
Abstract
Families provide a primary source of care for many people with a mental illness [1,2] and, since deinstitutionalization and the shift of psychiatric care to the community, the role of families caring for people with a mental illness has grown considerably [3]. Many people with a mental illness receive substantial help from family in managing the symptoms, functional impairment and treatment associated with their illness [4]. Most families providing such care face ongoing challenges. They may assume new roles, such as advocacy, crisis management, and assistance with activities of daily living, and may have to cope with altered family expectations, financial demands, and changed social networks [5]. Many families care for their relative with limited resources, little information about the aetiology of mental illnesses, and no training in symptom management [6]. Moreover, families frequently report feeling isolated from usual sources of social and emotional support and ignored by the mental health system [7,8]. Potential negative consequences of providing care to a relative with a mental illness on the carer's psychological well-being include persistent worrying, feelings of loss, perceived tension between the carer and their relative [9], and psychological distress [10], here defined as negative emotional and psychological outcomes including symptoms of stress, anxiety and depression.
For more than two decades, family education programmes have been provided by carer organizations in Australia (e.g. Schizophrenia Fellowship Victoria's 14 Principles Programme [11], the Foundations Programme by Carers NSW, based on the Carer Life Course Framework [12], and the Coping with Mental Illness programme by ARAFMI Brisbane [13]), and elsewhere (e.g. National Alliance on Mental Illness (NAMI)'s Family-to-Family programme [14]) in order to assist family carers in their role and ultimately to reduce the negative care-giving consequences outlined above. Family education programmes are usually delivered in groups facilitated by trained volunteer carers and tend to be brief (12 sessions or fewer). They typically provide education about mental illnesses, help carers develop effective coping and communication skills, and encourage support between group members.
Although family education programmes share some similarities with clinician-delivered family psycho-education programmes (e.g. multiple-family groups [15]), in particular, education about mental illness and treatments, and skills training in communication and problem solving, they form a distinct type of intervention, whereas the primary focus of family education programmes is carers’ well-being, clinician-delivered family psycho-education programmes ultimately aim to improve clinical outcomes for the carers’ ill relatives, with a focus on relapse prevention [6]. Further, despite considerable empirical evidence to support their efficacy [16], clinician-delivered family psycho-education programmes have had poor rates of dissemination in mental health services and specific training initiatives have had modest uptake by staff and services [17–19]. Family education programmes facilitated by carers provide a complementary service that can engage participants in ways of understanding mental illness and coping with practical issues through the authenticity that comes from the lived experience of its facilitators. Because they are overseen by carer organizations they bypass some of the dissemination barriers faced by evidence-based family psychoeducation interventions. For example, family education programmes do not require carers’ relatives to be receiving clinical services, nor are relatives required to attend, so the attitude of the consumer is not a barrier to accessing the programme. Hence it could be argued that carer-facilitated family education programmes tend to be more accessible than professional-led psycho-education interventions.
Despite the growth and popularity of family education programmes [14], little empirical research has evaluated their efficacy. To date, three groups of researchers have conducted controlled evaluations of family education programmes in the USA [14,20] and China [21]. Results from these studies demonstrated support for the efficacy of the programmes in reducing subjective burden and depressive symptoms, and in improving empowerment and relationships within the family.
Although the efficacy of family education programmes has been demonstrated in the above-mentioned studies, the evidence base remains small. Further, no evaluations of Australian family education programmes have yet been published. It is important to examine whether such programmes are effective within Australia, given differences in culture, the mental health system, and the programmes available. Here we report an evaluation of Well Ways [22], a family education programme developed by the Mental Illness Fellowship Victoria and delivered across Australia through the Mental Illness Fellowship Australia by each state and territory's member organization. Given its extensive development over 8 years and its current dissemination through the Department of Health and Ageing to more than 2800 carers over 6 states and territories, such an evaluation is particularly timely. In this study we examined the effectiveness of Well Ways in reducing negative care-giving consequences. We also investigated whether the programme was more effective for some types of participants than for others (according to sex, relationship to the person with a mental illness, diagnosis of the person with a mental illness, and length of illness), since this may indicate a need for specialized programmes for different subgroups of carers. Secondary analyses explored maintenance of gains over time; a single-item question regarding participants’ ability to cope with their relative's mental health problems; and amount of contact with the relative as a predictor of outcomes. Our principal hypothesis was that participants’ negative care-giving consequences would be significantly lower following completion of the 8-session Well Ways course.
Materials and methods
Study design
The study evaluates the major phase of the Well Ways programme, which comprises eight 3-hour, weekly group sessions. We used an uncontrolled pre-post study design with four assessment time-points: pre-Well Ways (Time 1), post-Well Ways (Time 2), 3 month follow up (Time 3), and 6 month follow up (Time 4).
Participants
The principal outcome measure was completed by 812 participants at Time 1. A record of carers invited to participate was not kept so the response rate could not be calculated; anecdotally, however, programme facilitators reported high rates of participation. Of the 812 participants who completed the questionnaire at Time 1, 459 participants completed it again at Time 2. The sample therefore comprised 459 participants (57% of the Time 1 sample; 78% females, mean age = 55 years). The sample was drawn from 135 separate groups conducted by Mental Illness Fellowship Victoria, Mental Illness Fellowship ACT, Mental Illness Fellowship WA, Schizophrenia Fellowship Queensland, Schizophrenia Fellowship NSW, Mental Illness Fellowship SA, and Mental Health Carers NT.
