
Abstract
Acute mental illness frequently interferes with sufferers’ capacity to be involved in decisions about their treatment and health care. Anticipatory planning tools may overcome this problem, as they allow patients to develop and document a plan for their treatment in the event of an incapacitating period of acute illness [1]. Advocates for these types of documents argue that they promote patients’ human-right for self-determination [2,3] and improve service quality and delivery [4,5]. Also, anticipatory planning tools may enhance therapeutic gains as they promote more collaborative therapeutic relationships [6–8]. More broadly, increasing awareness of anticipatory planning tools could help reduce stigma as they improve perceptions about the capacity of people with mental illness to be involved in their treatment [9].
Since the introduction of the United States Patient Self Determination Act (1990) 25 jurisdictions have legislated anticipatory planning tools as patients’ instructions to their care providers [10,11]. Similarly, in the UK the profile of advance planning in mental health has been raised following the reviews of mental health legislation in 2001 [10]. While the Australian Fourth National Mental Health Plan 2009–2014 is committed to involving consumers [12], strategies such as anticipatory planning tools are at a relatively early stage of development in Australia. Some Australian mental health services have made anticipatory planning tools and processes available to consumers but none of these documents are to date legally authorized. In addition, there is no research in the Australian context looking at anticipatory planning tools, how to optimize their benefits or identify barriers to their implementation. The current study provides local evidence about these issues by examining the processes and outcomes associated with the implementation of mental health advance agreements (AdAs) as anticipatory planning documents in the Australian Capital Territory (ACT).
The empirical findings on psychiatric anticipatory planning have been equivocal. Some studies document benefits such as fewer compulsory admissions [13] while others show no significant improvements for compulsory readmissions, voluntary readmissions or days spent in hospital [14]. Few studies provide information on person-related benefits such as sense of self-determination, sense of control regarding treatment, or alliance with clinicians. Furthermore, knowledge about how anticipatory planning tools could be effectively implemented within mental health services is very limited [15]. For example, one study reported that only between 4% and 13% of psychiatric outpatients had completed an advanced directive, despite between 66% and 77% wanting to if given assistance [11]. Swanson [16] recently found that although a 2-h facilitation session is effective in overcoming barriers to completing an advanced directive, 2 months after the session only 43% of people had finalized a directive. Importantly, these authors recommended that ‘for advanced directives to achieve their promised benefits, system level policies and interventions may be needed in order to embed facilitation of psychiatric advanced directives in usual-care settings’ [16, p.1950].
Our conclusions from this evidence is that embedding of anticipatory planning tools in mental health settings will require knowledge of patient and service factors which impact on their implementation. These considerations can be idiosyncratic and diverse, so local research [17] will be the starting point for how to best progress anticipatory planning tools. This research needs to be part of the ‘good deal of trial and error (which) is needed before workable, culturally congruent practices (supporting advanced directives) are arrived at’ [15]. The current study is an investigation into AdAs as an initiative within Mental Health ACT (MHACT). The objectives of the initiative were to trial and evaluate the implementation of AdAs and to contribute to the growing knowledge on anticipatory planning as a part of mental health services.
This study has two specific aims:
To document and evaluate the stages and processes involved in developing an AdA including obstacles to implementation, and
To provide feedback on outcomes associated with developing an AdA.
These aims are addressed through a combined quantitative and qualitative examination of the development and implementation of AdA in MHACT.
Study design
The AdA initiative introduced a method for documenting a consumer's preferences for future treatment. The initiative used an action research design that progressed through five main phases. Phase one: identifying and targeting relevant stakeholders and establishing their interest. Phase two: assembling the materials required for the initiative. This included creating and trialling an AdA guide and template, an AdA workbook designed to assist the completion of the AdA template, and an AdA manual for clinicians. Phase Three: disseminating the initiative within MHACT and consumer groups. This phase involved creating a campaign of posters, fliers, and education sessions for consumers, families and clinicians. Phase Four: implementing AdAs. This phase consisted of recruitment, further education, gaining consent, implementing the initiative materials. Phase Five: evaluating the implementation of AdAs. This was achieved by formulating two evaluation tools, AdA questionnaires semi-structured interviews conducted on completion of an AdA. The current study reports the findings from phases 4 and 5 in regard to the evaluation of process and outcomes.
