
Abstract
In the field of traumatic stress, chemoprophylaxis is a term that is often used but rarely well understood. There has been no shortage of debate on the issue, but few rigorous studies to ground the discussion. The purpose of the current paper is to explore the issues surrounding this contentious area. Databases including PubMed, PsychArticles and Web of Knowledge were searched using the key words ‘chemo or pharmaco’, ‘prevention or prophylaxis’, and ‘PTSD or post-traumatic stress’. Relevant journals and reference lists of the papers obtained through this search were scanned for additional references. Studies that investigated the use of pharmacotherapy to prevent the onset of post-traumatic stress disorder were considered for this paper. Studies that examined the treatment of established PTSD were excluded. A total of 15 empirical studies were included in the review (including five randomized controlled trials), and twice as many non-data-driven papers. Evidence for the prophylactic use of alcohol, morphine, propranolol, and hydrocortisone is presented, followed by a discussion of the many challenges of using pharmacological interventions in this context. While attention to this issue has increased in recent times, the dearth of empirical data has done little to further the field. Larger studies are indicated following small trials with medications such as propranolol and hydrocortisone. There remain a number of ethical and practical questions to be answered before the widespread use of chemoprophylaxis can be recommended.
Keywords
Chemoprophylaxis, particularly in the field of traumatic stress, is a term that has been used to convey a range of possible meanings. Since this is potentially a contentious and difficult area, it is important to be absolutely clear about what is meant by the term. The Oxford English Dictionary [1] defines chemoprophylaxis as ‘the prevention of a disease, esp. an infectious disease, by the administration of drugs’. Crucially, the word ‘treat’ does not appear in the OED definition. Thus, in the context of traumatic stress, the term chemoprophylaxis refers to the use of pharmacological interventions to prevent the development of mental health problems in individuals exposed to trauma. It does not refer to the treatment of an established disorder.
Traditionally, efforts to prevent post-traumatic stress disorder (PTSD) have been classified as either primary (intervention prior to the traumatic event) or secondary (intervention after the trauma but prior to the onset of full PTSD). We will discuss the former briefly; however, secondary prevention is the more common approach to chemoprophylaxis and thus will be the focus of this paper.
Despite a few randomized controlled trials, much of the literature to date has been largely theoretical in nature, or has relied on opportunistic research, with numerous and conflicting viewpoints being proposed. The purpose of the current paper is to explore the issues surrounding chemoprophylaxis for PTSD. While this paper will focus on preventing PTSD through pharmacological means, it needs to be noted that a parallel stream of literature exists addressing issues and preliminary research using psychosocial models of intervention (individual and community resilience building) [2,3].
