proportional odds assumption/test of parallel lines was violated. In addition to crude scores, adjusted odds ratios were calculated, controlling for age, gender, socioeconomic status, living alone, children in the household and non-English language spoken in the home. These variables were considered likely to have an impact on choice of information source used since they were also viewed as potential important predictors of pandemic influenza risk perception and protective behaviours against contracting influenza (in the larger study).
Correlation between amount of information obtained from a given source and the level of trust in it was calculated using Spearman's rho.
Within-group multivariate analyses using logistic regression were performed to explore the relationship between demographic characteristics (as independent/predictor variables) and a significant amount of information obtained from, or trust invested in, each information source (dependent variables). As with the between-group regression analysis, the dependent variable responses were dichotomized into ‘none or a little’ versus ‘a moderate, a lot or an extreme amount’. The best predictor of amount of use and trust was sought for each information source.
Results
The mean age in the SCZ group was 36.6 years (SD = 14; range = 19–62) and 36.1 years in the GP group (SD = 9.7; range = 18–65). In the SCZ group 70% of participants were male compared with 34% in the GP group. As might be anticipated there was also a disparity between the two groups in estimated household annual income and highest level of education achieved, with almost 50% of GP attendees reporting attainment of a university degree compared with less than 10% in the SCZ group.
An independent t-test showed no significant difference between the SCZ and GP groups in terms of age but chi-square tests confirmed significant differences for gender distribution, employment status, living alone, estimated household annual income and highest level of education. There was no statistical difference for non-English language spoken in the home. Differences were controlled for as potential confounders in regression analysis.
As shown in Table 2, the most commonly used sources for obtaining a significant amount of information on health matters for participants in the SCZ group were, in rank order, doctor, family and friends, and TV. More than 50% of people in this group reported obtaining at least a moderate amount of information from each of these sources. By comparison, for GP attendees, most health information was derived from, in rank order, a doctor, the Internet, and family and friends. Approximately 60% of participants with schizophrenia reported obtaining at least a moderate amount of information from a doctor compared with about 80% in the case of GP attendees. Only 35.2% of people in the SCZ group reported using the Internet as a significant source of health information compared with 66.5% for GP attendees.
Comparison of SCZ and GP groups in the reporting of at least a moderate amount of information obtained from a given source
