
Abstract
The period of emerging adulthood (18–25) is a key transition point in the life cycle [1]. One dynamic that may compromise adult functioning is childhood and adolescent antisocial behaviour. Antisocial behaviour is common in Australia, with population surveys reporting that up to 5% of young people exhibit significant aggression, and 7% exhibit significant delinquent behaviour [2]. Additionally, young people are over-represented in official crime statistics [3]. Antisocial behaviour in childhood or adolescence is linked with a range of adverse outcomes in adulthood [4,5]. Domains affected include unemployment [6], mental health problems [7], greater rates of adversity [8], more problems with educational attainment, substance use and interpersonal relationships [8,9] and greater risk of mortality [10]. There is an array of potential mechanisms linking early antisocial behaviour and later adult outcomes. Genetic or early life factors may contribute to risk of both aggression and impaired adult functioning [11,12]. Additionally, the relationship between childhood aggression and adult outcomes may be mediated by psychosocial factors such as peer influence or disruption to education [8,13].
A variety of conceptual perspectives exists from which to understand the relationship between early antisocial behaviour and adult outcomes. Some studies examine behaviours in specific time periods such as tantrums at three years [14], or aggression in early adolescence [15]. The Australian Temperament Study found that a persistently antisocial adolescent group, compared to transient antisocial or non-deviant peers, had more trouble finishing high school, higher rates of substance abuse and exhibited poorer adjustment in interpersonal relationships during emerging adulthood [9]. Another model classifies young people based on both the presence of problem behaviour at key developmental stages and continuity across stages. Developed by Moffitt [16,17], this typology comprises three key groups: (i) childhood limited (CL), previously referred to as ‘recoveries’[17] refers to those who exhibit significant antisocial or externalizing problems in childhood but do not exhibit serious antisocial problems in adolescence; (ii) adolescent limited (AL) refers to those who exhibit serious antisocial problems in adolescence but not earlier in childhood (also referred to as adolescent onset); and (iii) life course persistent (LCP), which describes individuals who exhibit serious antisocial or related problems throughout both childhood and adolescence. The model predicts that the LCP group will exhibit the worst outcomes across varied domains, the AL group will age out of their antisocial behaviour in early adulthood, and the CL group will exhibit some antisocial behaviour in adulthood, but not as extreme as the LCP group [17].
Traditionally, males have been over-represented in official crime statistics of western countries. However, research indicates that the gender gap in criminal and antisocial behaviour is narrowing, with an increasing presence of women in official crime statistics [18,19]. Within this context an important question is whether early antisocial behaviour in girls is associated with adverse outcomes similar to those observed in antisocial males. It has been suggested that antisocial girls will have fewer problems in adulthood than males, due to societal pressures to conform [20,21]. In contrast, is has also been argued that females face worse outcomes than males, due to co-occurrence of psychological disorders and stigma of offending behaviour in women [22]. Other researchers suggest that both male and female antisocial adolescents will exhibit similar adverse outcomes, due to similarity of causal factors influencing offending behaviour [23].
Extant research is not able to resolve this issue. The Dunedin Longitudinal Study [24] reported that at 21 years, AL males and females exhibited a similar range of adverse outcomes [12]. Examining outcomes for LCP females was limited by the small number of girls (six) classified as LCP [25]. As such, most extant research examining outcomes for antisocial behaviour focuses on males (e.g. Moffitt et al. [26]), and little data is available to inform our understanding of female outcomes. To address this gap, the current study examines whether early antisocial behaviour in girls is associated with similar adverse adult outcomes as antisocial behaviour in boys, especially for high prevalence outcomes such as binge drinking, cannabis use, general health, mental health symptoms and indicators of antisocial behaviour. We hypothesize that antisocial behaviour in females would be associated with increased risk of a range of adverse adult outcomes, similar to patterns observed in males.
Method
Study sample
Data for this study have been taken from the Mater–University of Queensland Study of Pregnancy (MUSP), a 21-year longitudinal study initiated in 1981. Pregnant women attending their first clinic visit (at approximately 18 weeks gestation) at the Mater Misericordiae Mothers’ Hospital (Brisbane, Australia) were invited to participate in the study [27,28]. Written informed consent from the mother was obtained at all data collection phases and from the young adult at the 21-year follow up of the study. Ethics committees at the Mater Hospital and the University of Queensland approved each phase of the study.