Literature review
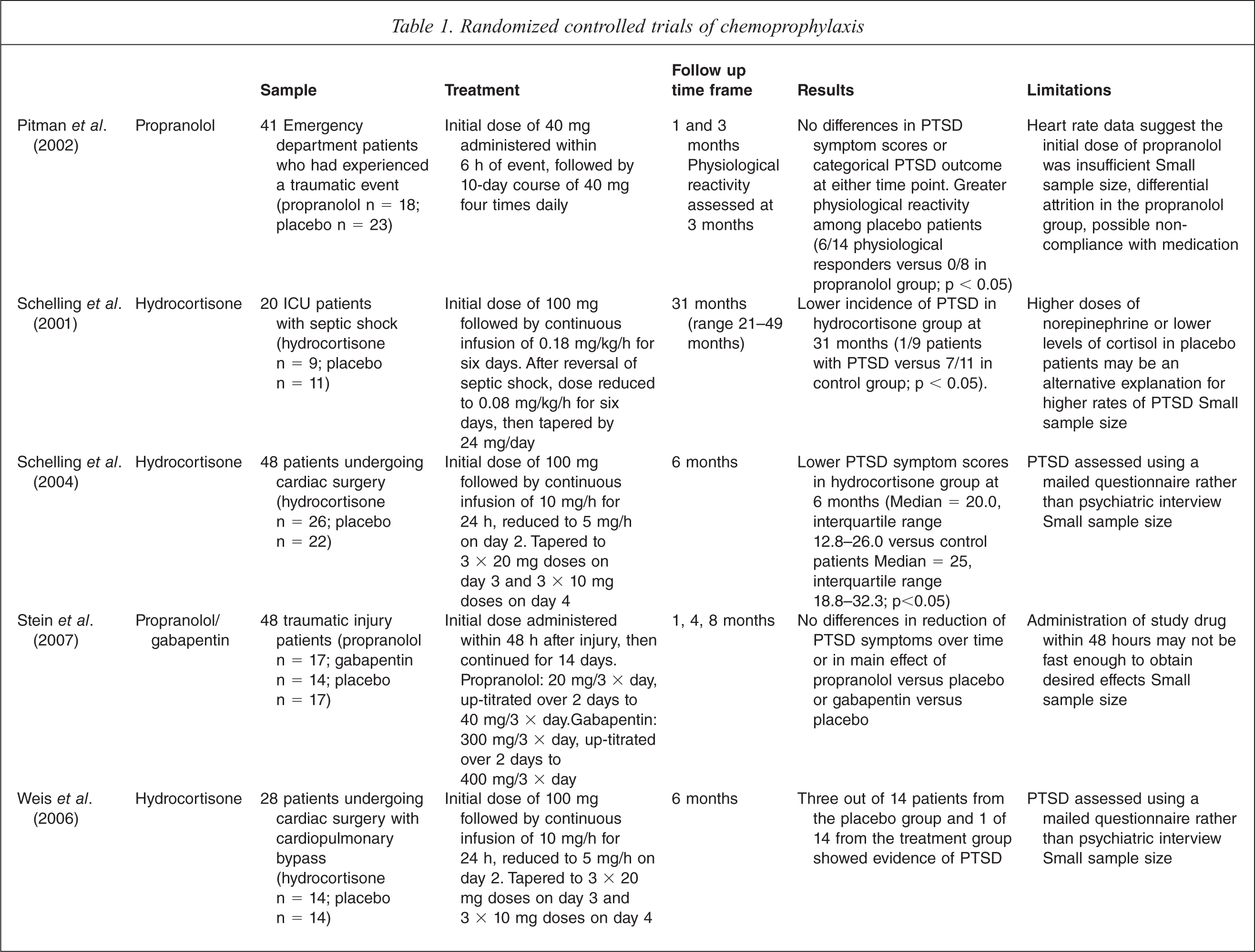
Databases including PubMed, PsychArticles and Web of Knowledge were searched using the key words ‘chemo or pharmaco’, ‘prevention or prophylaxis’, and ‘PTSD or post-traumatic stress’. Additional references were sourced from the reference lists of key papers obtained from database searches, and by scanning the contents of relevant journals. After excluding papers outside the scope of the current review, fifteen data-driven papers remained (including five randomized controlled trials; see Table 1), published between 1996 and 2010. A total of 30 non-data-driven papers (such as review, conceptual or ethical debate papers) were also included. Taken as a body of literature, these papers raise several issues for consideration.
Randomized controlled trials of chemoprophylaxis
Preventing PTSD: the options
Traumatic events are reasonably common, with around two thirds of the population being exposed to such an event at some point in their life [4–6]. Most of those exposed will not go on to develop long term psychopathology; the lifetime prevalence of PTSD in the general community has been estimated to be around 7% [7]. Around half of those who develop PTSD will recover within a year without professional help but, unfortunately, up to 15% of people with the disorder will show little or no improvement even after receiving treatment [8].
Given the relative frequency of treatment non-response, and the pervasive effect of the disorder on sufferers’ lives, preventing PTSD would be of great benefit in reducing the burden to both to society and individuals. At this stage there has not been a drug developed specifically to prevent PTSD. Instead, the prophylactic potential of medications already in existence which affect the neurotransmitters thought to be involved in the development of PTSD has been considered. While a number of such medications have been hypothesized to be potentially useful in preventing PTSD [9], we will consider here only those with some empirical support.
Alcohol
Of all the available drugs with the potential to prevent what we now call PTSD, alcohol has perhaps the longest history. For centuries soldiers have consumed alcohol before battle in an effort to reduce the stress of the experience [10,11]. More recently, naturalistic studies with fire [11] and motor vehicle accident [12] victims have found that intoxication at the time of trauma decreases the likelihood of subsequently developing PTSD. The protective effect of alcohol may be due to interference with the encoding and storage of memories [11,12]. Alcohol may also impair perception of relevant threat information, such that the event is not seen as severe or life threatening and is therefore less likely to lead to PTSD [13,14].