An additional item about the diagnoses of participants’ relatives was completed by a subset of the sample (n = 156) who responded to a separate follow up survey (results for which are not presented here) administered to the 459 participants. Data from this item are included here to allow analysis of outcomes by subgroups according to relative's diagnosis.
Intervention
Well Ways is a group-based support and education programme for families and friends of people with a mental illness. The programme was modelled on the American National Alliance for the Mentally Ill (NAMI)'s Family-to-Family Education Programme, formerly Journey of Hope [23], and was developed for the Australian cultural and mental health context by the Mental Illness Fellowship Victoria. It is conducted throughout Australia by member organizations of the Mental Illness Fellowship Australia. Well Ways aims to assist carers through education about mental illnesses and mental health services, as well as supporting them to develop effective strategies for caring for their relatives with a mental illness and themselves. In so doing, the programme also aims to alleviate negative care-giving consequences such as worrying about the person with a mental illness and tension within the relationship, and to improve carers’ psychological well-being. The only programme entry criterion is having a family member, partner or friend with a mental illness.
Well Ways is a twelve-month programme comprising three phases. The first is the engagement phase in which potential participants make contact and are assessed for suitability for entry into the programme. The second, major phase comprises eight, 3-hour, weekly group sessions of education and discussion. The data presented in this paper reflect participation in this 8-week course. The third phase aims to consolidate participants’ social networks and skills by encouraging groups to continue social contact and to become members of the Mental Illness Fellowship; sites may also offer four optional follow-up sessions.
Groups comprise 8–14 carers; carers’ relatives with a mental illness do not attend. The facilitators all have first-hand experience in caring for a person with a mental illness. Facilitators receive training, competency testing and accreditation in delivery of the programme. The programme is based on a biopsychosocial theoretical framework that incorporates the stress-vulnerability model and includes fact sheets for participants covering current information on mental illness, its symptoms, causes and treatment. It is also informed by the facilitators’ lived experience of caring for someone with a mental illness.
Well Ways participants are provided practical information about a range of mental illnesses, and about the treatment and support options provided by mental health and carer services. Facilitators present practical insights into the behaviours a person with a given mental illness might exhibit and discuss the complexities and challenges associated with caring for a person with a mental illness. Over the course of the programme, carers are taught new ways of communicating and solving problems, are provided opportunities to share experiences, and encouraged to develop ongoing support and information networks.
Principal outcome measure
The Involvement Evaluation Questionnaire (IEQ) [24] is a measure of the negative consequences of providing care to a relative with a mental illness. The full IEQ package contains 81 items; we examined only the 27 core items, the 12-item General Health Questionnaire (GHQ-12) [25], amount of contact with the ill relative, demographic items, and a single-item variable measuring how often participants felt able to cope with their relative's mental health problems. The 27 core items formed the following four subscales of the IEQ: 1) Worrying: the carer's concerns or worries about their relative or friend; 2) Tension: strained interpersonal relations between the carer and the person with a mental illness; 3) Supervision: the carer's efforts to oversee the actions of their relative or friend; and 4) Urging: the carer's attempts to motivate their relative or friend. Items were scored on a 4-point Likert scale in which higher scores on each subscale indicated greater severity. An IEQ sumscore was also computed from the addition of the 27 core items. The IEQ is an internationally standardized measure and has undergone extensive reliability and validity testing [24]. In the current study, the four subscales and sumscore had good internal consistency at both Time 1 and Time 2; Cronbach's α ranged from 0.7 to 0.92.
The GHQ-12 is a well established measure of psychological distress. The standard scoring method was used here, by which each item was dichotomized to 0 (better than usual, same as usual) or 1 (worse than usual, much worse than usual), yielding a single severity rating from 0–12, in which a score of ≥3 indicates psychiatric ‘caseness’ [25]. In the current study, Cronbach's α was 0.92 at Time 1 and 0.91 at Time 2.
Additional item: relative's diagnoses
Information about the diagnoses of the participants’ relative was collected as part of a smaller follow up survey (n = 156), and is included here to allow analysis of outcomes by subgroups according to disorder type (dichotomized into psychotic and non-psychotic disorders).
Procedure
All carers who undertook the Well Ways programme between 2003 and 2007 were invited to participate in the evaluation project by Mental Illness Fellowship personnel during enrolment into the programme. Carers were informed of the details of the project and given a Participant Information and Consent Form. Following written consent, participants then completed the IEQ prior to the first session of the programme (Time 1). Following completion of the 8-week programme, a second IEQ was sent by mail to participants (Time 2). Participants returned completed Time 2 questionnaires in a reply-paid envelope to the Mental Illness Fellowship. The IEQ was also sent to participants 3 months (Time 3) and 6 months (Time 4) following completion of the programme; because response rates were low, data at Time 3 and 4 are considered only in a secondary analysis in order to explore maintenance over time.
Statistical analysis
In order to examine whether negative care-giving consequences were significantly reduced following participation in the 8-week Well Ways course, we analysed each subscale of the IEQ and the GHQ-12 using a mixed between-within subjects analysis of variance (ANOVA). The within-subjects factor in each analysis was time (Time 1 and Time 2). To investigate whether the programme was more effective for some types of participants than for others we included the following between-subjects variables in each ANOVA: sex (female and male), relationship to person with a mental illness (mothers and other relationships), and relative's diagnosis (psychotic and non-psychotic disorders).
