
Abstract
Māori, the Indigenous people of New Zealand (NZ), experience significantly poorer mental health and higher rates of mental illness than NZ Europeans (particularly for schizophrenia and other psychotic disorders, mood disorders, substance use disorders and suicide) [1,2]. The majority of NZ psychiatrists recognize that an understanding of Māori culture is important to good psychotherapeutic outcomes for Māori clients, and believe they need training in Māori perspectives of health [3]. When patients and health professionals hold different and possibly conflicting beliefs about the patient's illness, this can result in conflict, patient non-adherence to treatment and frustration for both parties [4].
Traditional Māori beliefs about health have been described as holistic and encompass spiritual, mental, family and physical dimensions. Māori distinguish between illnesses as ‘mate tangata’, where the causes of injury are readily identifiable, and ‘mate atua’ (sickness of the gods) for which there is no obvious external cause [5]. Illnesses that are believed to be of spiritual origin or from the gods (atua) are perceived as the result of a breach of ‘tapu’ [5]. Tapu violation, deliberate or accidental, was believed to be the most frequent cause of illness [6]. Although there was believed to be a spiritual basis to mental illness, it was also closely linked with social norms [7]. Restoration of health required a ‘tohunga’ (traditional Māori healer). The tohunga traditionally diagnosed the cause of the illness and prescribed a rehabilitative process that usually involved the use of ‘karakia’ (prayer), ‘rongoa’ (remedies) and ‘utu’ (act of restitution). This process was designed to appease or remove the atua and was then followed by a ceremony to remove the tapu [7,8].
It has been proposed that rapid urbanization between 1950 and 1980 may have been a factor in the increase of psychiatric illness among Māori, involving separation from family and culture [9]. However, there has been a resurgence of Māori culture, identity and customs in the last few decades. The most popular and widely accepted contemporary Māori model of health is Durie's Te Whare Tapa Whā model [10], which compares health to the four walls of a house which represent the dimensions of mental, spiritual, physical and family health. Māori see mental illness as a result of a tapu infringement by the patient or their wider family [7], but it can also be seen as resulting from a movement away from Māori traditions and therefore a loss of connectedness to Māori spirituality. Correspondingly, healing can require a process of connecting to Māori traditions and values [8], and often Māori will accept western biomedical treatment for an illness while simultaneously seeking help from a tohunga [11].
Two qualitative studies explored the perceptions of Māori who identified as having recovered from mental illness. Both studies found recurring themes that balance (between body, person, ‘whānau‘, and the environment) and a secure personal and cultural identity were important to recovery [12,13]. The narratives of recovery between Māori and NZ Europeans contained many similar themes and processes but, Māori patients also identified Māori identity, understanding mental illness within a Māori cultural frame, whānau care, Māori healing processes and spirituality as important factors.
Developed in the 1980s, the Common Sense model of illness has been applied to understanding patients’ perceptions of illness. This social-cognitive model posits that patients form cognitive representations (illness perceptions or explanatory models) of, and have an emotional response to, their illness and that these beliefs influence how patients manage their illness [14]. Patients’ perceptions of illness have been found to cluster around five dimensions: illness identity (the name the patient gives the illness and the symptoms they associate with it), timeline (beliefs about the course and duration of the illness), consequences (the expected effects and outcomes of the illness on the patient's life), the patient's perceived cause(s) of the illness, perceived personal control over the illness and perceived treatment control [15]. Research has shown that this model, though originally developed for use with physical illness, is valid across a variety of mental illnesses including schizophrenia [16–18], and across cultures, including Māori [19,20]. Applying this model provides the advantage of a theoretical model for conducting research. Questionnaires have been developed and psychometrically validated, which allow easy assessment and comparisons to be made between individuals, groups and across time. Evidence suggests that there are cultural differences in illness perceptions among patients with diabetes or mental illness [4,21,22]. New Zealand diabetes research shows that Pacific Islanders tend to think that diabetes will last for a shorter amount of time than Europeans think, have more spiritual causal beliefs, and have lower medication-specific self-efficacy [21,22]. Causal models for mental distress have been shown to differ between ethnic groups in Britain [4]. To our knowledge, there are no published studies that have investigated differences in illness perceptions between NZ Europeans and NZ Māori using Leventhal's Common Sense model in any patient group.