Alcohol may be desirable as a prophylactic medication for PTSD for several reasons. It is relatively cheap, readily available and, of particular importance in military populations, is socially acceptable. Despite these advantages, however, alcohol is unlikely to be widely endorsed as the drug of choice for preventing PTSD. It seems that alcohol protects against stress only if consumed before a stressful experience [13,14]. Naturally, regular consumption of alcohol as a preventative strategy in case a trauma is experienced is ill advised [15]. Prophylactic use of alcohol would, therefore, be restricted to those individuals who are fairly certain that a traumatic experience is imminent, such as members of the emergency services or military. However, these individuals require their judgement to be intact and their psychomotor resources to be unimpaired. The impact of alcohol on speed of information processing, risk taking behaviour and physical coordination render its routine use as a prophylactic inappropriate. In addition, there is some evidence that the stress response is less likely to be inhibited by alcohol when the stressful event is expected [14]. Finally, it is unclear exactly how much alcohol is required to be effective in preventing PTSD [15], although there is some evidence that moderate to high level use is necessary [14]. Given that alcohol use disorders are in the top five leading causes of disability world-wide [16], the risks of increasing alcohol intake in an effort to prevent PTSD would seem to far outweigh the benefits.
Cortisol
Following activation of the sympathetic nervous system in times of stress, the production of cortisol serves to shut down the stress response [15,17]. In individuals who go on to develop PTSD, however, there is some evidence that this system of regulation fails and peri-traumatic cortisol levels are lower than in individuals who recover [18] or develop other disorders such as depression [19].
With low levels of cortisol presenting an increased risk for PTSD, it follows that artificially increasing cortisol levels would provide some protection against the development of the disorder. Indeed, randomized controlled trials with survivors of septic shock [20] and cardiac surgery [21,22] have shown that patients administered hydrocortisone in the intensive care unit were less likely to develop PTSD than those who received a placebo. Whether these results generalize to other trauma populations is, as yet, unknown.
Morphine
When faced with a traumatic event, the brain increases its production of norepinephrine, which is thought to cause enhanced consolidation of new memories [23,24]. This mechanism is thought to have evolved to ensure we remember potentially dangerous events differently to those that are less threatening [9]. The extreme physiological arousal associated with trauma, however, often leads to over-consolidation of the trauma memory, and it is this over-consolidation which is presumed to lead to PTSD [25,26].
The protective effect of morphine comes from its inhibition of norepinephrine release [15,24]. In a study of motor vehicle accident survivors, it was observed that patients who went on to develop PTSD had been given lower doses of morphine in the 48 h following their accident than those who were PTSD free at three month follow up [24]. Acute morphine administration has also been associated with a lower likelihood of subsequent PTSD in US military personnel serving in Iraq [27] and there is some evidence of its effectiveness in pediatric burn patients [28,29], although this relationship may be mediated by separation anxiety [30]. In short, while in theory acute administration of morphine to prevent PTSD makes sense, further empirical investigation is needed.
Propranolol
Developed in the 1950s and used in the treatment of hypertension and heart problems, propranolol has shown promise in the prevention of PTSD by blocking the reuptake of norepinephrine. Although propranolol has perhaps received the most attention in the literature, the evidence for its effectiveness in preventing PTSD remains equivocal.
Results of a non-randomized trial showed that trauma patients who refused propranolol were significantly more likely to suffer PTSD than those who took the drug [31]. On the other hand, propranolol did not appear to effectively prevent PTSD in burned veterans [32], although a number of confounding variables make the results of that study difficult to interpret. In a small randomized controlled trial conducted by Stein et al. [33], injury patients were assessed at hospital intake and 1, 4, and 8 months later. The authors found that the severity of PTSD symptoms declined over time in both placebo and propranolol patients, with no significant difference between the two groups. Pitman and colleagues [23] conducted a similar study and found no discernable difference in rates or severity of PTSD between propranolol and placebo patients at either 1 or 3 months after admittance to a hospital emergency department following a traumatic event. However, in addition to clinical assessment, Pitman et al. [23] also measured physiological arousal at 3 months after trauma. They found that those in the propranolol group were significantly less likely to demonstrate physiological arousal patterns consistent with those seen in PTSD. Pitman et al.'s positive findings on psychophysiological measures of arousal but not on overall measures of PTSD may in part be explained by the heterogeneity of PTSD symptoms. While re-experiencing, active avoidance, hypervigilance, and startle are more likely associated with fear-circuitry, the general passive avoidance and numbing symptoms may be less directly associated with these pathways and hence less responsive to interventions focused on norepinephrine re-uptake [34].