Secondary analyses explored maintenance of gains at 3 and 6 month follow up using one-way repeated-measures ANOVAs for each of the four subscales. These were not included within the primary analyses due to the smaller response rates at Times 3 and 4, which would have unnecessarily limited the study sample size (see secondary analyses for details). We used a repeated-measures t-test to analyse responses to a single-item question regarding participants’ ability to cope with their relative's mental health problems at Time 1 and Time 2, then explored maintenance of gains at 3 and 6 month follow up using a one-way repeated measures ANOVA. We also analysed the amount of contact that participants had with their ill relative (using both number of hours of contact and whether they resided with their relative) as predictors of IEQ outcomes using mixed between-within ANOVAs.
Distributions of scores for tension, supervision, urging, sumscore, and distress were significantly positively skewed; square root transformations were used to render these distributions normal for analysis.
Results
Preliminary results
Participant demographics are presented in Table 1. We examined demographic differences between participants who did and did not complete the questionnaire at Time 2. Results showed a significantly smaller proportion of females, χ2 (1, n = 797) = 4.7, p < 0.05; greater length of relative's or friend's illness, z = −2.72, p < 0.05; and younger mean age of relative/friend with a mental illness, z = −2.61, p < 0.05, amongst participants who completed the questionnaire at both Time 1 and Time 2 than amongst those excluded from analysis (i.e. those who completed only Time 1). However, effect sizes for these differences were small and considered to be of no practical importance.
Demographics (N = 459)
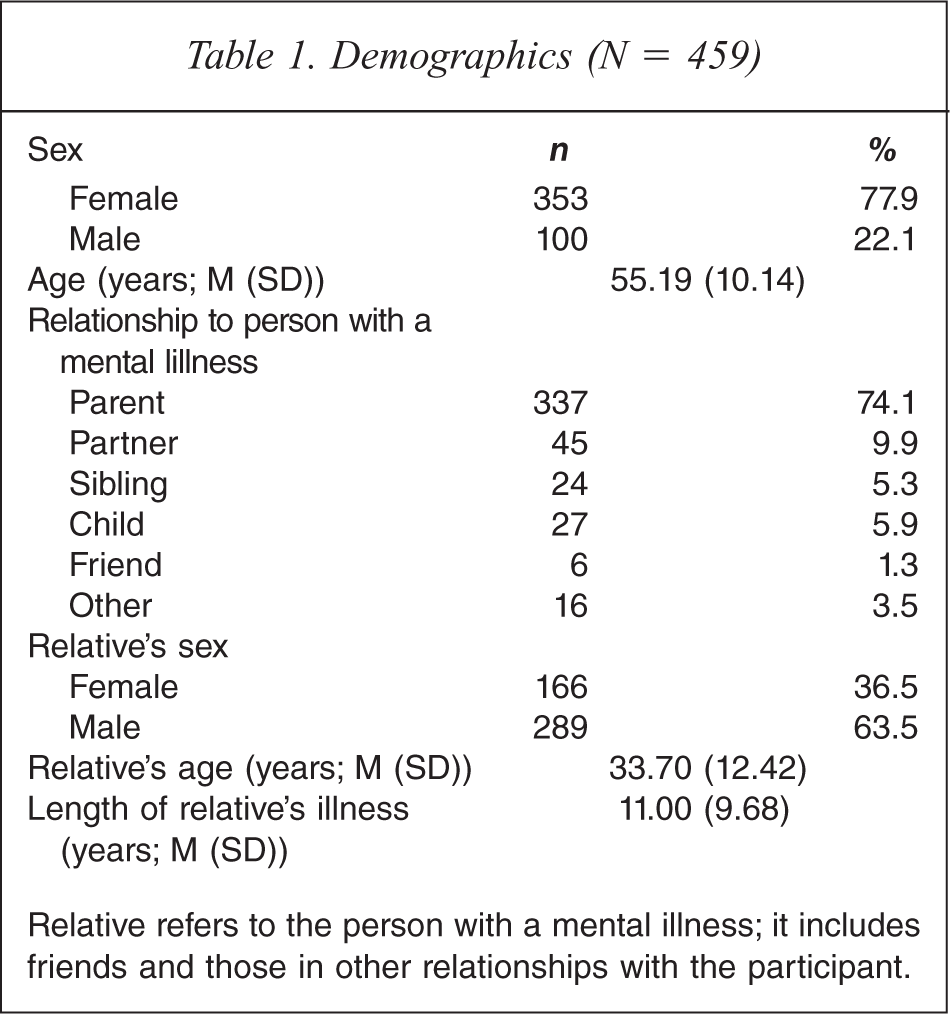
Relative refers to the person with a mental illness; it includes friends and those in other relationships with the participant.
Information about the diagnoses of participants’ relatives (collected only for participants who completed a follow-up survey, N = 156) was categorized by disorder type, and is as follows: psychotic disorder = 103 (66%); mood disorder = 60 (39%); anxiety disorder = 33 (21%); substance use disorder = 22 (14%); personality disorder = 17 (11%); eating disorder = 5 (3%); and other disorder = 17 (11%).
Participants with less than one hour per week of contact with their relative with a mental illness were instructed to skip non-applicable items from the IEQ. These participants (n = 130 at Time 1; n = 70 at Time 2) therefore obtained only a GHQ-12 and a worrying score and did not obtain a tension, supervision or urging score.