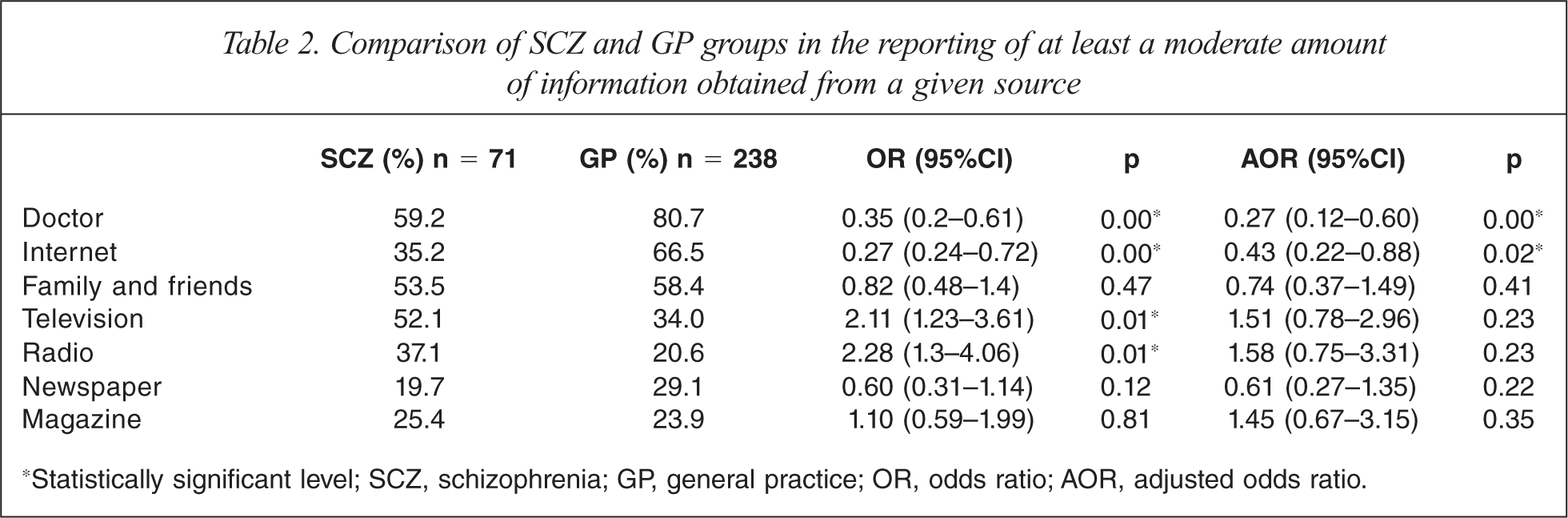
*Statistically significant level; SCZ, schizophrenia; GP, general practice; OR, odds ratio; AOR, adjusted odds ratio.
Mann-Whitney U tests (Table 3) indicated significant differences between SCZ and GP groups in the amount of health information obtained from a doctor, the Internet, television and radio. With respect to trust there were significant differences between the two groups only for doctor and the Internet.
Differences between SCZ and GP groups in amount of health information obtained from, and level of trust in, a given source
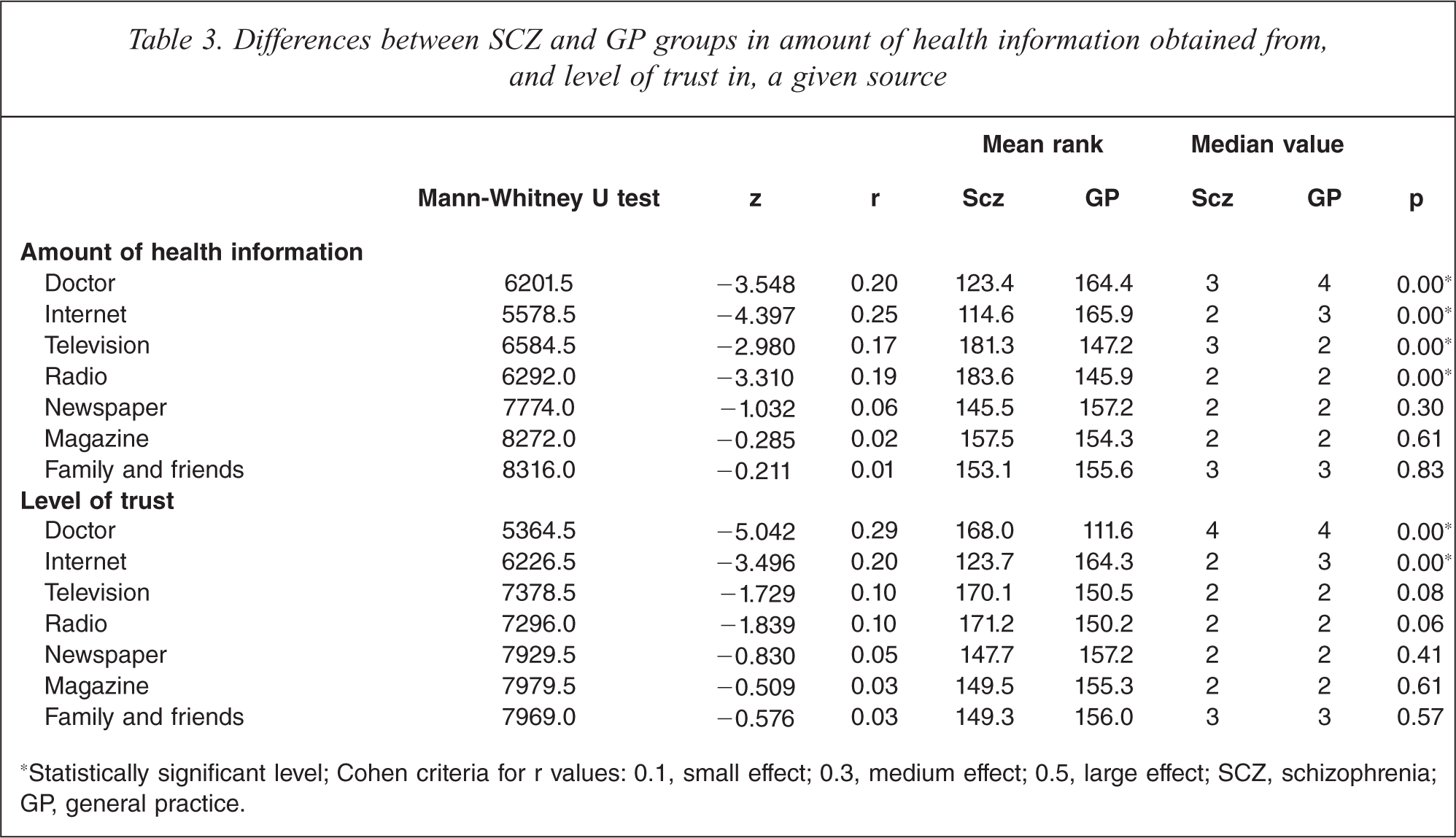
*Statistically significant level; Cohen criteria for r values: 0.1, small effect; 0.3, medium effect; 0.5, large effect; SCZ, schizophrenia; GP, general practice.
As revealed in Table 2, regression analyses indicated that people with schizophrenia were only about a quarter as likely to obtain at least a moderate amount of information from their doctor compared to GP attendees, and less than half as likely to significantly access health information from the Internet. Compared with GP attendees, people with schizophrenia were significantly less likely to trust their doctor (Table 4).
Comparison of SCZ and GP groups in the reporting of at least a moderate amount of trust in a given source
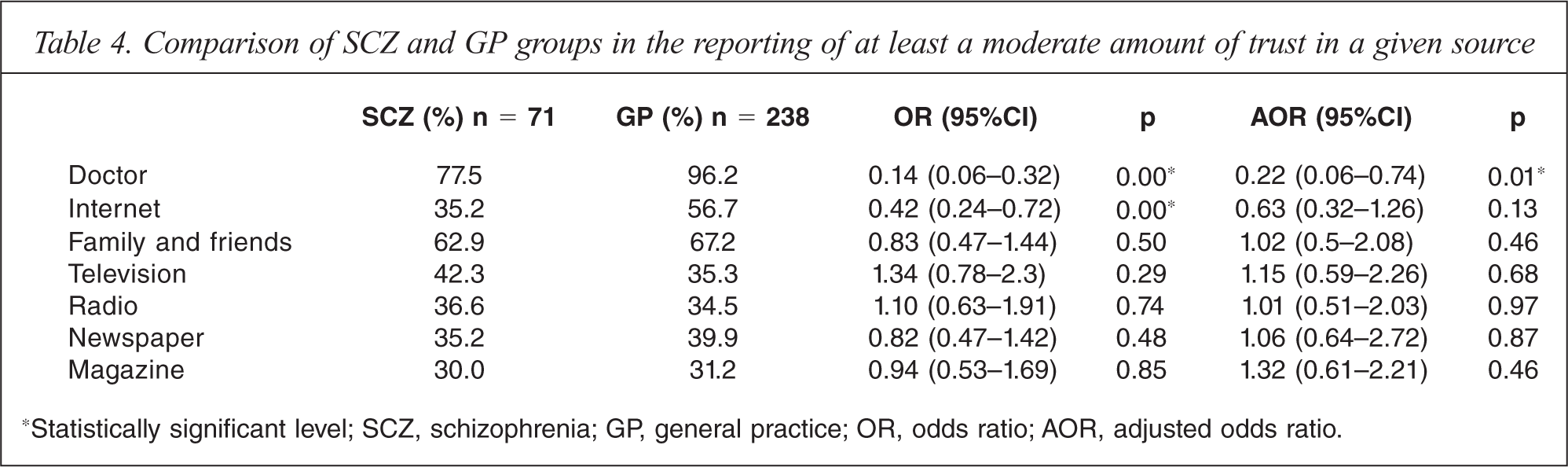
*Statistically significant level; SCZ, schizophrenia; GP, general practice; OR, odds ratio; AOR, adjusted odds ratio.