Between 1981 and 1984, 8556 consecutive pregnant women were invited to join the study and 8458 agreed to participate (phase 1). Of these, 7223 gave birth to a live singleton infant and it is this group of mothers and offspring that constitutes the MUSP birth cohort sample. Of these mothers, 5259 (73%) provided data for their child at 5 years, and 5185 mothers (72%) provided data at 14 years. At 21 years, complete data across the study was available for 3173 young people. Detailed information about the study has been published elsewhere [28].
To examine the possible effects of sample attrition over the follow ups on the validity of the conclusions, complementary tests were conducted to assess the association between child and adolescent antisocial behaviour, and a selected group of family backgrounds with sample losses up to the 21-year follow up. To estimate the effects of attrition in a particular instance, logistic regression analyses were conducted to identify the factors related to the probability of missing data (both loss to follow up and missing data in the followed up analysis sample). Using the inverse probability weighting method [29], previous reports on the MUSP data have demonstrated that loss to follow up did not affect the findings [30,31]. Detailed mathematical modelling with the aim of predicting bias in relative risk estimates in this cohort suggests that any effects of loss to follow up would mean that the results presented here are an underestimate rather than over estimate of the true effects [28].
Classification of antisocial behaviour
Antisocial behaviour at the 5-year follow up was assessed using a short form (33 items) of the Child Behaviour Checklist (CBCL) [32]. The short form was used due to resource constraints at the 5-year follow up. Prior analyses using a sub-sample of respondents indicates a strong correlation (r = 0.94) between the short (10 items) and long forms of the CBCL for the externalizing behaviour sub-scale [32]. The CBCL rates behaviour for the 6 months prior to interview. The mean score for externalizing behaviour at 5 years was 5.97 (6.25 for males and 5.71 for females) out of a possible maximum of 20.
Antisocial behaviour at 14-year follow up was assessed using the Youth Self Report of the CBCL (YSR) [33,34]. The YSR was designed for individuals aged 11–18 years and contains 102 items assessing problem behaviour (for 6 months prior to interview) including aggressive and delinquent problems (antisocial behaviour). The reliability and validity of the YSR has been supported by research [35].
Using the measures of antisocial behaviour at ages 5 and 14, we identified children who exhibited elevated aggression at each time point (defined as greater than one standard deviation above the mean) and then allocated them into one of the following groups:
Childhood limited: antisocial behaviour at 5 years, but not at 14 years (12%);
Adolescence onset: antisocial behaviour at 14 years but not at 5 years (11%);
Life course persistent: antisocial at both 5 and 14 years (3.7%);
Unclassified (UNCL): Below the cut-point for antisocial behaviour at both 5 and 14 years (73.3%).
The initial chi-square analysis shows statistically significant differences in the proportion of males and females in the typological groupings (see Table 1). Of the subjects, 3173 had complete data from early childhood to 21-year follow up.
Typological grouping of child and adolescent antisocial behaviour
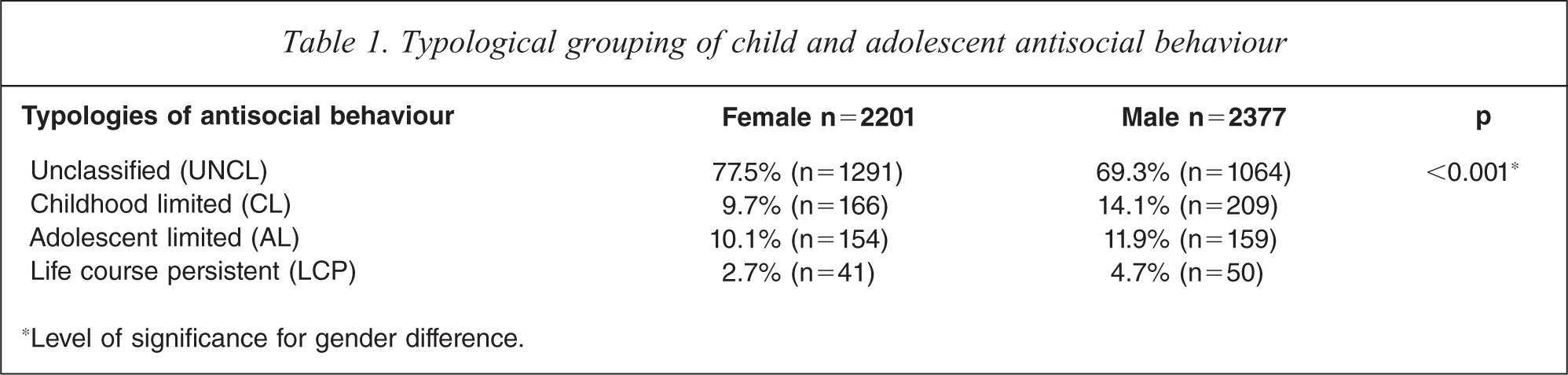
∗Level of significance for gender difference.