This study aimed to compare illness perceptions between Māori and NZ Europeans who were diagnosed with schizophrenia or other psychotic disorder. While this is an exploratory study, the literature review suggests that Māori may have more spiritual beliefs about the cause of their illness, less strongly believe in the effectiveness of medication as a treatment, and believe that their mental illness would have a shorter duration than NZ Europeans, due to traditional beliefs about the causes of illness and the ability of healers to cure illness.
Methods
Participants
This paper reports findings concerning ethnic differences in illness perceptions from data collected for a study of illness perceptions, unmet needs and attitudes to treatment [23]. A full description of methods is reported in that paper. The study was approved by the Auckland Ethics Committee, and support was gained from each DHB Māori Review Group.
In brief, 203 high users of mental health services completed interviews with trained interviewers matched on ethnicity, and health board staff rated their functioning. The interviewers were recruited from DHB consumer networks and NGOs and selected following selection interviews and an orientation and training day. This was followed by two days of training provided by the manager of the Survey Research Unit and a psychiatric research nurse, and a follow-up phone call after three to five interviews to check whether any problems had arisen [24]. In this paper we wanted to assess perceptions of patients within a common diagnostic group, therefore we only included patients with DSM-IV diagnoses of schizophrenia, schizoaffective disorder or psychotic disorder not otherwise specified. A total of 76 patients who did not meet these criteria were excluded. A further 16 patients who identified as an ethnicity other than Māori or NZ European were also excluded from this study. In the final sample, there were 41 NZ Europeans and 65 Māori who had diagnoses of schizophrenia; two NZ Europeans and three Māori who had other psychoses.
Measures
Demographic details were collected in the larger survey. Trained clinicians completed the Global Assessment of Functioning (GAF) from the DSM-IV, for each patient on a scale from 1 to 100 where 100 represents higher functioning.
The Brief Illness Perception Questionnaire was used to assess patients’ illness perceptions [25]. This 9-item questionnaire has established validity and reliability. Patients’ perceptions of the identity of their illness (extent of their symptoms), its consequences on their life, the timeline of the illness (chronic or acute), their own ability to personally control the illness, the ability of treatment to control the illness, their perceptions of how well they understand the illness, how concerned they are about it and how it emotionally affects them, are assessed on single-item scales rated from 0 to 10. The patient's top three perceived causes for their illness are assessed using an open-ended item.
The Drug Attitude Inventory (DAI-10) was used to assess attitudes towards medications [26]. This scale consists of statements that are rated true or false, such as ‘Taking medication will prevent me from having a breakdown’.
Statistical analysis
SPSS was used for data analysis. T-tests and Mann-Whitney U tests were conducted to assess whether Māori and NZ European patients differed in terms of their functioning and attitude to medication and illness perceptions. Causal beliefs were assessed by coding patients’ responses to the causal item into categories formed from a bottom-up assessment of the data. The frequency of the responses in each category was calculated and Pearson chi-square tests were performed to analyse whether there were any differences in causal attributions between Māori and NZ Europeans.
Results
A total of 111 participants with a diagnosis of schizophrenia or other psychotic disorder identified as Māori or NZ European. The characteristics of the two ethnic groups were compared to evaluate differences in demographic variables, functioning and attitude to medication (Table 1). There were no significant differences in the ages of the two groups, gender, partner status, and status under the Mental Health Act, or comorbidity.
Characteristics of NZ Europeans and Māori with schizophrenia.