Main results
Mean scores at Time 1 and Time 2 for each subscale were calculated and are presented in Table 2, together with main effects for time from each ANOVA.
Mean Scores for Each Subscale at Time 1 and Time 2
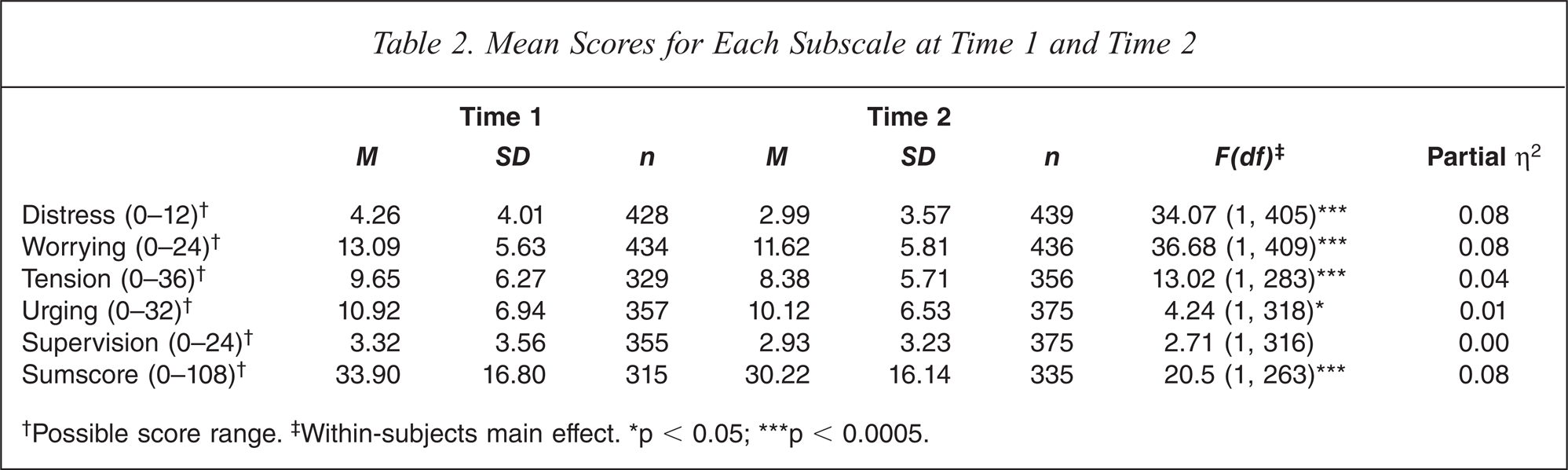
†Possible score range.‡ Within-subjects main effect. ∗p < 0.05; ∗∗∗p < 0.0005.
As shown in Table 2, there was a significant decrease from Time 1 to Time 2 for distress, worrying, tension, urging and sumscore; effect sizes for these decreases ranged from small (partial η2 = 0.01) to moderate (partial η2 = 0.08).
The proportion of participants who scored over the GHQ-12 psychiatric caseness threshold (≥3) was 54.4% at Time 1; at Time 2 it had decreased to 41.2%. A McNemar test showed that the proportion of participants with scores over the caseness threshold was significantly lower at Time 2 than at Time 1, χ2 = 22.56, p < 0.0001.
Outcomes by subgroup
Although not shown in Table 2, each ANOVA also tested interaction effects by subgroup according to sex, relationship to the person with a mental illness (mothers versus others), and relative's diagnosis (psychotic versus non-psychotic). Two significant interactions were found: carers of people with a psychotic disorder experienced significantly greater reductions in worrying than did carers of people with other types of disorders, F = 4.09 (1, 89), p < 0.05, partial η2 = 0.04 (small effect size); and females experienced significantly greater reductions in tension than did males, F = 7.77 (1, 283), p < 0.05, partial η2 = 0.03 (small effect size). These interactions are illustrated in Figures 1 and 2, respectively.