Assessment at 21 years
Outcomes assessed at 21 years included ongoing antisocial behaviour, substance use, mental health and general health. In the case of mental health and substance use, high prevalence symptoms and drug use behaviours were used as outcomes rather than formal diagnoses, as subsyndromal mental health symptoms and non-dependent drug use are associated with significant functional impairment [36–39]. The following outcomes were assessed at 21 years:
Young adult antisocial behaviour was measured using the antisocial behaviour subscale of the Young Adult Self-Report (YASR) version of the CBCL [40]. Antisocial scores exceeding one standard deviation above the mean were considered to represent ‘caseness’.
Offending behaviours: participants were asked whether they had committed any of the listed offences in the previous twelve months. Questions asked about (yes/no response): shoplifting, stealing things or parts from a car or motorbike, breaking into a house or building to steal things, deliberately hurting somebody, and forcing someone to have sex. A positive response to any item classified young adults as offenders (10.5% of participants).
Court attendance: participants were asked whether they had to go to court for something they did (rated dichotomously yes/no; 16.1% reported court attendance).
Cigarette smoking: based on average number of cigarettes smoked per day during the previous week, participants were divided into three categories: non-smokers, less than 10 cigarettes per day, and 10 or more cigarettes per day.
Binge drinking: participants were asked how many standard drinks they consumed on a typical drinking occasion (grouped as more than six drinks per drinking episodes, between one and six drinks per drinking episode, and non-drinkers).
Cannabis consumption: participants were asked how often in the last month had they used cannabis, marijuana, pot, etc. Options included: have never used, used every day, use it every few days, used it once or so and not used it in last month. Participants were grouped as: never used, occasional users (including ‘once or so’ and ‘not in the last month’), and frequent users (including ‘every day’ and ‘every few days’).
General health problems: participants they were asked whether they had been told by a doctor that they had a range of physical or mental health problems. According to the number of problems, individuals were divided into three groups: no problems at all, one to three problems, and four or more problems.
Anxiety and depressive symptoms were assessed using the YASR anxiety/depression subscale. Scores exceeding one standard deviation above the mean were considered to represent ‘caseness’.
Delusional symptoms were assessed using the 21 item Peters Delusion Inventory (PDI-21) [41], which measures delusional ideation in a normal population [41]. Questions are derived from the Present State Examination [42], but are rephrased and aimed at exploring a life-time experience, using the expression ‘do you ever feel as if…’. The internal consistency, concurrent validity, and criterion validity of the PDI-21 has been established [41]. The number of positive answers are summed to create a total score (0–21). Individuals were divided into three categories: 0–3 items (38.1%); 4–10 items (52.7%); and 11 or more items (9.2%).
Data analysis
Statistical analysis utilized a series of logistic regressions, conducted separately for males and females. For all analyses the key predictor variable was antisocial behaviour group (CL, AO, LCP and Unclassified as the reference group). The key outcome variables assessed were antisocial behaviour, substance use, mental health and health problems, as discussed above. For each model, the relationship between antisocial grouping and outcome was assessed using odds ratios (OR) with 95% confidence intervals (CIs). Further details about regression outcomes are available on request. The criterion for statistical significance was set at p < 0.05 and all analyses were carried out using SPSS version 15.
Results
Antisocial behaviour, offending and court attendance
CL antisocial behaviour was not associated with adult self-reported antisocial behaviour in males or females. In contrast, males and females in both AO and LCP groups exhibited higher risk of antisocial behaviour at 21 years (see Table 2).