Results of the within-group multivariate regression analyses are shown in Table 5. In the SCZ group: living alone increased almost five-fold the likelihood of obtaining at least a moderate amount of health information from television; a higher level of education made it more than twice as likely that a person with schizophrenia would trust the Internet as a health information source; a higher estimated yearly household income was associated with a greater likelihood of trusting newspapers; and women with schizophrenia were close to seven times more likely to trust family and friends as providers of health information than men with schizophrenia.
Best predictor of a significant amount of use or level of trust for each information source (within-group multivariate regression analysis)
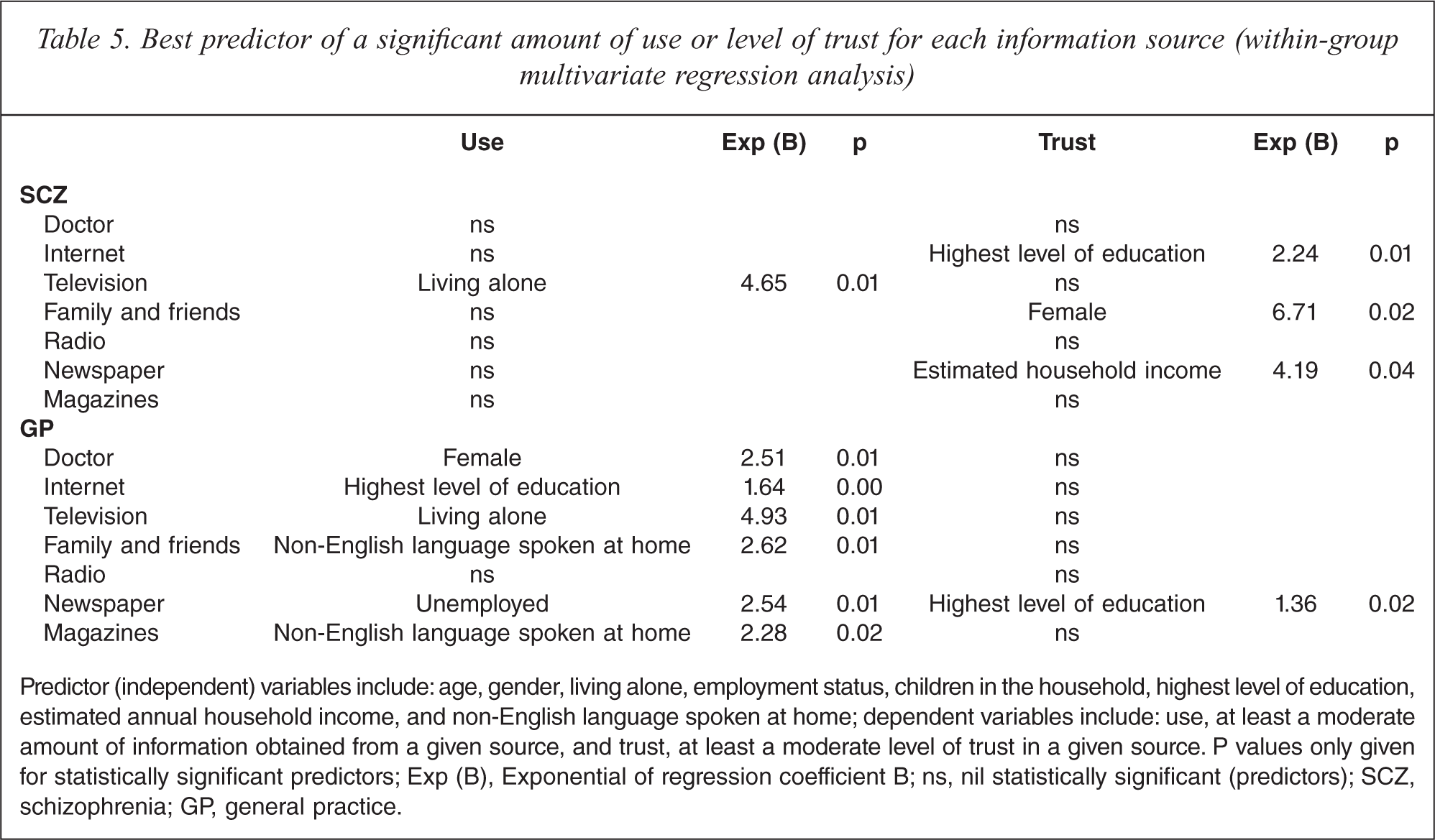