Method
Recruitment and procedure
The study protocol was approved by the human ethics committees of ACT Health and the Australian National University.
Participants
Participants were mental health consumers and their key clinician. To be eligible consumers had to be over 18, have a diagnosis of a serious mental illness, be currently receiving mental health care, be able to give informed consent and have a key clinician willing to participate in developing an AdA with them. During a six-month period we disseminated information about the initiative to adult mental health teams, older person mental health team and mental health rehabilitation units.
Procedure
Both consumers and clinicians could initiate participation and nominate their respective partner. Consent was collected individually. Once consent was obtained, pre-AdA measures were administered. Consumer/clinician pairs then moved through the process of developing an AdA as shown in Figure 1. Workshops and workbooks were provided to assist in the process and in listing preferences for future treatment in an acute episode. Participants were able to collaborate and develop the AdA in a way that they considered meaningful. At the completion of the AdA a semi-structured evaluation interview and self-report outcome measure was administered to each participant.
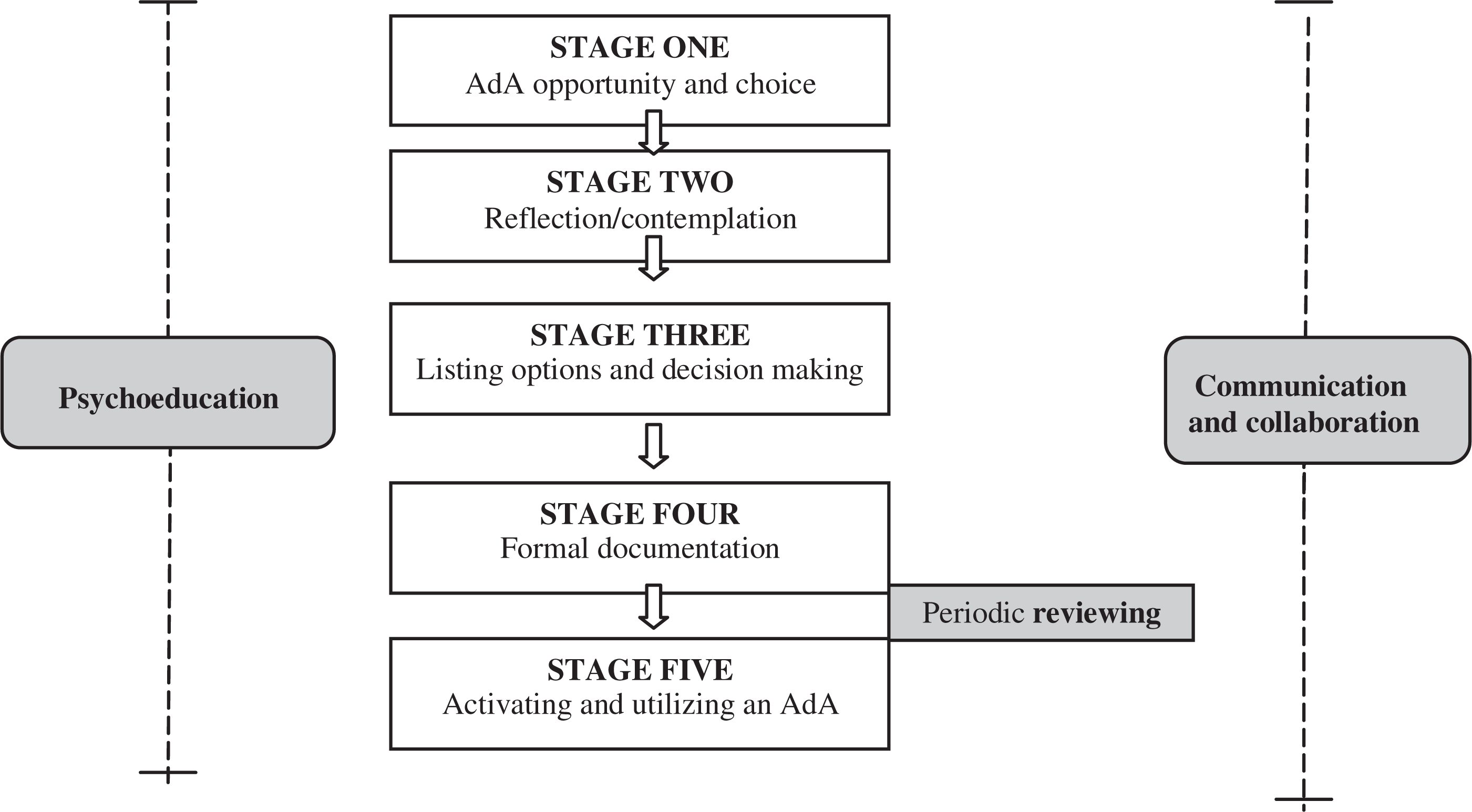
The five stages of developing and activating an advance agreement.
Measures
Demographics information
Relevant demographic and clinical information was obtained with patient consent from the MHACT database.
Beliefs and experiences of managing mental illness
We developed two questionnaires. The Consumer Pre-AdA questionnaire asked consumers about their ability to manage their mental illness and about useful aspects of treatment and care. The Clinician Pre-AdA questionnaire assessed clinicians’ prior experience with anticipatory planning documents, their beliefs about AdAs, and their estimate of the consumer's current management of his or her mental illness.
Outcomes. Individual semi-structured interviews
A semi-structured interview was constructed to gain feedback from participants who completed an AdA. By using a semi-structured interview the same topics could be addressed consistently across participants, allowing for individual elaboration and further explanation. The interview questions were open-ended and assembled around the aims and goals of the initiative. The interviews were conducted following completion of an AdA. A single researcher (B.W.) administered all of the semi-structured feedback interviews which lasted for approximately 30 to 50 min.
Content analysis