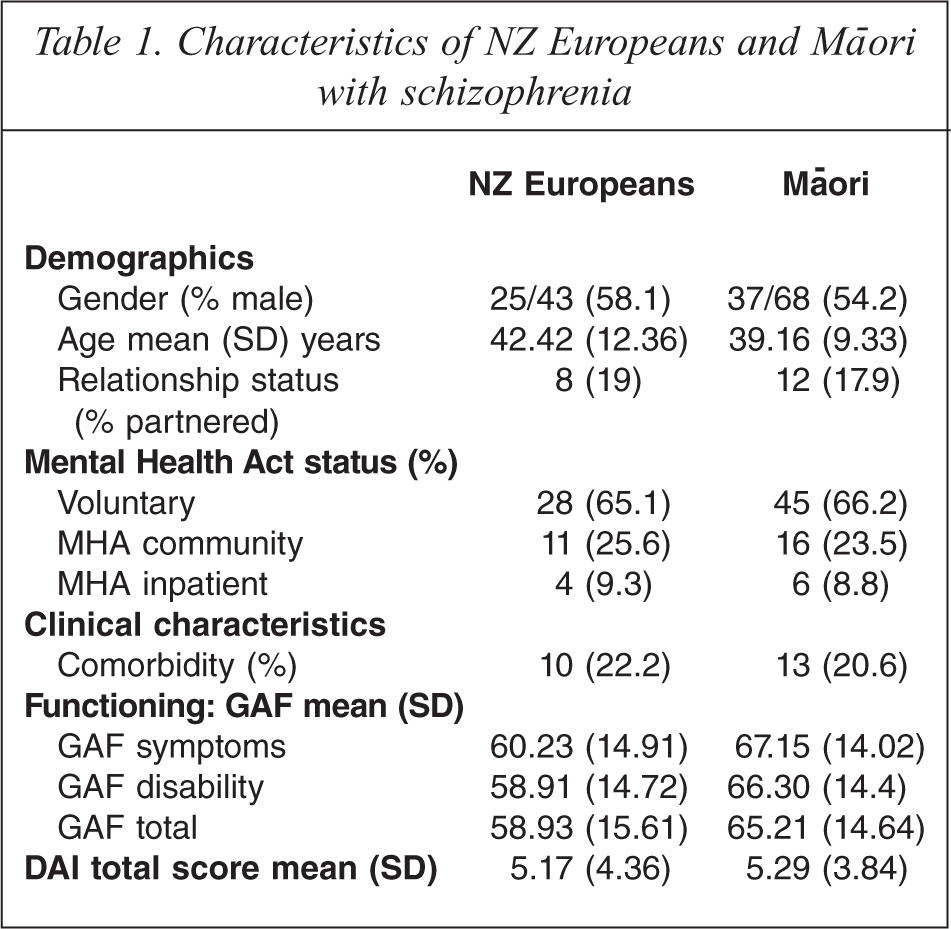
Māori experienced significantly better functioning on average, in terms of symptoms, disability and overall functioning, with t(107) = −2.46, p < 0.05, t(107) = −2.60, p < 0.05, and t(108) = −2.14, p < 0.05, respectively.
There was no significant difference between the two groups on the DAI, with both groups showing a positive attitude towards their psychiatric medication. There were no significant differences between groups on illness perceptions except on timeline, where Māori believed that their illness would continue for significantly less time than did NZ Europeans (Table 2).
Illness perception scores between NZ Europeans and Māori with schizophrenia.
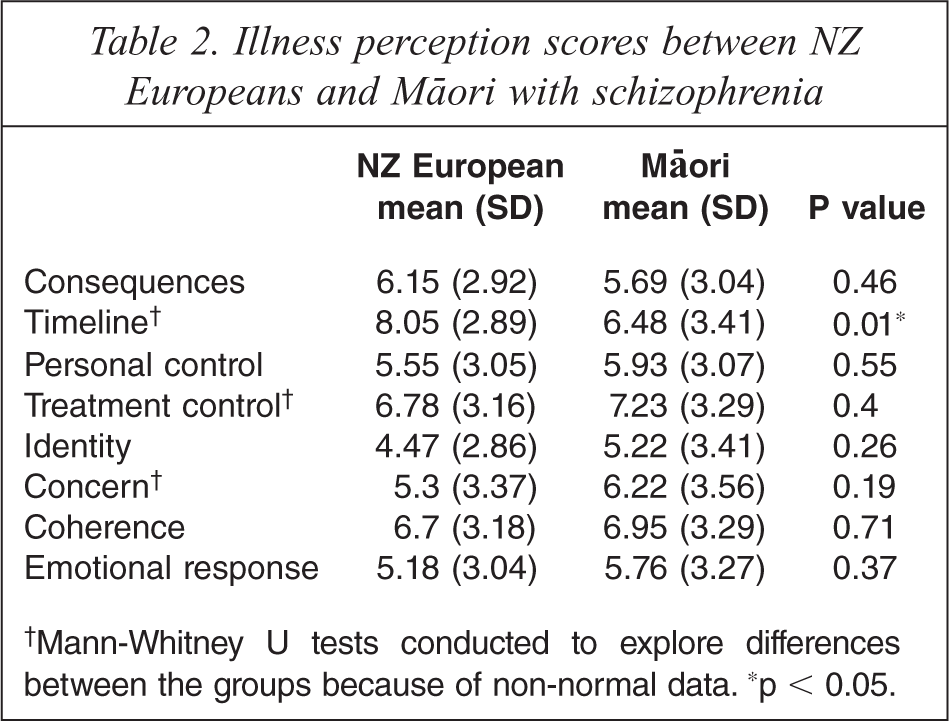
†Mann-Whitney U tests conducted to explore differences between the groups because of non-normal data. *p < 0.05.