Predictor (independent) variables include: age, gender, living alone, employment status, children in the household, highest level of education, estimated annual household income, and non-English language spoken at home; dependent variables include: use, at least a moderate amount of information obtained from a given source, and trust, at least a moderate level of trust in a given source. P values only given for statistically significant predictors; Exp (B), Exponential of regression coefficient B; ns, nil statistically significant (predictors); SCZ, schizophrenia; GP, general practice.
In both groups there was a statistically significant positive correlation (Table 6) between the amount of information obtained from a given source and the level of trust invested in it, except for newspaper in the schizophrenia group.
Spearman's correlations between amount of use of a given information source and the corresponding level of trust
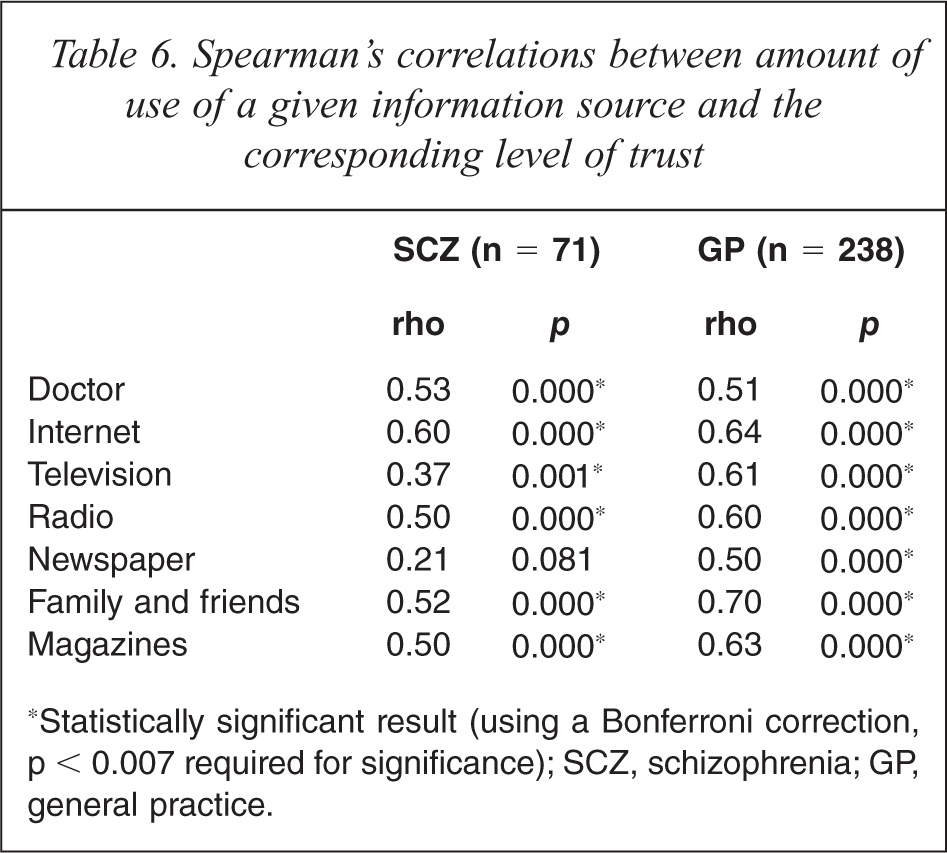
*Statistically significant result (using a Bonferroni correction, p < 0.007 required for significance); SCZ, schizophrenia; GP, general practice.