The semi-structured interviews were audiotaped and transcribed. A proportion of the transcripts were reviewed to ensure accurate transcription. Content analysis [18] was used to paraphrase and reduce the text to condensed records while preserving the essential contents. The condensed data was then used to develop structured protocols and a dimensional system. For example, ‘previous negative experiences with hospitalization’ may be assigned to a dimension titled ‘motivation to develop an AdA’. These dimensions included positive and negative motivations to develop and AdA, the quality and quantity of contribution for each member of the pair, the degree the AdA represents true preferences and perceived impact or outcomes of the process.
Self-rated outcomes
We also designed a self-report of the impact of the AdA process on the consumer's sense of independence, control, motivation, and confidence towards managing mental illness (less, no change, more, or unsure).
Analysis
All responses were anonymised (consumer, clinician). The data were analysed primarily to evaluate the process of developing an AdA, associated outcomes and to identify barriers. The analysis adopted primarily a descriptive approach. As well as reporting the quantitative findings we emphasise the individual experiences of consumer and clinician in various topics within the dimensions.
Results
Enrolment and sample characteristics
Figure 2 documents the recruitment and flow of participants through the research. Of the 33 consumers who consented to take part, 64% (n = 21) began the process of documenting an AdA. Of those who did not begin the document most, 67% (n = 8), could not be contacted after initial consent, 2 changed their minds about taking part and 2 did not feel the process was appropriate (1 consumer; 1 clinician). Of those who began, 64% (n = 14) completed an AdA. Reasons for not completing an AdA included discharge from clinical management (n = 2), relocation out of the ACT (n = 2) and relapse of illness (n = 2). One consumer found the process too confronting and requested not to continue. All consumers who completed on AdA had a history of both hospitalization and case management. Their primary diagnoses were schizophrenia (n = 8), major depressive disorder (n = 3), bipolar affective disorder (n = 2) and borderline personality disorder (n = 1). Seven of these had no hospitalizations during the 12 months prior to engagement with the project, four had one hospitalization and two consumers reported two hospitalizations during that time. Of those consumers, participation was initiated equally by clinical managers and consumers.