Because of the significant differences between Māori and NZ Europeans on GAF scores, ANCOVAs were run, with GAF symptoms, disability and overall functioning as covariates. Where data was not normal, this was done with ranked scores. There was no change in the significance of the results for differences in illness perceptions and drug attitudes.
There was a relatively poor response rate to the causal question with only 49.5% (55 participants) identifying what they thought was the most important cause of their illness, and this decreased for subsequent causes. Responses were grouped into categories using a bottom-up approach in order to see which factors were most commonly endorsed as important causes of mental illness. Eight categories were derived; family relationships/abuse, biological, drugs/alcohol, behaviours, stress, psychological, chance/don't know, and spiritual (Table 3).
Perceptions of most important cause of illness amongst NZ European and Māori consumers with schizophrenia.
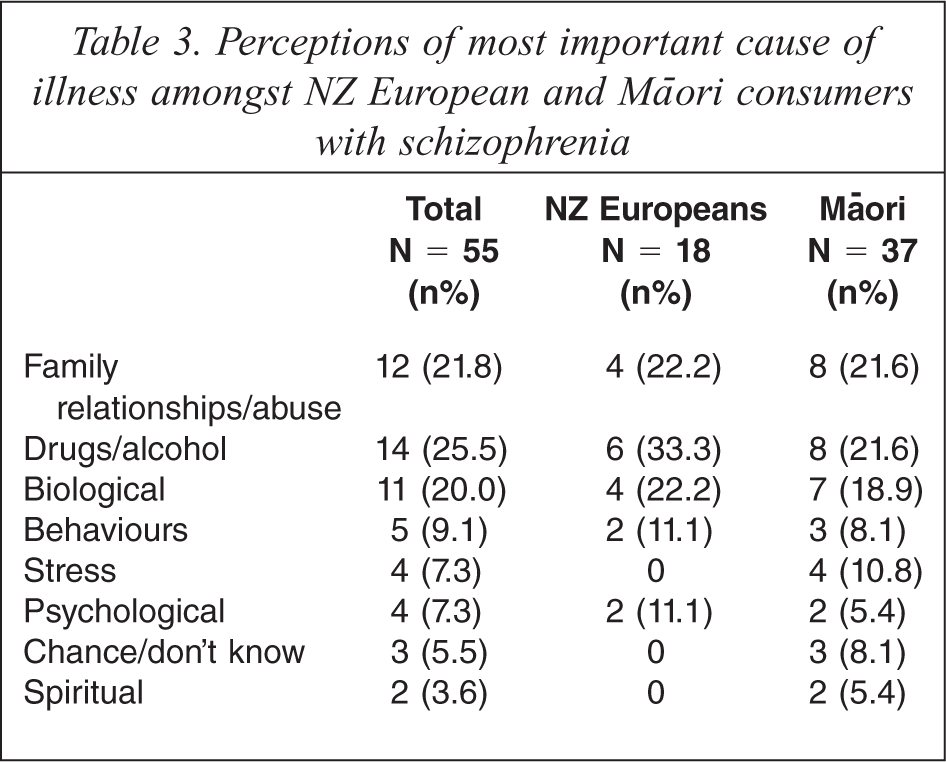
The three most frequently endorsed causes for both Māori and NZ Europeans were drugs/alcohol, family relationships/abuse and biological causes. No significant differences in causal attribution were detected between Māori and NZ Europeans. Only Māori endorsed ‘chance/don't know’ and ‘spiritual’ as the most important cause of their illness/schizophrenia, but sample sizes were too small for statistical analysis of these categories.
Discussion
NZ Māori patients with schizophrenia hold the perception that schizophrenia will last for a shorter time compared to NZ Europeans. Māori have similar attitudes about their medications, and similar perceptions concerning the identity, consequences, perceived control over their illness, understanding of their illness, concern and emotional reactions to the illness. Five Māori consumers responded with ‘chance/don't know’ or spiritual attributions for schizophrenia compared to no NZ Europeans.
These findings are similar to previous work showing that Pacific Islanders and South Asians have shorter timeline beliefs about diabetes [22]. Traditionally, Māori believed that mental illness (‘wairangi’ or ‘po-rangi‘) was due to the infringement of tapu and making amends for the offence and treatment by the tohunga would (usually) cure the illness. It is possible that this contributes to the shorter timeline belief held by Māori, although only two Māori patients explicitly reported spiritual causes for their illness.