Discussion
Use of health information sources
People with schizophrenia are exposed to health threats arising from both their significant vulnerability to comorbid medical disorders as well as risks and challenges associated with their mental illness. Therefore, the disparity in our study between the SCZ and GP groups in the use of doctors and the Internet as a health information source is of concern.
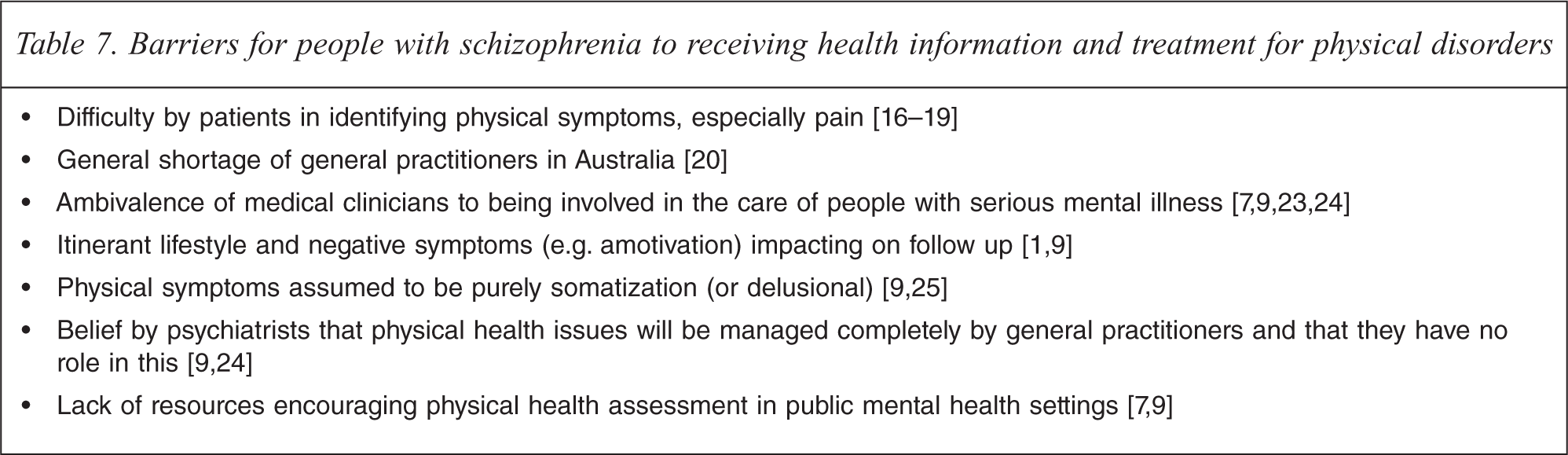
People suffering from schizophrenia need to be able to receive relevant and optimally communicated health information from their doctor(s). However, significant barriers exist. There is evidence that they may experience difficulty in identifying or communicating a physical (or mental) symptom, on which to seek information. A study of 102 consecutive patients admitted to the acute medical care unit of a psychiatric hospital found that less than a quarter could accurately describe the symptoms of their physical illness [16]. This was particularly true of pain, consistent with evidence from other studies for greater pain tolerance in people with schizophrenia [17–19]. Another important obstacle is a shortage of GPs in some regions [20]. With respect to our study, the ACT has the lowest GP bulk billing rate of any state or territory in Australia as well as a relative shortage of GPs [21]. This is particularly relevant given that a large majority of participants in the SCZ group in our study reported an estimated annual household income of less than $20,000. There is also evidence of inequality with respect to physical health care in people with schizophrenia compared to those without this illness. For example, people with schizophrenia attending a general practice, even though as a group they have been found to be more likely to suffer from hyperlipidemia, are less likely to have a recent record of their cholesterol level or to have received a script for a statin (cholesterol lowering agent) compared to people without schizophrenia [22]. See Table 7 for a summary of barriers to treatment (a component of which is the provision of health information).