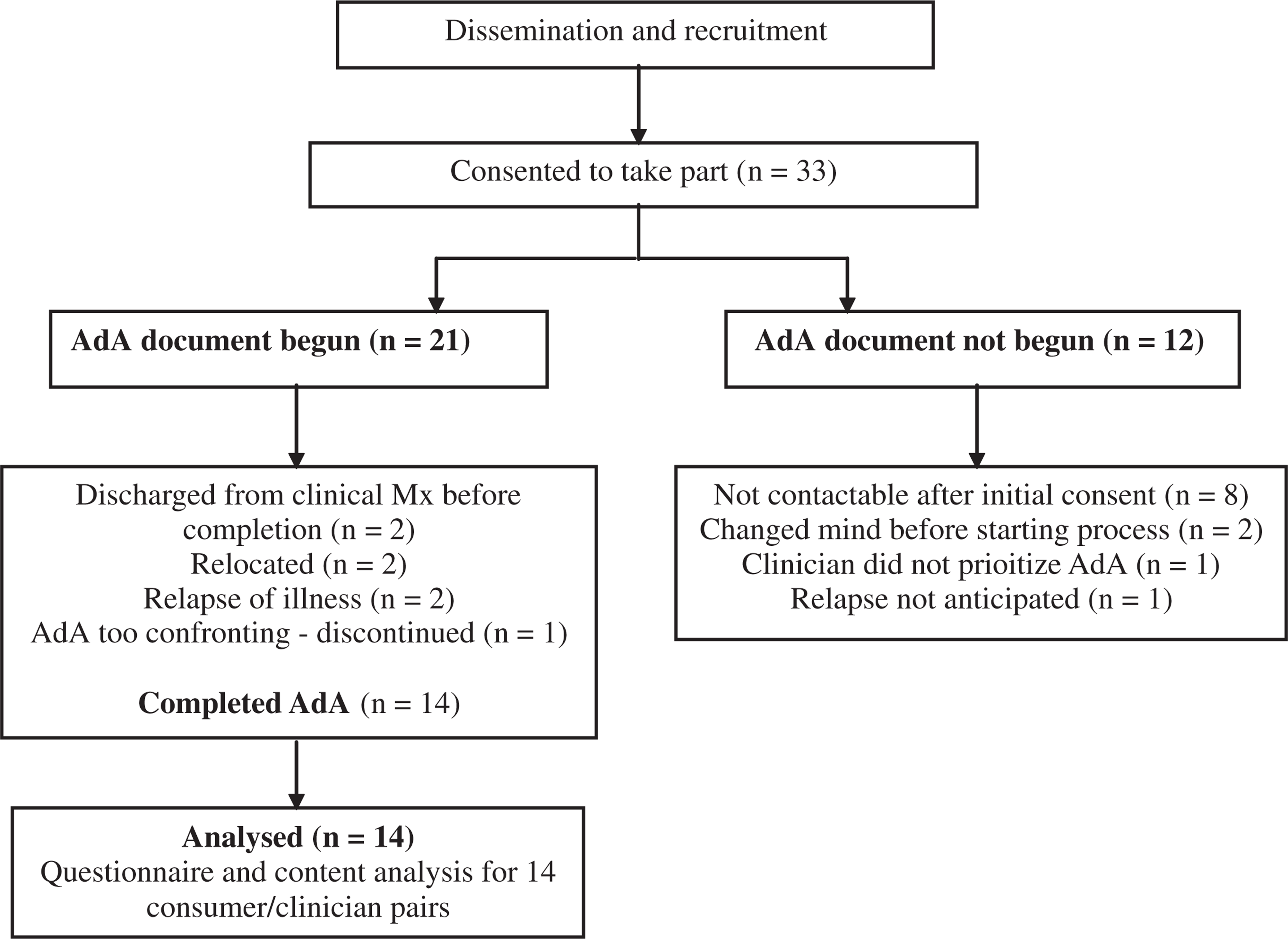
Enrolment and outcome for AdA dissemination strategy.