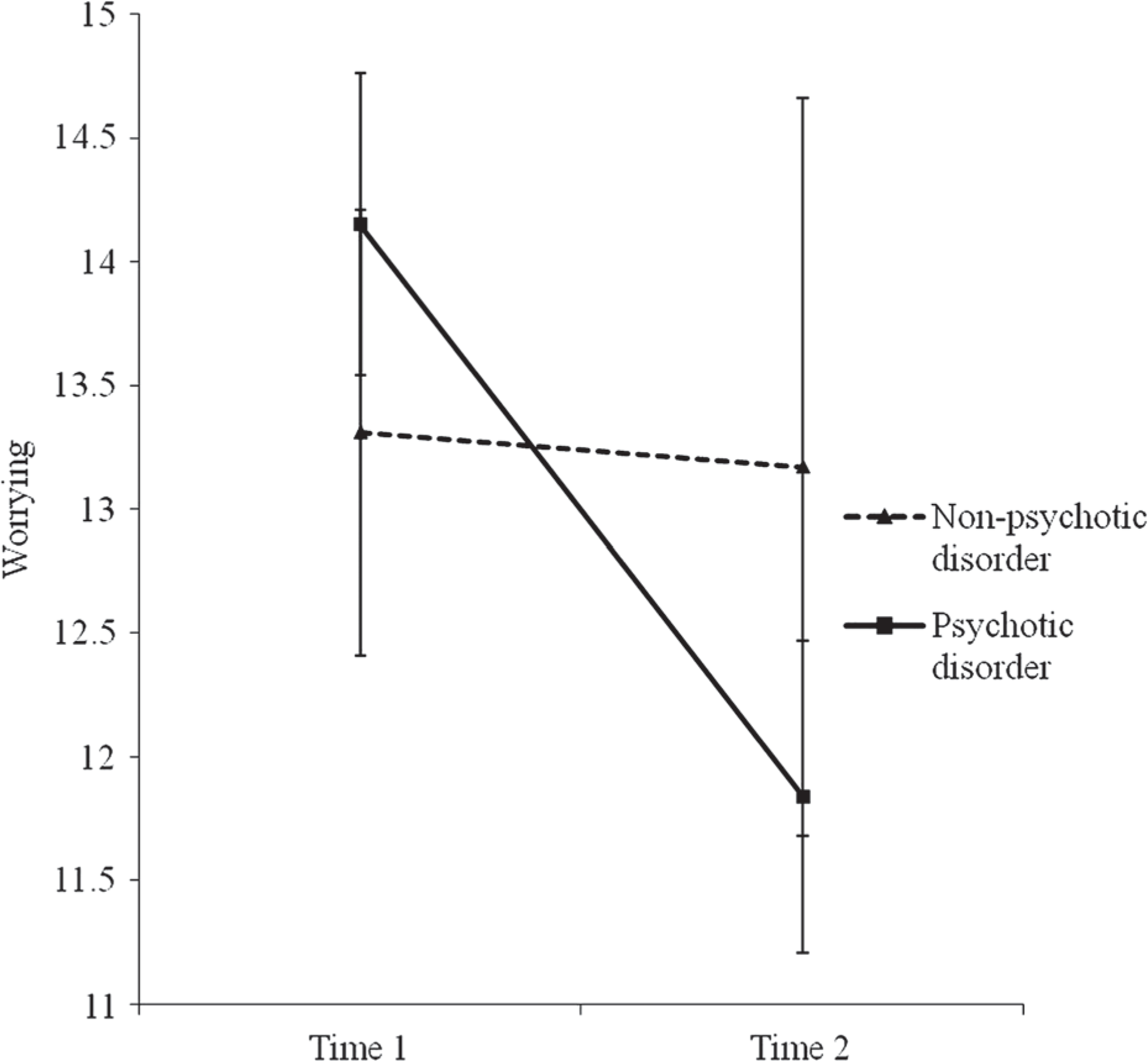
Mean worrying scores (±SE) for carers of people with psychotic disorders and other types of disorders at Time 1 and Time 2 (n = 156).
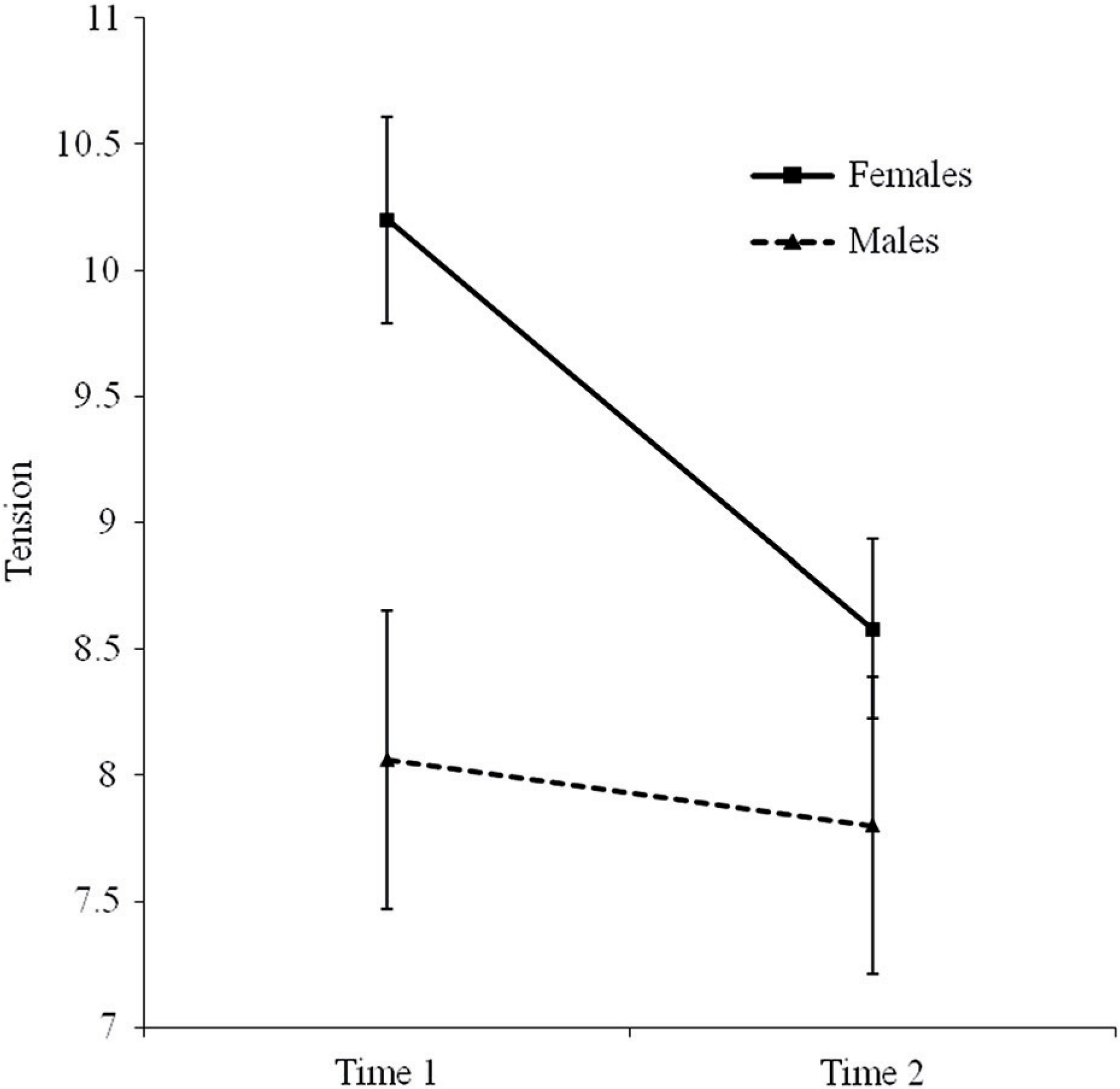
Mean tension scores (± SE) for males and females at Time 1 and Time 2.