Contrary to the hypothesis that Māori would have less positive attitudes towards medication, both groups demonstrated positive attitudes. This is a positive sign for acceptance of drug treatments. Evidence suggests that in Auckland in 2004, European and Māori patients had equal access to recommended best practice with antipsychotic treatment in schizophrenia [27]. Other work suggests that stronger therapeutic alliance is related to better attitudes towards medication in patients with schizophrenia [28].
It was surprising that there were not greater differences in other dimensions of illness perceptions. Many Māori, particularly those in cities, may have lost ties to their wider whānau and their ‘iwi’. This may mean that they do not have much knowledge of traditional Māori culture and may not hold traditional beliefs about health and illness, including mental illness. Because the sample was primarily from Auckland, a heavily urbanized area, differences between Māori and NZ Europeans may have been attenuated. Other evidence suggests Māori have higher rates of serious mental disorders and have lower health service contact for mental illness (after adjusting for severity) [29]. Contrary to this evidence, the Māori group in this study were better functioning than Europeans, suggesting they were a selected group. Future research could assess the degree of cultural immersion or how strongly Māori identify with Māori culture and traditions in order to see if this affects their illness representations.
Overall, the most common causes to which schizophrenia and psychotic illness were attributed were family relationships/abuse, biological factors, and drugs and/or alcohol. Stress was only endorsed by 7% of the sample. In comparison, Lobban and Barrowclough [30] used a causal checklist and found the most commonly endorsed causes for schizophrenia were stress/worry, trauma, chemical imbalance, mental attitude and thinking too much. Using an open-ended question allowed participants to list culturally specific causal beliefs such as Māori tapu. This suggests that an open-ended format may be more appropriate when investigating causal beliefs in cultures with traditional medicine.
The common perceived causes are consistent with current theories of mental illness, particularly psychosis. A widely accepted view of psychosis is the stress vulnerability model [31], which posits that people have an underlying vulnerability to developing psychosis and that this can be triggered by varying degrees of stress. This is supported by the fact that family relationships/abuse was the most frequently mentioned cause in the present study, as were biological factors which included genetic predisposition. Morrison [32], has suggested that traumatic experiences play a role in the development of psychotic symptoms. The results are also consistent with the theory that drug use is associated with mental illness, particularly psychotic disorders.
Māori experienced fewer symptoms, less disability and had better overall functioning than NZ Europeans. This was contrary to expectations, as previous research had found that Māori were more adversely affected by mental illness and tended to access mental health services only when in crisis or acutely unwell [1]. This may suggest that Māori consumers with a serious mental illness in the greater Auckland area are receiving high quality, culturally appropriate services from their mental health providers. However, these results may reflect a selection bias, whereby only highly functioning patients agreed to take part. Other possible explanations for these results are that Māori and Pacific teams may hold on to ‘recovered’ patients longer than other teams and/or the raters for the GAF scores (who were the clinicians responsible for the individual), may have rated differently. It is possible that, because of the patients’ traditionally poor medication adherence and history of accessing services only when in crisis, mental health services have adopted a policy of maintaining longer-term contact and providing a higher level of support to Māori consumers. In contrast, the NZ European consumers in this study may be more unwell and not have been receiving support from mental health services as long nor as intensely. However, there is no evidence to support this proposition. Other work has suggested that a lack of cultural understanding may result in clinicians mis-rating consumers [33]. Future research in this area should consider the influence and assess the length of contact with mental health services, as this may influence beliefs and behaviours.
This study has several limitations. The sample may have been biased to only include those consumers with better functioning because of self-selection to take part in the interview. It is limited by a small sample size, particularly for causal beliefs. This item was at the end of a fairly long questionnaire and had an open-ended format; it is possible that the interviewers were not trained to write ‘don't know’ when this was the participant's answer. The interviewers were themselves consumers, rather than professional researchers, and may not have had the skills to interpret difficult answers.
A strength of the present study was that the majority of the interviewers were matched for ethnicity with the participants they interviewed.
This preliminary research has shown that Māori have shorter timeline perceptions than NZ Europeans about schizophrenia. More research is needed in this area. Clinicians may ask patients about their perceptions of the likely duration of their mental illness in order to better communicate with patients using shared understandings.
Footnotes
Acknowledgements