Barriers for people with schizophrenia to receiving health information and treatment for physical disorders
There has been an expansion of the Internet as an accessible, dynamic and interactive information source for mental and physical health issues [26]. Furthermore, the Internet has been promulgated as enhancing mental health literacy and promoting engagement in mental heath programmes, especially for those who do not feel comfortable seeking, or cannot access (e.g. due to rural or remote locations), face-to-face professional help [26]. Close to two thirds of survey respondents in the general population of the USA reported using the Internet for any reason, and health information seeking was by far the most commonly reported online activity [27]. In contrast, our finding of the relative lack of use of the Internet for acquiring health information by people with schizophrenia places them at a potential disadvantage. Although it seems plausible that higher education might predict the use of the Internet as a source of health information, this was only the case for the GP group, a finding consistent with prior research [27,28]. Seeking to understand the barriers and facilitators to accessing the Internet for people with schizophrenia remains a worthwhile endeavour.
Trust in information sources
The comparatively lower level of trust in doctors by participants with schizophrenia in our study warrants further exploration. Trust has long been recognized as a core element of the therapeutic relationship between a doctor and a patient [29–32] and is a significant contributor to therapeutic outcomes [33]. For example, low levels of patient trust in their doctor have been shown to be associated with poor perceived effectiveness of care, reduced adherence to management recommendations, less doctor–patient contact and poorer continuity of care, less utilization of health care services, greater likelihood to seek a second opinion and worse health by self-report [34–38]. Unfortunately, however, there has been a lack of successful interventions which have been measurably shown to significantly improve trust by patients towards their doctors [39]. Given the persecutory ideation, guardedness, asociality and other negative symptoms experienced by many people with schizophrenia, the challenges in developing trust in the doctor–patient relationship are considerable.
In our study, the proportion of participants in the SCZ group who reported placing a significant amount of trust in the Internet was only about half that of the GP group (35.2% versus 66.5%). The Internet was also lower in the rank order of significantly trusted sources in the SCZ group. The Mann-Whitney test found a significant difference between the two groups with more trust invested in the Internet by participants in the GP group. However, when potential confounders were controlled for in the regression analysis this difference did not reach statistical significance.
Perhaps there is justification in having a degree of healthy reservation in the level of trust placed in the Internet as a health information source. For example, a study evaluating 21 popular websites on depression [26] found that their overall quality was poor, identifying misinformation, misleading information and a lack of balance. The authors highlighted a need for quality assurance mechanisms and suggested the possibility of developing intelligent search engines that use algorithms linked to ‘gold standards’.
Finally, while fully utilizing the technical marvels of electronic health resources, it is important also to ensure that the humanity and sense of value of patients be supported and not replaced [40].