No changes from Time 1 to Time 2 on any subscale were significantly correlated with length of relative's mental illness (correlations ranged from r = −0.04 to 0.01).
Secondary analyses
Maintenance of gains over time
Analyses were conducted on data from participants who completed the IEQ at 3 and 6 month follow up (Time 3, n = 264 and Time 4, n = 189, respectively) in order to explore whether gains in distress, tension, worrying, urging and IEQ sumscore were maintained over time. Mean scores for distress, worrying, urging and sumscore all continued to decrease across Time 3 and 4; tension scores did not decrease further (see Figure 3).
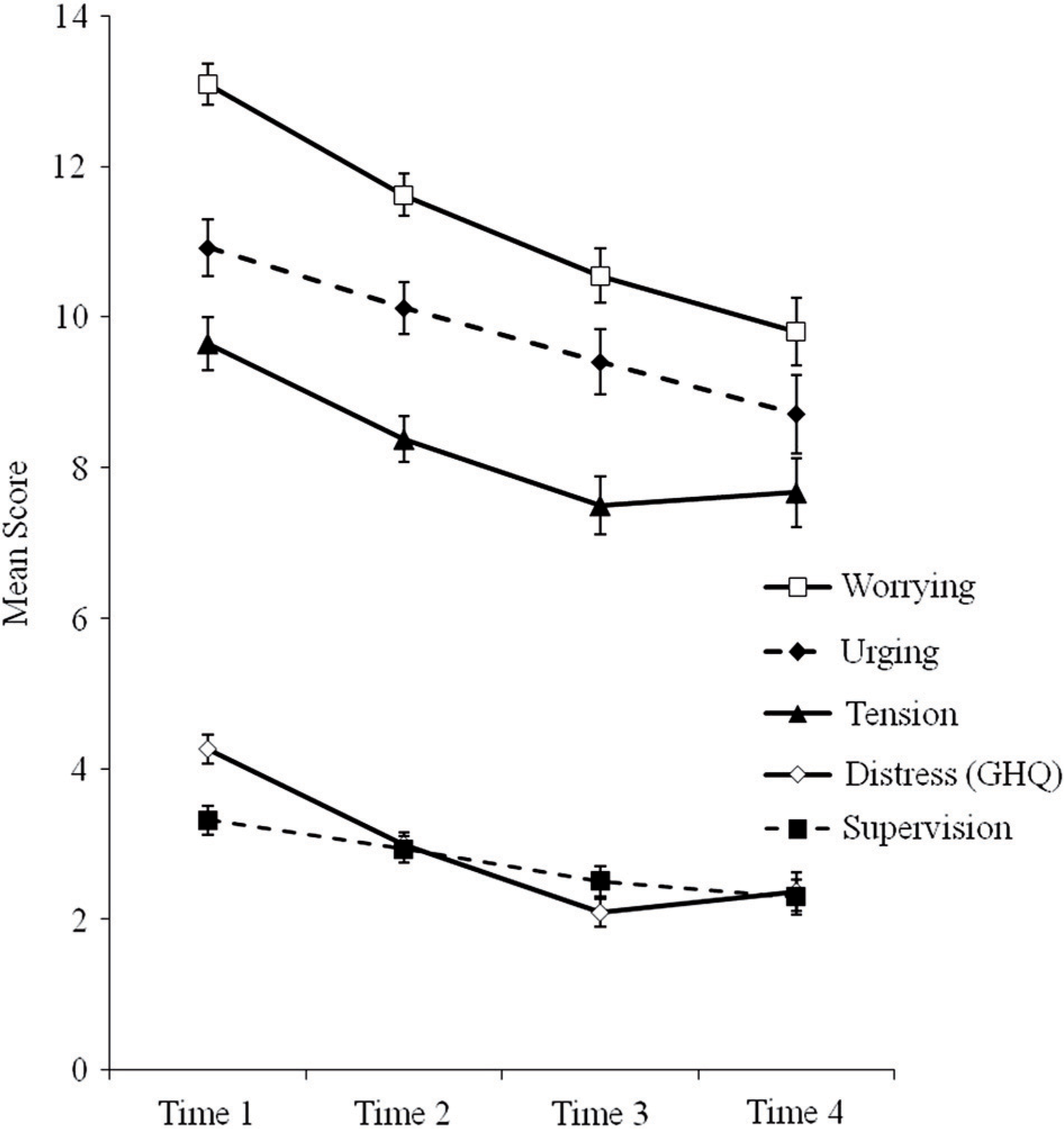
Mean scores for all subscales from Time 1–4.
