
Abstract
Disasters involving widespread loss of life and property may result in a range of mental health outcomes among the affected population [1]. A proportion will show a ‘resistant’ trajectory of recovery, reporting few or no clinically significant symptoms, while a small minority will develop persistent diagnosable psychiatric conditions. Between these extremes, a large group of survivors are likely to develop mild to moderate clinically significant symptoms [1–3]. This latter group is important because although their psychological distress may not be sufficient to warrant full mental health intervention, they nonetheless contribute to marked distress, reduced productivity, interrupted relationships, and can subsequently develop into significant psychiatric disorder. Accordingly, it is incumbent upon response agencies to ensure, for reasons of both economic impact and human suffering, that appropriate mental health interventions are provided to promote psychological recovery for this significant proportion of disaster survivors. One component of such recovery programmes typically involves provision of assistance by existing health providers.
On Saturday 7 February 2009, a series of severe bushfires in Victoria, Australia, resulted in Australia's worst natural disaster: 173 people died, 7000 people lost their homes, and several entire communities were devastated. In the aftermath of this disaster, the Australian and Victorian State governments met with experts in psychological trauma, as well as health professional associations, to discuss how best to facilitate psychological recovery among survivors of the fires. An evidence-informed framework was developed outlining recommended levels of care underpinned by an education and training agenda [4,5].
The framework identified three levels of response. The first (level 1) was consistent with current models of psychological first aid (PFA) [6]. PFA is an evidence-informed approach recommended in Australian [7,8] and international [9–11] guidelines for assisting people in the immediate and short-term aftermath of disaster. A detailed manual guide to PFA is available from the US National Center for PTSD website (www.ncptsd.va.gov) and the US National Child Traumatic Stress Network website (www.nctsn.org). This approach acknowledges that immediate debriefing to all survivors that involves disclosure of one's reactions is not optimal [12], but rather emphasizes social support, problem-solving, and addressing immediate needs.
At the other end of the spectrum, level 3 focused on the minority of survivors who were likely, over time, to develop a diagnosable mental disorder. Based on reports following previous disasters internationally [1], it was expected that the predominant disorders would be PTSD, depression, complicated grief, anxiety, and substance abuse. An intensive training programme was developed for mental health practitioners to equip them in providing evidence-based treatments targeted at these post-disaster psychiatric disorders.
The focus of the current review, however, is on second level of care (level 2). This level 2 initiative was designed for primary and allied health providers treating survivors with mild to moderate distress, including worry, sadness, insomnia, anger, decreased ability to function at work, school or home, or other psychological issues after the fires, that did not warrant formal mental health intervention. It was assumed that this level of distress or dysfunction would be more common than diagnosable mental disorders and that these conditions would remain prevalent over the ensuing months, fuelled by practical issues arising from bereavement, destruction of property and other possessions, relocation, and rebuilding. This need is highlighted by evidence following Hurricane Katrina that there were increases in mental health problems as time elapsed following the hurricane [13].
Up until this point, in the space between PFA in the short-term aftermath and clinical interventions for diagnosable psychiatric disorders over the longer term, there has been little in the way of structured evidence-informed intervention models. A recently developed model called Skills for Psychological Recovery (SPR) was identified as appropriate for survivors with this type of ongoing distress (Berkowitz S, Bryant R, Brymer M, et al. National Center for PTSD and National Child Traumatic Stress Network. Skills for Psychological Recovery: Field Operations Guide: Unpublished draft edition, 2009). Since SPR was only recently developed, and is the first formal, manualized approach designed for the large numbers of disaster survivors with mild to moderate psychological difficulties, this paper describes the nature and roll out of an education programme for health practitioners in bushfire affected areas. In the context of describing the implementation of SPR, we also provide an overview of practitioner perceptions of the model.