Beliefs and experiences
Half of consumers (n = 7) reported that during their last hospitalization they were not involved in their treatment. Half reported that over the past year they found psycho-education and medication to be the most helpful aspects of managing mental illness. Of the consumers 57% (n = 8) reported feeling extremely or completely motivated towards managing their mental illness. None of the clinicians reported having experiences with anticipatory planning tools.
Semi-structured interview
Process evaluation
Motivations for developing an AdA. Consumers believed developing an AdA was important in order to communicate self involvement, enhance communication with mental health professionals, and improve outcomes for treatment and care. More specifically, consumers connected ‘involvement’ to: providing consent, reflecting on past experiences, gaining control, and demonstrating they have knowledge, experience, and acceptance of their mental illness. For many consumers, previous negative experiences with hospitalizations and medications were also motivations. Many clinicians reported that ascertaining a consumer's preferences was part of routine practice, although not in the way of the formal agreement. Clinician reasons for developing an AdA were to use it as a therapeutic tool, as a way of including other potential support when needed, and to facilitate treatment during an acute episode.
Contemplation. Some consumers put a significant amount of effort into contemplating issues related to their mental illness and past treatments, while others stated that they already knew their preferences. Reflecting on one's own mental illness was often reported to be a challenging aspect of developing an AdA, although spending more time on contemplating issues around their mental illness resulted in more detailed AdA.
Deciding on preferences and documenting them. Completing an AdA ranged from 30 min (one session) to 15 h over several sessions. Clinicians commented that completion time was impacted by case loads, how well the consumer was, and the amount of documentation. Most participants recognized the process was dependent on the consumer, who should complete the AdA ‘in their own time and their own way’. Many consumers knew their preferences or flowed through the steps of decision making automatically. For some, the steps of problem solving outlined in the workbooks was time-consuming and repetitive. For the preferences that did require some problem solving, researching information, deciding on actual preferences, and making complete plans were reported as difficult.
The completed document. All the consumers reported the AdA documented their true preferences with some minor limitations. All clinicians indicated that they believed the AdA adequately represented the consumer's true preferences. Clinicians described several barriers to gaining a consumer's ‘true’ preference. Firstly, the options on offer and the consumer wishes can conflict. For instance, a consumer may prefer clinically unviable options. Secondly, due to mental illness or personality, some consumers frequently and rapidly change their mind. Thirdly, it was recognized that some consumers are not assertive or effective at verbalizing their views.
Education and collaboration. All participants reported possessing enough knowledge to complete their AdA. Eight consumers reported that they had more input into developing the AdA compared to their clinician. Five consumers stated they had equal input and one stated they had less input compared to their clinician. All clinicians and thirteen out of 14 consumers reported satisfaction with their partners input. The consumer reporting dissatisfaction with clinician involvement attributed this to realizing they could be treated for mental illness regardless of the AdA. Clinicians reported that points of disagreement were resolved through open discussion, giving the consumer space, gently challenging and acknowledging differences of opinion. Consumers identified several roles for clinicians such as organizing the process, scribing, helping the consumer to articulate preferences, sharing knowledge, encouraging the notion that treatment is required for mental health, facilitating decision making, and reducing distress when discussing issues that may arise. While over half of the consumers included their significant others in their AdA, only four consumers reported that the inclusion entailed direct involvement or collaboration.
Outcomes
Self-rated changes
Table 1 outlines results of self-rated outcomes for independence, control, motivation, and confidence towards managing mental illness.