Bonferroni post-hoc tests following one-way repeated-measures ANOVAs for each of the four subscales and IEQ sumscore showed that scores at Times 2, 3 and 4 were all significantly lower than at Time 1. This indicates that the improvements in care-giving consequences observed at completion of the programme were maintained over time for those participants who completed the follow-up questionnaires. Consistent with this finding, the proportion of participants who scored over the GHQ-12 psychiatric caseness threshold (≥3) had decreased to 30.3% at Time 3 and 29.6% at Time 4.
Ability to cope
We examined a single-item question that was not included within the four subscales that asked how often participants felt able to cope with their relative's mental health problems; higher scores represented greater ability to cope. A repeated-measures t-test showed that participants’ ability to cope significantly increased from Time 1 (M = 1.74, SD = 1.13) to Time 2 (M = 2.01, SD = 1.14), t (435) = −4.97, p < 0.0005, partial η2 = 0.05 (small effect). A secondary analysis was conducted to explore whether this increased ability to cope was maintained over time. A Bonferroni post-hoc test following a one-way repeated measures ANOVA for ability to cope showed that scores at Time 3 (M = 2.14, SD = 1.14, n = 266) and Time 4 (M = 2.24, SD = 1.22, n = 190) remained significantly greater than at Time 1.
Amount of contact with ill relative
We first examined the number of hours’ contact that carers had with their relatives per week as a predictor of scores on each subscale at Time 1 and Time 2. We found no significant relationships between reported number of contact hours and scores on any subscale at either time-point, nor were there any significant interaction effects between amount of contact and change scores on any subscale from Time 1 to Time 2. Second, we examined whether the participant resided with their ill relative as a predictor of scores on each subscale. Results showed participants who resided with their ill relative had significantly higher tension (F(1, 281) = 6.69, p < 0.05, partial η2 = 0.02), urging (F(1, 316) = 18.18, p < 0.05, partial η2 = 0.05), supervision (F(1, 314) = 16.55, p < 0.05, partial η2 = 0.05), and sumscore (F(1, 262) = 6.55, p < 0.05, partial η2 = 0.02 (all small effects)) at both Time 1 and Time 2 than participants who lived apart from their relative. No significant interaction effects were found, indicating that participants who lived with their relative did not gain significantly greater reductions in care-giving consequences than those who lived apart from their relative.
Discussion
Results supported our principal hypothesis that participants’ negative care-giving consequences would be significantly reduced following completion of the 8-week Well Ways course. A moderate effect size was found for reductions in worrying and distress, and there were small reductions in tension and urging. Together, these results lend support to the effectiveness of Well Ways in reducing negative care-giving consequences. Secondary analyses indicated that gains reported following the 8-week course were maintained for participants who completed the IEQ at 3 and 6 month follow up. The improvements in care-giving consequences observed here are consistent with findings from studies of other brief group-based family education programmes for carers of people with a mental illness [14,20,21], which all found reductions in various measures of negative care-giving consequences.
That supervision scores did not significantly improve is perhaps unsurprising. Supervision measures the carer's tasks of guarding their ill relative's medication intake, sleep and illness-related behaviours and, as such, may be conceptualized as an objective burden. Well Ways does not specifically target the needs and behaviour of the ill relatives, and so objective burden-type constructs are not expected to be greatly amenable to change. This finding is consistent with that of Dixon and colleagues [14], which also showed no reductions in a similar measure of supervision or other measures of objective burden following the family-to-family education programme.
We examined whether Well Ways was more effective for some carers than others, according to the type of disorder their relative experienced, carer's sex, length of the relative's illness, and the relationship to their relative. Few differences were found amongst these subgroups for any of the outcomes; these are outlined below.
Carers of people with a psychotic disorder gained greater reductions in worrying than did other carers. Given that these carers did not have significantly higher worrying scores at baseline, their greater reduction is unlikely due to a floor effect (whereby carers of people with non-psychotic disorders were already experiencing low initial levels of worrying). Instead, it appears more likely that carers of people with psychosis gained greater reductions in worrying because the content of the programme was more relevant to them (Well Ways has a greater focus on psychosis than on other types of mental illness), or because they had more in common with other group members, being the largest majority subgroup. These possibilities require further investigation, including an examination of group factors, and an examination of participants’ feedback about programme content and relevance according to their relatives’ disorder type. The latter would then guide the decision as to whether Well Ways is better delivered to separate subgroups based on their relative's disorder.