Skills for Psychological Recovery
The SPR protocol was recently developed by the US National Center for PTSD (NCPTSD) and the US National Child Traumatic Stress Network (NCTSN), as well as some outside consultants. Indeed, it was still in draft form at the time of the Victorian bushfires. Designed for practitioners of varying backgrounds and qualifications, it is: (i) based on extensive research of the most common emotional and behavioural reactions arising after disasters in adults and children; (ii) aimed at developing the briefest but most effective strategies derived from evidence-based approaches to managing these reactions; and (iii) formatted to ensure that training and delivery would be feasible in the wake of massive disasters. It is intended to assist people across developmental levels in coping with mild depression, anxiety, grief, post-traumatic stress, anger, and ongoing difficulties in the disaster setting. Each skill is taught in terms of working with adults, children, or families. Because many survivors will only consult a health care provider on one or two occasions, and often not in a traditional ‘consulting room’ setting, it is designed for single or multiple sessions delivered in a range of environments. Although the protocol encourages attendance at multiple sessions to maximize benefit to the survivor, each session is designed as a ‘stand-alone’ intervention.
SPR comprises six core modules that can be used by the provider depending on the survivor's needs:
Gathering information and prioritizing assistance: This module was conceptualized as the foundation for all the SPR skills, partly because many survivors may only attend for a single session, and partly because choosing which SPR skills to work on should be based on a good understanding of the survivor's concerns and priorities. There is evidence that identifying and understanding psychological reactions can have benefit in reducing distress [14]. This three-stage component (i) identifies the survivor's primary concern, (ii) feeds back to the survivor a problem formulation that places this presenting problem in a framework, and (iii) suggests an action plan. Gathering information and prioritizing assistance gives a map for choosing which SPR skills to work on. Handouts and worksheets are provided to help the survivor learn the steps. If the survivor cannot attend for a second session, handouts are provided to direct him or her to outline the steps required to address other problems he or she might have identified.
Building problem-solving skills: This skill teaches the survivor to break his or her problem into manageable and sequential components, and to identify the steps to addressing the problem. This strategy is extremely useful after a disaster because it is applicable to a wide range of events and, in the aftermath of widespread destruction, many survivors may be grappling with a variety of practical problems. Evidence indicates that problem-solving is an efficacious intervention for mental health problems [15], and anecdotal reports suggest that this component was the most widely used skill in New Orleans after Hurricane Katrina.
Promoting positive activities: This skill is based on evidence that the major behavioural means to reduce depression and associated conditions is to increase activity, routine, and positive events [16]. It teaches the survivor to proactively structure activity schedules in collaboration with the health provider.
Managing reactions: This skill aims to assist people to manage the distress they feel, manage reminders of their distress, and also to begin to resolve their distress through simple exercises that promote emotional processing and discussion. It includes a number of skills such as breathing retraining, writing about one's experiences, and identifying and planning for triggers and reminders. All are based on evidence that these strategies are beneficial in reducing post-traumatic distress [17–19].
Promoting helpful thinking: This strategy is based on much evidence that maladaptive or catastrophic appraisals after trauma strongly maintain psychological conditions, and with converging evidence that cognitive restructuring effectively reduces anxiety and depression after trauma [20–22]. This skill teaches people to identify the common maladaptive appraisals made after a disaster, and to rehearse different appraisals.
Rebuilding healthy social connections: This skill is based on evidence showing that, while social support buffers many adverse psychological reactions to disaster, social networks and the support that they normally provide are often severely disrupted by disaster [23]. It specifically teaches people to access social and community supports in a practical way.
The SPR protocol is intended to give health providers a repertoire of skills that build upon their existing professional competence to assist the disaster survivor. The protocol does not specify that the skills are to be applied in any specific order or which skills must be applied with a particular individual. The modular skills are instead designed to be selected based upon an assessment of the presenting problems, perceived needs, and priorities of the individual survivor. Thus, the intent is to use these skills in the context of existing competencies and provider judgement, not as a ‘cookbook’ in isolation of good practice.
Although the draft SPR manual had only just been completed, the original authors consented to make it available for the Victorian fires recovery effort. Considerable amendment and abbreviation of the manual to ensure it was suitable to local needs was conducted by three of the current authors (RB, DF, MC) with the full permission and cooperation of the original SPR developers.
Method
Workshop participants
A two-day ‘train the trainer’ workshop was developed and delivered by the authors (RB, MC, and DF) to 30 trainers selected by health discipline professional bodies. Those trainers then conducted approximately 25 one-day SPR workshops in the bushfire affected areas between 30 May and 24 August 2009, with a total of 342 participants.