Frequency of post-AdA ratings of change in psychological factors related to management of mental illness
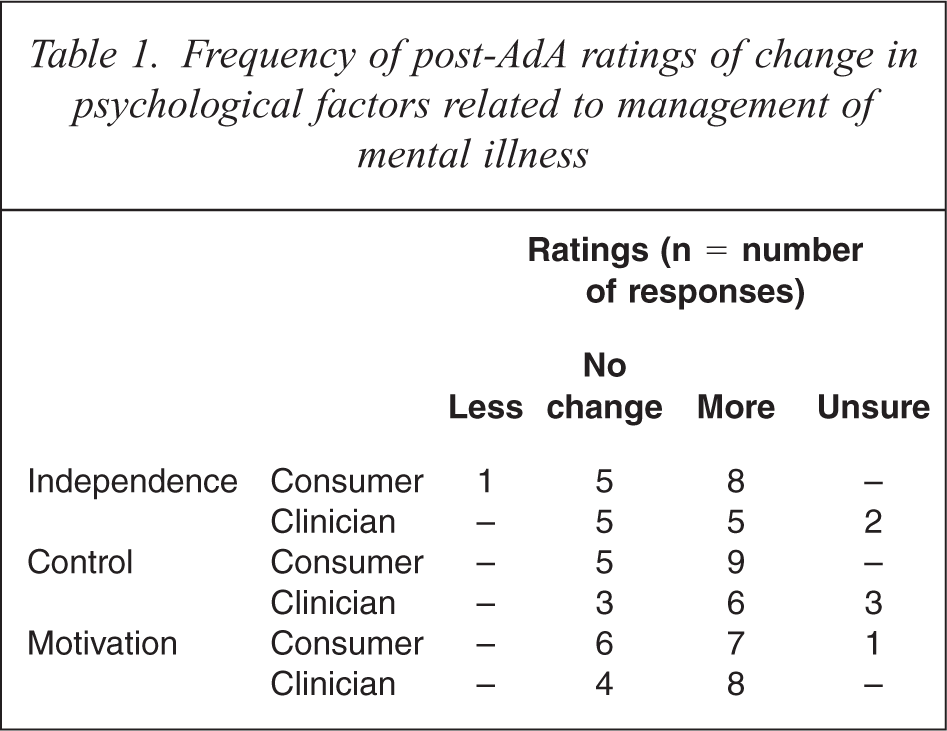
Consumers who rated themselves as more independent attributed this to feeling independent around future periods of illness and increased knowledge of options. All consumers who reported no change had rated their sense of independence as moderate or above pre-AdA. One consumer reported feeling less independent because they realized how much power mental health professionals have over hospital admissions. Clinicians identified that independence was enhanced by giving a consumer time to discuss their mental illness, and encouraging ownership of choices. The consumer's enhanced sense of control was mostly related to control over medication options. All five consumers who reported no change in their level of control in managing their mental illness had pre-AdA ratings of feeling in control ‘half of the time’ or more. Half the consumers stated they felt more motivated to seek help and support if they noticed early warning signs. Clinicians identified consumers as more motivated to adhere to a treatment plan, attributing this to psycho-education, a greater acceptance of mental illness, and acknowledgment of the benefits of treatment.
Semi-structured interview
Perceived outcomes: benefits
The identified benefits described in the interviews clustered into three groups: consumer benefits, interpersonal benefits, and professional or system benefits. For the consumers, perceived benefits include improved sense of self-determination and knowledge of their illness and of treatment options. Perceived interpersonal benefits included enhancement of the therapeutic relationship, improved clinician empathy and identifying support. At the service level, perceived benefits include clarification of roles and responsibilities, improved integration of care and improvement in attitudes towards consumer self-determination. There were also community level benefits noted. One consumer, for example, reported that AdA may aid understanding of mental illness in the broader community.
Perceived outcomes: barriers
Three broad themes about barriers to AdAs became apparent throughout the interviews. These were limited treatment options available, mental health legislation, and consumer previous experiences with the mental health system.