In summary, while there are several promising options, there is currently no compelling evidence that any of the drugs above can effectively prevent PTSD.
Pathological and normal reactions
Importantly, the goal of chemoprophylaxis is to prevent pathological responses to trauma, not to eliminate normal psychological reactions. While the majority of individuals who experience a traumatic event will display some early distress, most will recover on their own within two or three weeks with only a minority going on to develop PTSD [4, 6]. Thus, widespread prophylaxis would be, at best, a costly waste of time for the majority of the traumatized population, and may even have a detrimental effect on recovery for more resilient individuals, for whom the arousal associated with trauma serves to facilitate memory processing. Drugs which reduce arousal could therefore be hypothesized to interfere with the normal consolidation and integration of the trauma memory [26].
Unfortunately, previous authors have often overlooked the distinction between normal and pathological responses to trauma and have discussed the perils of chemoprophylaxis in the context of the former [35]. It is reasonable to argue that attenuating such feelings as embarrassment [25,36], loss after a friend's betrayal [37] or disappointment on missing out on a job opportunity [38] is inadvisable and the risks are likely to outweigh any potential benefits. The debilitating effects of severe PTSD, on the other hand, should be prevented if at all possible.
Timing of chemoprophylaxis
If future research supports current thinking that certain medications can indeed prevent the development of PTSD, the question is when to administer a drug for maximum effectiveness. That is, should it be given before or after exposure to a potentially traumatic event?
Pre-exposure administration
Presumably, drugs administered prior to exposure would be given non-selectively to the whole traumatized population with the aim of moderating, for example, levels of arousal or acquisition of traumatic memories during the event. As others have noted, this has potentially critical implications for cognitive processes during the trauma and the person's ability to make appropriate moral judgements [25,39]. In other words, administering drugs prior to exposure may interfere with the individual's perception of, and response to, risks to the personal safety of themselves or others. In such a scenario, any benefits in terms of preventing subsequent psychopathology may be outweighed by the increased danger for the individual and those around him or her.
There exists some empirical evidence to support this concern. As mentioned earlier in this paper, alcohol is known to impair many cognitive processes likely to be required during a traumatic event, and it is not unique in this regard. Administration of propranolol prior to decision-making tasks, for example, has been found to result in a conservative bias in conditions of uncertainty [40], and to decrease sensitivity to punishment cues [41]. As Craigie [39] notes, relatively small doses of propranolol were used in these two studies. Since much larger doses may be required to prevent PTSD, the effect on decision making may similarly be much greater.
Further complicating this situation is the need to administer prophylactic medications quite close to the occurrence of the traumatic event. As such, any attempt to ‘vaccinate’ the general population against PTSD would currently be at best an unnecessary expense and at worse a dangerous misuse of a potent drug. The vast majority of individuals would not experience a traumatic event within the time frame in which chemoprophylaxis would be effective. Therefore, pre-exposure administration would need to target individuals for whom exposure to a traumatic event is likely to be imminent, such as military personnel and emergency service workers. As Hall and Carter [42] state:
[Those] at risk…should not be denied prophylaxis against PTSD when undertaking difficult and often gruesome tasks such as recovering bodies. If it is reasonable to ask these individuals to engage in life threatening and emotionally distressing activities, then it would be wrong to deny them access to medications that may reduce their considerable risk of PTSD. (p. 24)
On the other hand, those individuals who can be reasonably sure they will soon experience a potentially traumatic event are also those who are likely to require their judgement to be intact. Until it is shown conclusively that the prophylactic drugs currently available have no effect on cognitive, moral, or other capacities, we suggest that pre-exposure administration may be best avoided. The risks outweigh the (currently questionable) benefits.
Administration post-exposure
Providing prophylactic medication immediately following trauma exposure is also fraught with difficulty. Neuroimaging studies have shown that new memories are stored in around 6 h [9], although this is the subject of much debate. Morphine has been reported to protect against the development of PTSD where administration occurs within the first 48 h of traumatic injury [24], while trials of propranolol have shown the drug to impair memory when administered up to 24 h after a learning task [15]. Further research is needed to determine the optimal window for administration of prophylactic medications.