Participants in the SPR workshops were overwhelmingly female (n = 267, 79%), with a mean age of 48 years (SD = 10.2). On average they had been providing health services for 14 years. They were drawn from a full range of health disciplines including psychology (n = 152, 45%), social work (n = 59, 18%), medicine (n = 25, 7%), nursing (n = 24, 7%), and general counsellors (n = 34, 10%), with the remainder identifying themselves as working in psychosocial rehabilitation, occupational therapy, and case management (n = 44, 13%). A total of 17% of participants (n = 55) reported having ‘a lot’ of experience in treating people following disasters or trauma, with 41% (n = 137); 38% (n = 128); 4% (n = 14) reporting having moderate, a little and no experience in this area respectively.
Participants described the theoretical framework that most informed their clinical work as cognitive-behavioural (n = 169, 44%), person-centred/Rogerian (n = 65, 19%), narrative (n = 38, 11%), solution focused (n = 93, 10%), psychodynamic (n = 32, 9%) and systemic (n = 24, 7%).
Procedures
Participants were administered a pre-workshop questionnaire that asked them to rate the extent they agreed or disagreed on 4 point Likert scales (1 = ‘strongly disagree’, 4 = ‘strongly agree’) with the following statements:
Evidence-based treatments are too prescriptive. They do not take into account individual clinical judgement;
I would be reluctant to use a therapy/intervention that follows a treatment manual.
Following the workshop, participants were asked to rate on a 5 point scale (1 = ‘poor’, 5 = ‘excellent’) (i) the overall quality of the educational components as a learning experience and on a 5 point scale (1 = ‘not at all’, 5 = ‘very’) (ii) whether the workshop was well presented and interesting; (iii) whether SPR was relevant to their work; (iv) their likelihood of using SPR in their practice; (v) their confidence in using SPR; and (vi) the usefulness of each of the six modules. The aim of the pre-workshop questions on perceptions of evidence-based and manualized interventions was to assess the degree to which these views affected their experience of the training, their likelihood of using the SPR, and their perceptions of the usefulness of the six modules. Completion of the questionnaires was voluntary and participants were informed prior to completion of the questionnaires that responses would be used for the purposes of research.
A subset of 20 SPR-trained practitioners monitored their use of SPR over the course of the three months post-training in the context of their routine clinical work using log sheets. Across these 20 practitioners, 61 log sheets recording their use of SPR were returned. Log sheets required these practitioners to note the traumatic event experienced by the client and the issues they initially presented with. They were then asked to indicate which of the SPR modules they had used with that particular client (for up to six sessions) and, on a scale from 1 (not at all) to 5 (very), how confident they were in delivering that module and how useful they thought the client found it. Finally, the log sheet asked whether the client had received treatment other than SPR and, if so, whether that treatment was psychological or pharmacological.
Results
Perceptions of evidence-based treatments and use of manualized interventions
Prior to the workshop, approximately one third of participants perceived evidence-based treatments as too prescriptive (30% (n = 93) scoring 3 (agree) and 2% (n = 7) scoring 4 (strongly agree) on the 4 point scale) and 20% of participants (17% scoring 3 and 3% scoring 4 on the 4 point scale) reported that they would be reluctant to use an intervention that followed a treatment manual.
Evaluation of SPR workshops
Evaluations of the workshops are presented in Table 1.