Many participants remarked on the limited options for future treatment and the difficulty accessing services. For example, regarding hospitalization, one consumer commented ‘I don't have private health cover so it's really, I don't think it's a choice for me where I go’. Discussion about treatment options revolved around case management. Participants commented on the long waiting lists, heavy case loads, difficulty accessing and receiving case management, and staff changing roles or absences. Current clinical management was viewed to be ‘crisis’ driven, available predominantly for consumers who are acutely unwell, and addressing immediate issues as opposed to underlying psychological problems. Consequently, it was pointed out that if a consumer is clinically managed, they are assumed to be fairly unwell, and may not be viewed as at a suitable stage for an AdA.
Many participants questioned how much control the consumer actually holds, referring to the current legislation and its ability to override consumer preferences during an acute episode. Linked to this issue was the belief that voluntary treatment is not really voluntary and that the AdA will only be beneficial if it is activated.
Several participants noted that overriding an AdA can be detrimental, as providing consumers with a service that enhances autonomy, control and power can be confusing, overwhelming, and ironic given the mental health system ultimately has the decision-making power during a crisis. Some clinicians commented that they had to remind the consumer of the duty of care the mental health service has in caring for individuals experiencing mental illness.
The third common theme was the impact previous negative experiences had on consumers’ attitudes and beliefs towards AdAs. Many consumers expressed some cynicism, reflecting a sense of hopelessness amongst participants regarding being listened to, having choice, control and power over decisions relating to their individual care. It was emphasized that memories of previous experiences of illness may be traumatic or distorted and therefore could influence a consumer's desire to participate in preparing an AdA. For instance, a consumer may feel suspicious and consider the AdA as a ‘trick’.
While these issues were considered serious obstacles the participants also suggested solutions. These included highlighting the time to build trust in developing an AdA and stressing integrating AdAs with therapy, developing strategies to increase staff awareness, introducing mandatory staff education, debriefing significant others after a crisis, and reviewing how the consumer's AdA was utilized. The participants also suggested that independently overseeing the quality of AdAs and making the offering of an AdA a mandatory practice could reduce the sense of coercion and improve the cooperation of clinicians.
Discussion
In this study we examined the implementation of advanced agreements as an anticipatory planning tool for mental health patients in a community setting. We disseminated an information strategy and provided education, materials and support to assist consumers and clinicians in completing individual advanced agreements. We assessed the process and outcomes related to the initiative with intensive interviews and self-report questionnaires.
We found that most consumers who consented to take part engaged in the process of developing an AdA with the main reasons for discontinuing being unrelated to the AdA. Illness relapses, relocations, loss to follow up and discharge from clinical management were the main factors accounting for non completion, with few consumers discontinuing for reasons related to the AdA process. For ethical reasons and because it reflects what might happen in practice, we relied on clinicians to inform the consumer about the availability of AdAs. We found, however, only 12 clinicians willing to take part in the study and feedback suggested that besides work-load, the belief that AdAs should be ‘consumer driven, staff collaborative’ was the main reason for low engagement by clinicians. Taken together, these results suggest that the development and embedding of anticipatory planning tools in mental health will require measures to ensure clinicians better appreciate their critical role in providing mental health consumers with anticipatory planning options.
Some of our results about the processes of developing an AdA suggest that clinicians may engage in anticipatory planning when they value the process as a therapeutic window of opportunity. Many consumers described that reflecting on the episodic nature of their illness, previous acute episodes and treatment during these episodes was challenging and sometimes distressing. Our results show that developing an AdA with consumers can provide clinicians with an opportunity to counsel them on sensitive topics, such as perceptions of their illness and negative aspects of previous treatment. Many participating clinicians recognized the therapeutic value of AdA and also that using them in this way may enhance the quality of the finished document.
