
Abstract

We refer to the study by Lewis et al. [1] showing babies of mothers exposed to antidepressants whilst pregnant were at increased risk of prematurity and lower birthweight as well as being smaller in length and head circumference. While the study adds to the growing body of literature on the complexity of managing depressed pregnant women, several issues need clarification. Firstly, it is stated that the control group were matched, but not what factors they were matched on. Of particular note is that controls could not be matched on the non-pathological determinants of foetal growth, such as parental height and build since these were not recorded. Secondly, the women on antidepressants were severely depressed, but there is no mention that the control group were depressed at all. It therefore remains unclear whether the difference in gestational age and birthweight can be attributed to the antidepressant or the underlying condition, Thirdly, the mean gestation at birth in the exposed group was 38.86 weeks which is only 1 week less than the mean gestation for the control group, and well within what is considered ‘term’. The mean birthweight of the control group was 3671.19 g, which appears rather large. A comparison with the Victorian Perinatal Data Collection [2], showing the average birthweight of male babies in 2004 was 3419 g and of female babies was 3302 g, indicates that birthweight for this control group may be slightly skewed, particularly since it consisted predominantly of females (17 females: 9 males). The issue of low numbers was highlighted in the study.
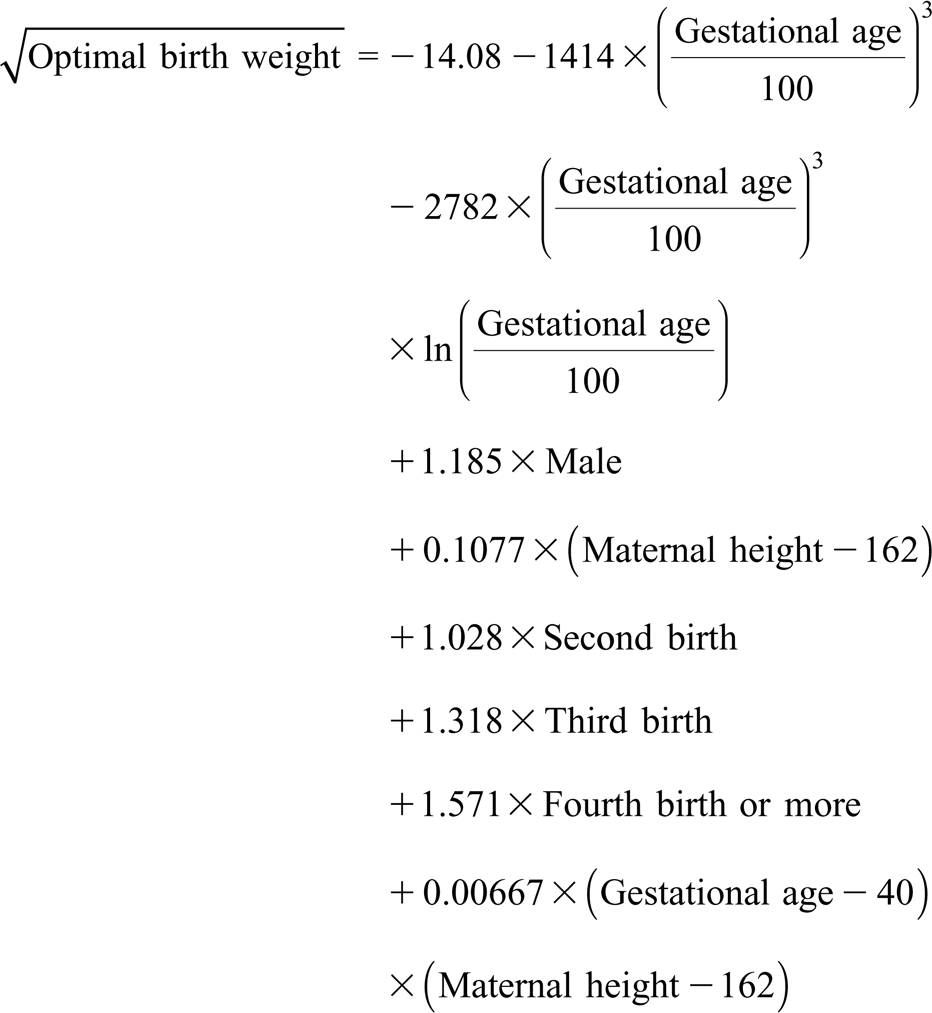
Since the average weight gain between 38 and 39 weeks is about 200 g, (growth for gestational age charts), the 400 g difference in mean birthweight shown in the study does suggest a slower rate of growth. We suggest however, that it would be more convincing to look at individual patient data with a properly calculated proportion of optimal birthweight (POBW), using the formula developed by Blair et al. [3], which also takes into account other variables including gestation:
It should be noted that equations for optimal foetal dimensions were estimated from a population without any growth restricting pathology including exposure to cigarette smoke. Average foetal dimensions for a given set of non-pathological determinants tend to be below optimal. The fact that the control group consistently show proportions greater than 1 despite including a proportion of smokers suggests that they may be systematically exposed to growth accelerating factors such as greater parental size or metabolic syndrome. Accurate interpretation of this study requires more information about the characteristics of the control group and how they compare clinically with those of the treatment group.
Taken in these contexts, the result of the study may show a relative discrepancy in some growth variables of the exposed group versus control; however, the absolute values may well be within normal limits. It remains to be seen whether these discrepancies will translate into clinically significant long-term developmental outcomes for the child.