Due to the potentially adverse effects of chemoprophylaxis for individuals who would recover naturally [26], it seems inappropriate to offer all patients preventative treatment. Rather, targeting only those at risk of developing PTSD is likely to be a more effective strategy. Several risk factors for PTSD have been identified including pre-trauma factors (such as prior trauma and psychiatric history), characteristics of the event (such as perceived life threat and peri-traumatic dissociation), and post-trauma factors such as social support, other life stress, and pain [43–45]. As mentioned earlier, low levels of cortisol immediately after a traumatic event have been found to be predictive of PTSD [17]. Another promising finding is that individuals who go on to develop the disorder often have an increased heart rate in the acute post-trauma phase compared to those who recover [46,47]. As patient heart rate is monitored in emergency departments as a matter of course, this method of predicting PTSD may be more acceptable to the health professionals involved in acute care of trauma patients and is a line of enquiry worth pursuing. Using one or more of these approaches singly or in consultation would assist in targeting individuals for post-exposure chemoprophylaxis. Indeed, there is promising evidence that brief screening measures may do a reasonable job of predicting subsequent adjustment [48]. However, even when combined, known predictors of PTSD account for only a minority of the total variability of response to traumatic stress [44], and the potential for inaccurate predictions, particularly of the false negative variety, to some degree cautions against the use of chemoprophylaxis until more reliable predictors are known.
Ongoing trauma
For many individuals, trauma exposure will not be an isolated incident. In the case of domestic violence or war zone exposure for military personnel or civilians in war-torn nations for example, the question of when to administer preventative medications becomes far more complex. It is generally accepted that early psychological interventions are ineffective in situations where the trauma is ongoing [26], and it is difficult to imagine pharmacological intervention being any different. The difficulties of providing a drug immediately before or after a traumatic event when the person is exposed to multiple events are clear. Given the greater likelihood of developing PTSD when exposed to ongoing trauma [49], this is an issue of great importance for future chemoprophylaxis research to address.
Legal ramifications
Much of the argument against chemoprophylaxis for PTSD seems to stem from a concern that it would result in the individual feeling no emotion over the traumatic event. Authors ascribing to this view fear that routine use of prophylactic drugs after traumatic events would lead to the disappearance of distress following traumatic events. The events would still occur, but no one would be particularly bothered by them.
Studies trialling the use of prophylactic medications, however, have not provided evidence that their administration prevents an individual from feeling any emotion about a particular event. Following administration of cortisol or propranolol, study participants report negative stimuli to be less arousing than their placebo counterparts. Such stimuli were, however, still rated as being negative. Receiving either of the drugs prior to exposure did not cause participants to interpret negative stimuli as neutral or positive [50,51]. As far as we are aware, no studies have investigated the degree to which other potential prophylactic drugs such as morphine moderate the perception of emotional stimuli.
Concerns over the blunting of emotions by chemoprophylaxis are most often raised in relation to the legal proceedings that can arise from traumatic events such as rape and motor vehicle accidents. It has been suggested that a witness or victim who uses medication acutely to dull the pain of a traumatic event would also experience an impact on memory, and that for justice to be done, memories must be preserved [36]. However, eyewitness testimony at the best of times is far from infallible, and more concrete evidence that a crime has been committed is generally required for a conviction. Further, guilty verdicts should never hinge on whether or not the victim or witness develops PTSD [42].
It has also been suggested that the blunted affect of a rape victim who was administered prophylactic medication in the emergency room may lead a jury to find the person's testimony unconvincing, thus weakening the case against the perpetrator in court [52]. In discussing the pros and cons of chemoprophylaxis in the context of providing such testimony, it must once again be remembered that the purpose of this intervention is to prevent PTSD. Had the person been suffering this debilitating disorder, the rape victim's ability to provide valuable testimony may have been further impaired.
While issues relating to the effect of chemoprophylaxis on eyewitness testimony are worth considering, they do not pose an insurmountable problem. Expert witnesses, for example, can explain to the court the reasons for, and effects of, chemoprophylaxis. Given the above findings, while ramifications in criminal cases will continue to present some challenges, apprehension over chemoprophylaxis based on the potential for emotional blunting should not be exaggerated.