Correlation between amount of use of and level of trust in information sources
In our study a significant amount of the variance in the quantity of information gained from a given source (in both groups) was explained by variation in the level of trust invested in that source (Table 6). This was especially so for family and friends in the GP group (r2 = 0.49). It makes intuitive sense that if you trust a source you are more likely to use it, and conversely, that if you use a source and find it reliable you are likely to develop trust in it. However, this correlation is not always the case. A study of 810 college students aged 18–24 [41] found that these young people reported obtaining most of their health information from sources they did not particularly trust, such as friends, the media, and the Internet. On the contrary, health professionals were highly trusted by these students yet were among the least common providers of health information. Furthermore, another study [27] revealed that although physicians remained the most highly trusted source and respondents reported wanting to access them first to obtain specific health information, when asked what they actually did, almost 50% reported going online first as opposed to 10.9% who indicated consulting their physician first.
Limitations
Limitations of this study include recruitment bias (self selection bias; purposive non-probability sampling; cluster sampling), the relatively small sample size, case ascertainment in the SCZ group by consultant psychiatrist diagnosis rather than the employment of a diagnostic instrument, and the inherent limitations of Likert scales. One may not be able to generalize our results to non-health service attendees; however, how non-attendees could be assessed for a diagnosis is a dilemma. It should also be noted that the level of educational attainment is disproportionately high in the ACT. Based on 2009 Australian Bureau of Statistics data [42], 34.9% of individuals aged 15–64 years in the ACT have a bachelor or post-graduate university degree compared with only 20.5% for Australia. A further potential source of systematic bias was that frequency of contact with a doctor, and what discipline that doctor worked in, were not controlled for in our analysis. Participants with schizophrenia may have had less contact with medical practitioners both within and outside mental health services. Another limitation is the possibility that in the SCZ group some of the reported health ‘information’ obtained from television, radio, Internet and the print media may have been secondary to psychotic phenomena, such as delusions of reference or auditory hallucinations or other perceptual disturbance. Validity may be questionable when asking people what they do, as in this study, rather than observing what they actually do. Furthermore, while our study invited participants to report on which information sources they were currently using, it should be borne in mind that this may not necessarily be an indication of their preference but rather reflect availability. In addition our study did not distinguish between passively acquiring health information (e.g. while reading a newspaper) versus actively seeking specific information (e.g. after noticing that a mole has changed colour) though in this initial study we were interested in both. Finally, our study also did not specify the type of heath information sought or explore the subgroups within a given information source.
Practical implications
Several practical implications arise from our study. There needs to be investigation into strategies which seek to encourage stronger and more effective links between patients with schizophrenia and a GP, for the provision of accurate health information. Furthermore, clinicians may need to adopt an assertive approach of actively enquiring about physical health issues and then providing relevant and tailored information and recommendations rather than having an expectation that physical symptoms will be disclosed spontaneously. We received positive feedback from many participants with schizophrenia expressing a strong approval of enquiries into, and attempts to find strategies to improve, their physical health. However, GP shortages could present a challenge here. Perhaps mental health services need to consider providing general medical services to their patients.
As family and friends ranked both the second most trusted and second most used health information source for people with schizophrenia, clinicians might consider encouraging and supporting them in a role of providers of health information, as is the case in many chronic neurodegenerative diseases. This might include provision of information sheets and pamphlets which they could share with the patient at a later time.
Finally, as information and communications technologies continue to gather momentum, perhaps integrated community health programmes could be developed which utilize electronic health resources but which are strongly linked to treating clinicians [28]. There may be a role here for allied health services.
Conclusion
There exist significant differences in the reported utilization and trust of health information sources between people with schizophrenia and attendees in GP settings. Given the likelihood of the Internet playing an increasing and dynamic role in health information and service delivery in the future, and the importance of accessing health advice from medically trained clinicians, further research is required to inform on strategies to mitigate this disparity. This is particularly critical in light of the high rates of comorbid physical illness and reduced longevity in people with schizophrenia.
Footnotes
Acknowledgements