Females showed significantly greater reductions in tension than did males. The implications of this result for the effectiveness of Well Ways for males need careful consideration. Females’ significantly higher tension at baseline is interesting given they did not report having more contact with their ill relatives. This suggests gender differences in aspects of care and support provided, or in perceptions of tension in the relationship between carer and care recipient. Previous research has found that women are more involved in their ill relatives’ daily activities, and are more burdened by their caring role than are men [26]. This is partially consistent with this study's findings in that, together with significantly greater tension at baseline, there were trends towards females’ having higher levels of other negative care-giving consequences at baseline. A logical argument follows that since females tend to be more involved in care-giving and experience greater negative consequences such as tension in the caring relationship, they derive greater benefit than males do from carer support and education programmes. This argument is partially supported by the finding of greater reductions in tension scores for females. Additional means by which females derived greater reductions in tension during the course may have arisen from being in the majority (groups were predominantly female) and also from having a female facilitator (most facilitators were female). These gender-based group factors are worthy of further investigation.
A further, not incompatible, possibility should be acknowledged. It has been suggested that, although male and female carers experience similar levels of negative care-giving consequences, men are less likely to acknowledge their distress [27]. Hence, males may have had less willingness to report negative consequences prior to participation; in effect, males may have been under-reporting tension at baseline. Participating in Well Ways may have encouraged males to recognize and acknowledge negative care-giving consequences (processes explicitly addressed within the programme); hence, any improvements in males’ tension may have been partially cancelled out by their increased likelihood of reporting it.
Perhaps it is likely that both explanations contributed to the finding of females’ greater reductions in tension. Clearly, further research that directly assesses some of these variables and processes would help to investigate these possibilities. Based on our findings alone, however, there is insufficient evidence to suggest that family education programmes such as Well Ways are less effective for males, or that they would be more effective if provided separately to males and females.
No association between length of illness and scores on any subscale was found; more experienced carers derived as much benefit from the programme as newer carers. Likewise, no association was found between the relationship between carer and relative (or friend) and scores on any subscale.
Limitations
Three main limitations related to sampling were present in the current study. The first was that we did not use a control group, so any inferences about Well Ways having caused the improved outcomes are tentative. The reductions in care-giving consequences may have been due to factors other than participation in the programme, such as so-called continued maturation [28], whereby carers’ ability to cope with their relatives’ illness naturally increases over time. However, it is unlikely that the magnitude of such maturation effects from Time 1 to Time 2 (approximately 8 weeks) would have been great, given that the mean length of time that participants had been caring for a person with a mental illness was 11 years. It is more plausible that reductions in care-giving consequences arose from a combination of the intervention and continued maturation. Pickett-Schenk and colleagues [20] suggested a similar explanation for their study's findings that although their family education intervention group showed significantly greater gains than their control group, the control group also improved over time.
The second sampling limitation relates to attrition bias. The drop in questionnaire completion rates from Time 1 to Time 4 limits the findings of improvements over time, given the possibility that participants who gained most from the programme were more likely to complete the questionnaires. Similar studies in the future could consider putting in place more assertive strategies for ensuring completion of questionnaires at every time-point, such as reminders or incentives.
The third sampling limitation was that the sample representativeness was not assessed, thus limiting the generalizability of this study's findings to all carers of a person with a mental illness.
Because attendance at the eight sessions was not consistently recorded at all sites, the extent to which differential rates of completion affected the results is not known. Anecdotal findings from a retrospective survey of facilitators indicated a high retention rate; approximately 80% of participants attended most or all of the eight sessions. This would suggest that the drop in completion of the questionnaires across time was not due to difficulties in retention. However, it does not answer questions about whether greater attendance at sessions contributed to improved outcomes generally and for specific subgroups; for example, did carers of people with psychosis attend more sessions, given the programme was more specific to their needs, and did this contribute to their achieving better outcomes? A related limitation was the lack of consistent recording procedures for attendance at the third phase of the Well Ways programme; anecdotally, however, the majority of participants did not attend the follow-up sessions offered as part of the third phase of the programme. Therefore, the long-term benefits shown by those participants who completed Time 3 and 4 outcome measures were unlikely to require attendance at the third phase.
Future research
Specific suggestions for further research may be drawn from the findings and limitations in this research project. The first is that a control group, such as a waiting list control, would allow future studies to draw conclusions about causality, lending greater weight to findings. Future studies could collect information about the diagnoses of carers’ relatives in order to test whether the finding of greater improvements in worrying for carers of people with psychosis is replicable and generalizable to other outcomes; if so, this would imply that programmes such as Well Ways may be more effective if delivered to subgroups of carers based on their relative's disorder.
Future research could aim to identify the effective elements of Well Ways and other family education programmes. For example, therapeutic group processes and peer modelling are two likely effective components of Well Ways that are amenable to evaluation. Further, an examination of mediators and other mechanisms of change, such as changes in family stigma, grief and empowerment, could provide valuable insight into how family education works.
Conclusion
This study supported the effectiveness of the Well Ways programme in reducing negative care-giving consequences for families of people with a mental illness. Findings of significantly improved outcomes following eight sessions of family education are particularly notable given that a previous review by Dixon and colleagues [17] found no evidence that brief programmes of less than 10 sessions’ duration produced any significant improvements in family burden. Programmes such as Well Ways may be an effective, accessible and affordable option for individuals who provide care for a relative with a mental illness. The importance of such programmes is considerable given the evidence of poor psychological health and negatively appraised family relationships observed at baseline.
Further research into the effectiveness of family education programmes and the mechanisms by which they exert their effects would be valuable. Research that incorporates the recommendations outlined above would help to more effectively test the efficacy of such programmes and to inform their ongoing development.
Footnotes
Acknowledgements
We thank research assistants Taisia Thompson and Katelyn Moore for collecting and entering data.