While we did not evaluate the degree to which the finished AdAs were consistent with standards of practice, the overwhelming majority of consumers and clinicians reported that their AdA reflected well the patient's preferences for treatment within the limits of available, clinically suitable options. In addition, the participants reported that the process was collaborative, positive and satisfying. Our study indicates that when provided with opportunity and support mental health patients have the capacity to be active agents in their own treatment and care [19]. The results are consistent with those of other studies [16] which show that patients and clinicians can work collaboratively to produce anticipatory treatment requests which are feasible, appropriate and consistent with good care and acceptable to patient and clinician. Some clinicians expressed concern about the paucity of direct inclusion of significant other involvement in the AdA document. This may reflect population characteristics of our sample and suggest that standards for the content of anticipatory planning tools will vary according to the nature of the patient's illness.
The current findings show that although the benefits gained from AdAs was highly individual, these benefits parallel those anticipated in the literature [2–4]. Person-related benefits included increased sense of control and involvement in managing their illness together with better insight into their illness. Interpersonal benefits included improved rapport and clinician empathy, and better recognition of supports available. We also identified service level benefits such as better information gathering and clearer demarcation of roles, but overwhelmingly discussion of system level issues focused on impediments to implementing anticipatory planning tools in mental health. For our participants the key issues here were the limited clinical options available for preferred care in acute settings and the impotence of AdAs as they carry no legal weight. These concerns are consistent with other commentators [1,10] who describe how the perceived dishonouring of anticipatory agreements can damage patients’ sense of efficacy, their relationships with clinicians, and their confidence in the mental health system.
These problems are major challenges for mental health services and policy makers in their attempts to introduce anticipatory planning tools in a meaningful way. The amount of legal weight anticipatory planning documents should possess is a complex issue. Our results suggest that there may be benefits in the short term if mental health services ensure that consumer's expectations around the legal status of anticipatory planning are clear and that staff are provided with good faith immunity against perceived legal liability. In the medium term it would be helpful for Australian states and territories to work towards specific recommendations for mental health patients within existing guidelines about the legal status of the health care advance directive [20].
The project assisted the patients and clinicians with education, workbooks and materials. Generally, participants found the amount of support adequate. It is likely that initial embedding of anticipatory planning tools in a mental health service will require similar levels of staff and patient education and material support. We acknowledge, nevertheless, that the provision of anticipatory planning documents to all patients will only be sustained if more streamlined and efficient methods of support are developed. Other researchers [16] have shown that methods such as brief facilitation sessions are efficient in increasing rates of completion of good quality anticipatory planning documents. Given the beliefs of clinicians in our study, staff education about anticipatory planning will also be important in sustaining such documents in mental health.
The biggest limitations of the current study were the relatively small sample of patients and particularly clinicians who took part. Retention of participants in the study was challenging because many mental health consumers have transient lifestyles and because of the pressure on clinicians to discharge consumers from clinical management. In addition, the work load pressures on clinicians and the prevalent belief of many clinicians that AdAs should be patient initiated were obstacles to recruitment. The study may have been strengthened by standardized measures of process and specific outcomes which would have enable more quantitative analysis of outcomes. Nevertheless, the adoption of the qualitative methods for the project was considered appropriate at this stage of development of AdAs with more in-depth analysis of responses compensating for the small numbers of participants. Clearly, the implementation of anticipatory planning tools in mental health services needs to include ongoing evaluation of the both the immediate and longer term outcomes such as reduced rates of involuntary hospitalizations and improved patient functioning.
This study is the first to examine and document the process and outcomes of the implementation of anticipatory planning tools in an Australian community mental health setting. Overall, its findings provide support for the benefits associated with the individualized and collaborative process of developing anticipatory planning tools in mental health. While they may not be appropriate or desirable for all, the study's findings lend support to the value of anticipatory planning tools for many mental health patients. The study also identified an array of issues at the consumer, clinician and service level which services will have to overcome to facilitate consumer involvement. Our experiences suggest that the embedding of anticipatory planning tools as part of routine mental health service delivery will require significant resources, time, practice and persistence. Despite these challenges the study's findings encourage this persistence and offer an initial model of how to incorporate meaningful anticipatory planning into community mental health services.
Footnotes
Acknowledgements
We would like to acknowledge the many consumers, families, and mental health professionals who volunteered for or gave support to the project.