Mean scores for SPR evaluation items (N = 343)
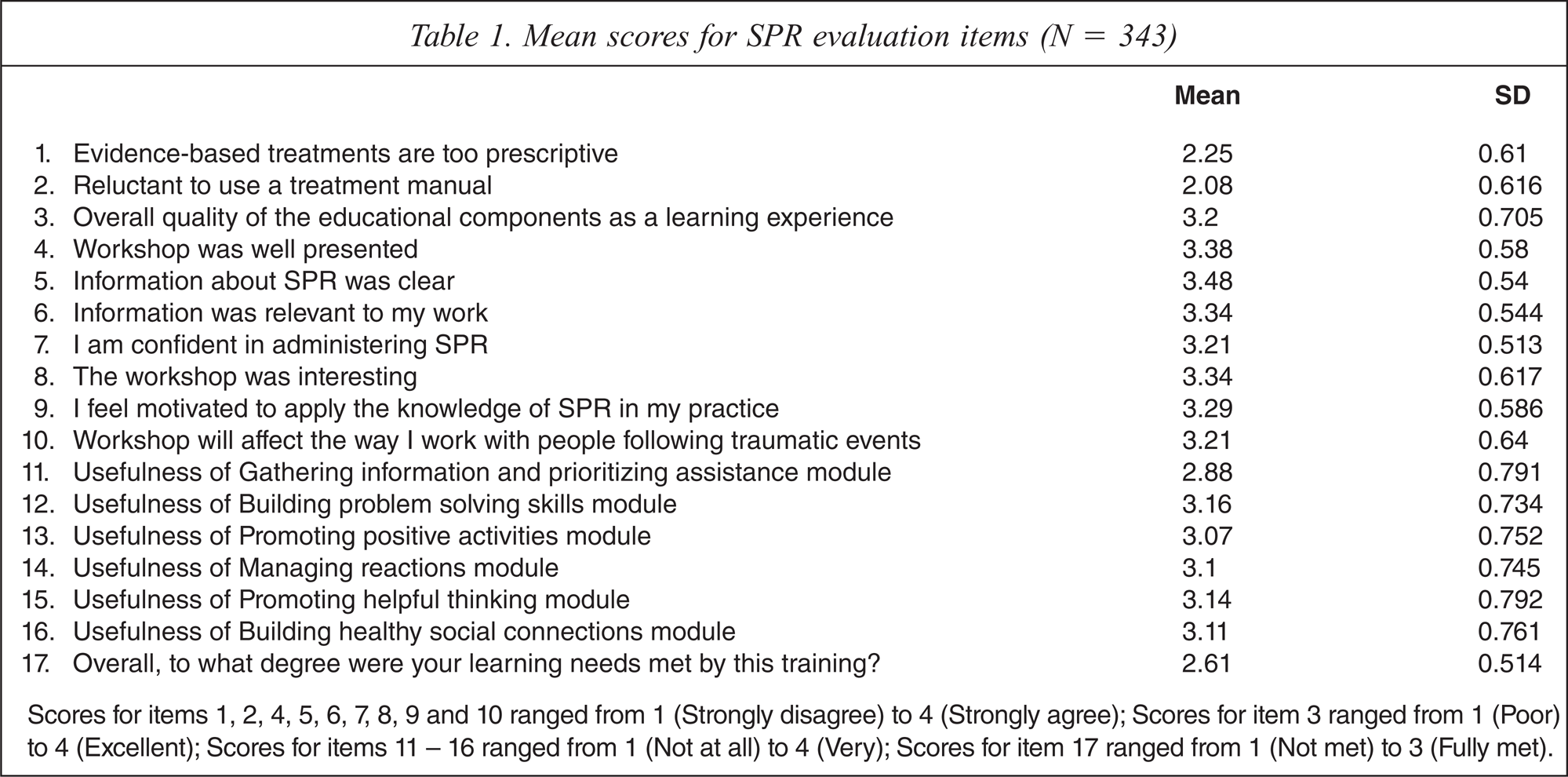
Scores for items 1, 2, 4, 5, 6, 7, 8, 9 and 10 ranged from 1 (Strongly disagree) to 4 (Strongly agree); Scores for item 3 ranged from 1 (Poor) to 4 (Excellent); Scores for items 11 – 16 ranged from 1 (Not at all) to 4 (Very); Scores for item 17 ranged from 1 (Not met) to 3 (Fully met).
Overall, the SPR workshop was rated as a positive experience, with only a minority of participants reporting that the information provided was not relevant to their work (n = 10, 3%), that they were not confident in administering SPR (n = 16, 5%), that they were not motivated to apply their knowledge of SPR to their clinical work (n = 19, 6%), and that they would not pass on the information learned or recommend the training to colleagues (n = 23, 7%).
The six modules that make up the SPR approach were rated fairly evenly, with between 65% to 85% of participants rating them as being at least ‘quite useful’. Overall, each module was rated comparably with the exception of ‘Gathering information and prioritizing assistance’, which was rated slightly less positively.
Pearson correlation analyses examining the relationship between perceptions of evidence-based research with overall perceptions of SPR and of the six SPR modules were conducted. Unfavourable perceptions of evidence-based interventions were negatively associated with motivation to apply SPR in clinical practice (r = −0.17, p < 0.01) and, specifically, perceptions of the usefulness of the Gathering information and prioritizing assistance (r = −0.13, p < 0.05), Promoting helpful thinking (r = −0.16, p < 0.01) and Managing reactions (r = −0.13, p < 0.05) modules. However, this item was not related to perceptions of the usefulness of specific modules of Promoting positive activities (r = −0.05, n.s.), Building problem solving skills (r = −0.09, n.s.) or Rebuilding healthy social connections (r = −0.1, n.s.).