Civil cases, particularly those in which compensation is involved, have slightly different implications for chemoprophylaxis. Such cases often depend heavily on the presence of a diagnosis such as PTSD and the plaintiff's claim would be weakened if he or she did not meet criteria. Assuming that the chemoprophylaxis was successful, it would be hard to argue that the victim would have developed PTSD in the absence of such prophylactic medication. Indeed, of course, one would hope that the absence of long-term psychiatric disability would negate the need for the civil proceedings in the first place.
In summary, there are several potential legal ramifications raised by the issue of chemoprophylaxis in the field of traumatic stress. No doubt they will be the subject of discussions by expert witnesses and will continue to present challenges for the legal fraternity. These issues, however, are not insurmountable and are most definitely not an argument for not adopting these preventive measures if they are demonstrably effective. Our first priority, without question, must be the emotional health and well-being of people exposed to trauma.
Obstacles to chemoprophylaxis
There are a number of obstacles to the widespread use of prophylactic drugs which require further consideration. In the acute phase following trauma, patient reluctance and informed consent are potentially huge barriers to chemoprophylaxis. Trauma patients are often understandably more concerned with their physical pain, and focusing their attention on the possible mental health sequelae of their experience can be difficult [9,33]. Even more difficult, informed consent must be gained. This may be an almost insurmountable task for some patients; aside from the obvious problem of unconsciousness, physical injuries and loss of loved ones may understandably prevent them from comprehending the complex nature of memory altering. Issues that may need to be discussed include the uncertainty of PTSD predictions, the potential implications for aiding criminal trials, and potential detriments to post-traumatic growth [33,52]. At present there is little information about these issues in the empirical literature. Qualitative research with PTSD sufferers and patients who receive preventative medications in the acute aftermath of trauma may provide answers to some of these questions.
If the data on prophylactic medications were stronger, it could be argued that informed consent would not be required. In the same way that medications or procedures are decided for unconscious or otherwise incapacitated patients, chemoprophylaxis would become a question of judgement for the treating physician.
Of course, drugs with the potential to prevent PTSD are not suitable for everyone. As with any medication, the potential benefits must be weighed against the risk of side effects, and contraindications including a history of substance abuse (morphine), asthma (propranolol), or penetrative injuries (hydrocortisone) must be taken into account [9,53]. Further, PTSD is commonly comorbid with other disorders such as depression and alcohol abuse. At this stage it is unclear what effect these preventative medications have on other post-traumatic mental health conditions.
One of the most problematic barriers to chemoprophylaxis, though, is that following a traumatic experience, many people simply do not come to the attention of the relevant authorities in the short time frame available. All empirical research to date has investigated the effect of prophylactic medications on hospital patients and for good reason; individuals who sustain major physical injuries during a traumatic event are rare in being identifiable in the immediate aftermath of their experience. Thus, although it may be possible to prevent PTSD and other mental health sequelae of trauma in this population, it is unclear whether chemoprophylaxis will ever be of use for survivors of other horrific events who do not require urgent medical attention. In the meantime, it may be wise to focus our attention on preventing PTSD in high risk populations such as the military and emergency services.
Conclusions
In the past few years attention on chemoprophylaxis for post-traumatic stress disorder has greatly increased. Unfortunately, the unfounded fears comprising much of the literature to date have done little to further the field. When considering chemoprophylaxis, two fundamental concepts must be kept in mind. Firstly, that chemoprophylaxis refers not to the treatment but to the prevention of PTSD. Secondly, that the goal of chemoprophylaxis is not to interfere with normal recovery. Aligning future discussion with these concepts will assist in improving both the empirical and philosophical literature in this field.
The small randomized controlled trials conducted to date have not provided unequivocal evidence of the benefits of chemoprophylaxis, although some results, particularly in regard to hydrocortisone, are promising. This may in part be an issue of power; the biggest RCTs to date have involved less than 50 participants. Larger trials are therefore needed to further investigate the efficacy of potential medications such as propranolol, hydrocortisone, and morphine. In addition, further work must be undertaken in order to establish concrete predictors of PTSD. With the small window of opportunity for administration of prophylactic drugs, we must be able to predict the development of the disorder with much greater accuracy than we currently do before chemoprophylaxis moves from the research domain into the real world.
Footnotes
Acknowledgements