Pre-workshop reluctance to use manualized interventions was negatively related to motivation to apply SPR in clinical practice (r = −0.13, p < 0.05) and the perceived usefulness of the Gathering information and prioritizing assistance (r = −0.16, p < 0.01), Promoting helpful thinking (r = −0.14, p < 0.01) and Building problem solving skills (r = −0.14, p < 0.01) modules. It was not associated with perceptions of the usefulness of Rebuilding healthy social connections (r = −0.04, n.s.), Managing reactions (r = −0.1, n.s.), or Promoting positive activities (r = −0.02, n.s.).
Monitoring of ongoing use of SPR
Table 2 presents the mean ratings derived from the 61 log sheets returned (range per practitioner 1–14 with a mode of 4); 46% of the log sheets reflected the use of SPR with adult clients who presented with issues related to the bushfires, and 54% used SPR to address ongoing problems following other traumatic events. The issues people presented with could be grouped into a few broad categories including anxiety, depression, substance abuse, relationship problems and grief. Providers saw clients for an average of four sessions. Gathering information and prioritizing assistance was the most commonly used module (in 93% of the 61 cases), while the remaining modules were used fairly equally (range: 67% to 77%). Providers were generally very confident about administering the modules and thought their clients found the modules ‘quite useful’. Providers were least confident about administering the Managing reactions module.
Mean practitioner confidence and perceived client usefulness of SPR modules (N = 61)
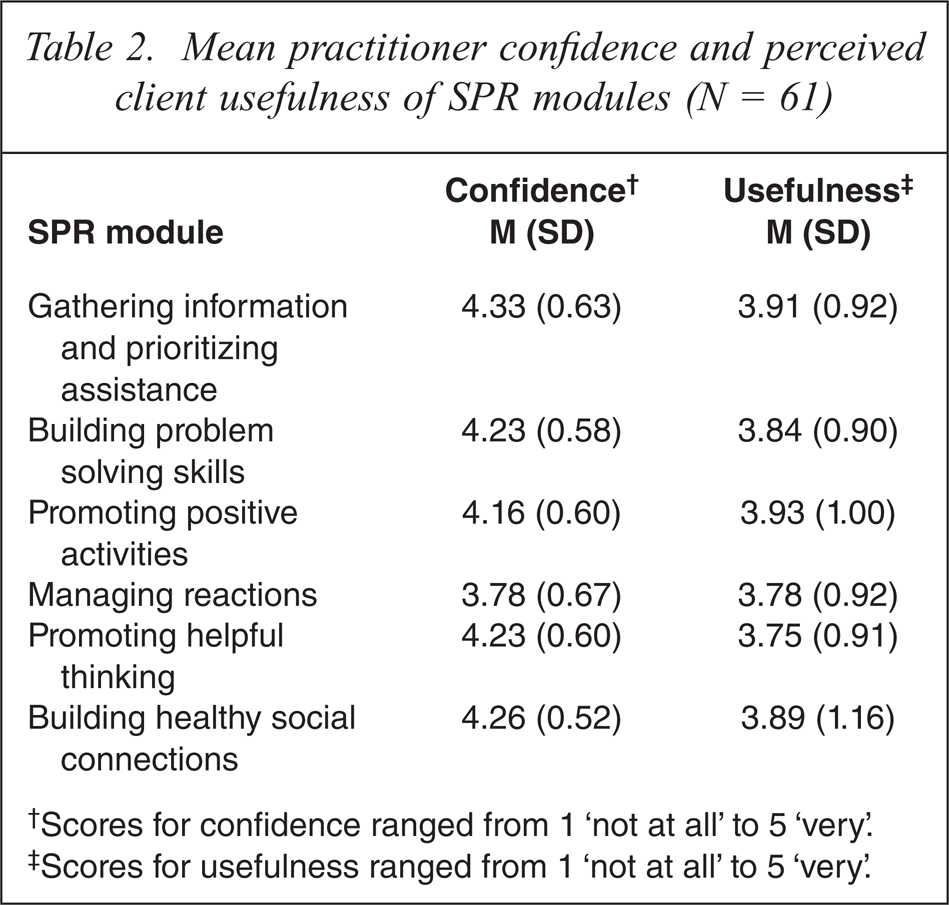
†Scores for confidence ranged from 1 ‘not at all’ to 5 ‘very’.
‡Scores for usefulness ranged from 1 ‘not at all’ to 5 ‘very’.
Conclusions
The Victorian bushfires required an unprecedented education and training response to ensure, as far as possible, that psychological assistance was provided in line with best practice. For the first time, this included a formal intervention, called SPR, aimed at survivors with ongoing mild to moderate distress for whom optimal intervention fell between the provision of PFA and interventions for mental health disorders. This study represents the first preliminary evaluation of the implementation of the SPR protocol in response to a disaster. The evaluations indicated that the SPR workshops were well received. Practitioners were largely satisfied with the experience, found the information relevant to their work, were confident in administering SPR directly following the training, were motivated to apply their knowledge of SPR to their clinical work and indicated that they would pass on the information they learned or recommend the training to colleagues. The majority of participants rated each of the SPR modules as being useful with the exception of the Gathering information module, which was rated slightly less positively. This finding may be due to the fact that the skills and actions required to implement this module are too basic for experienced health providers. Despite this, as would be expected in following the SPR protocol, Gathering information and prioritizing assistance was the module used most often by providers as the entry point into SPR.
Negative perceptions of evidence-based approaches were associated with lower motivation to apply SPR in clinical practice, and lower perceptions of the usefulness of the Gathering information and prioritizing assistance, Promoting helpful thinking, and Managing reactions modules. This suggests that those who believe evidence-based treatments are too prescriptive may be less likely to use these modules. Interestingly, perceptions about evidence-based treatment did not affect perceptions of the usefulness of Building problem solving skills, Rebuilding healthy social connections and Promoting positive activities modules. Similarly, an expressed reluctance to use manualized interventions was negatively related to motivation to apply SPR in clinical practice, but perceptions of manualized interventions did not affect preparedness to apply Rebuilding healthy social connections or Promoting positive activities modules. It appears that Facilitating social connectedness, Problem-solving, and Encouraging increased positive activity are not susceptible to the negative biases associated with perceptions of evidence-based protocols. There is much evidence that the majority of practitioners do not employ evidence-based treatments for trauma survivors [24]. Accordingly, one conclusion to draw from these patterns in terms of dissemination is that training will optimally succeed when training practitioners to engage in positive activity scheduling, as well as rebuilding social connectedness and problem solving skills; considering that these strategies have strong evidence for their capacity to enhance recovery following disasters, it seems wise to place emphasis on them.
Encouragingly, data provided by practitioners who completed log sheets three months after training indicated that these practitioners were confident about administering SPR and thought that their clients found the interventions to be useful. Gathering information and prioritizing assistance was the most commonly used module, while the other modules were used fairly equally. Practitioners were found to be least confident in administering the Managing reactions module, which may reflect general health practitioners’ apprehensions in addressing trauma memories and the associated affect.
Clearly, this report represents preliminary reactions to implementation of SPR following a major disaster. We note that these responses were limited to experienced practitioners, there was no control group who did not receive training, the measure used to examine practitioner perceptions had not been psychometrically tested and no adherence to protocol measures were available. Most importantly, it was not possible to rigorously evaluate the impact of SPR implementation on survivors’ mental health outcomes. Future studies should explore why some SPR modules were less likely to be administered, what barriers were encountered in providing SPR, survivor satisfaction with SPR, and the use of SPR with other disasters. It will be important for randomized controlled trials to evaluate the efficacy of this approach, focusing on both symptoms and positive adaptation among survivors to reflect the specific goals of SPR. To help those who did not feel confident using the skills after the training, exploring other training platforms such as providing ongoing consultation or increasing practice is important. The initial indications, however, are that SPR is acceptable to the majority of practitioners and it is an approach that practitioners are willing to implement following brief, easy to provide training.
Footnotes
Acknowledgements
The authors would like to thank the Commonwealth Department of Health and Ageing and the Australian Psychological Society for their support in the development and delivery of the SPR training. We would also like to thank the developers of SPR for their permission to use it in the aftermath of this disaster.