Young adult antisocial behaviour (YASR), offending behaviour and court attendance by typological grouping (n=3134)
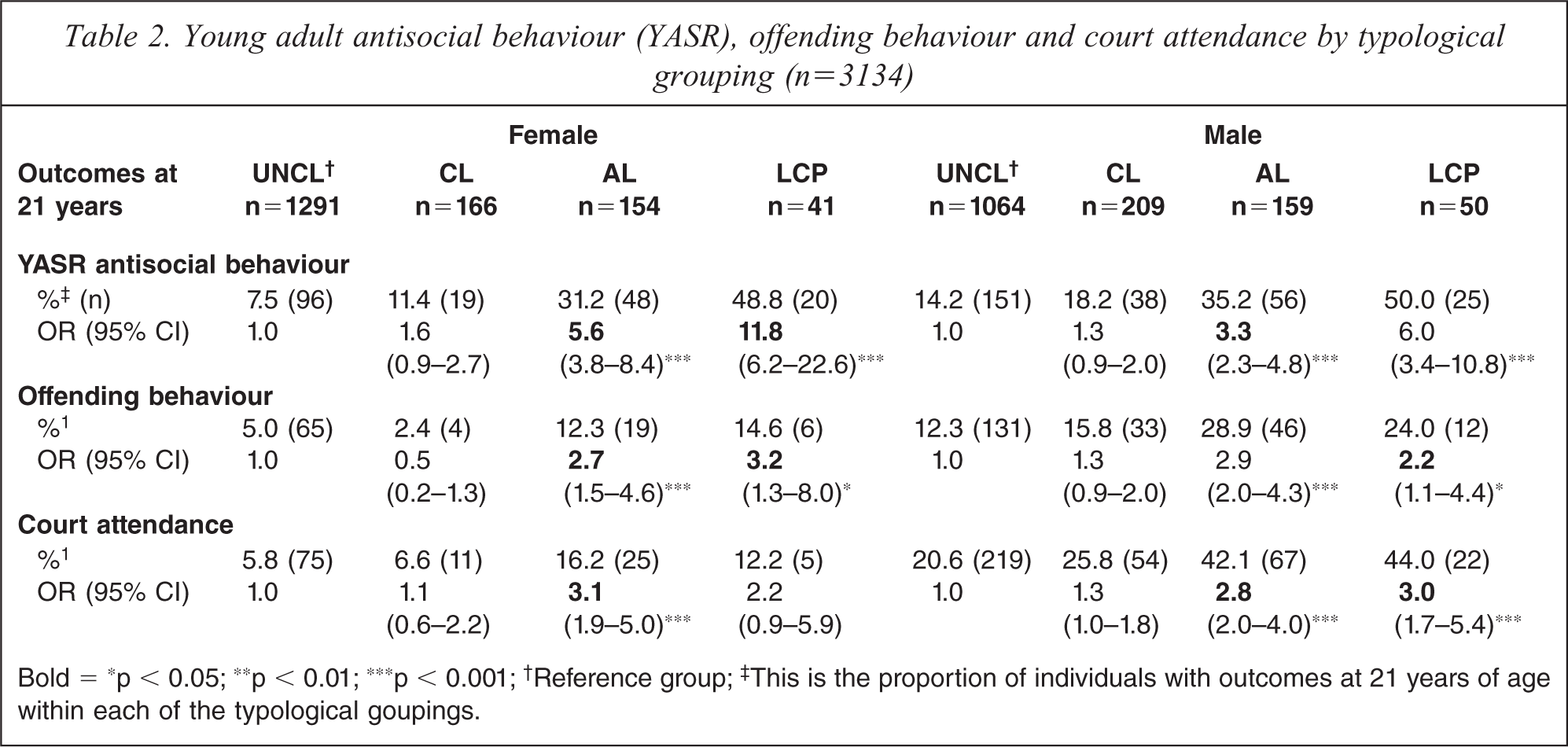
Bold = ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; †Reference group; ‡This is the proportion of individuals with outcomes at 21 years of age within each of the typological goupings.
A similar pattern of relationships can be observed when examining self-reported offending. Antisocial behaviour in childhood did not significantly predict offending in either males or females. Individuals in both the AO and LCP groups were significantly more likely to self-report offending (Table 2). When examining the females’ self-reported court attendance, only AO antisocial behaviour significantly predicted attendance. In contrast, two groups of males’ antisocial behaviour (AO, LCP) were significantly more likely to lead to court contact compared to the UNCL group.
Substance use outcomes
Cigarette smoking of less than 10 per day was predicted by only females in the AO and LCP groups (Table 3). Cigarette smoking of ten or more cigarettes per day was predicted by all three antisocial behaviour groups in males, whereas only AO and LCP antisocial behaviour predicted this level of smoking in females (Table 3). Alcohol consumption (low or high) was not predicted by antisocial behaviour for either gender (Table 3). In contrast, both AO and LCP antisocial behaviour for both genders predicted occasional cannabis use. Frequent use of cannabis at 21 years (Table 3) revealed a somewhat different pattern; AO and LCP antisocial behaviour significantly predicted elevated levels of use in males. However, in females, only AO antisocial behaviour significantly predicted frequent cannabis use.
Young adult smoking, alcohol consumption and cannabis use by typological grouping (n=3175)
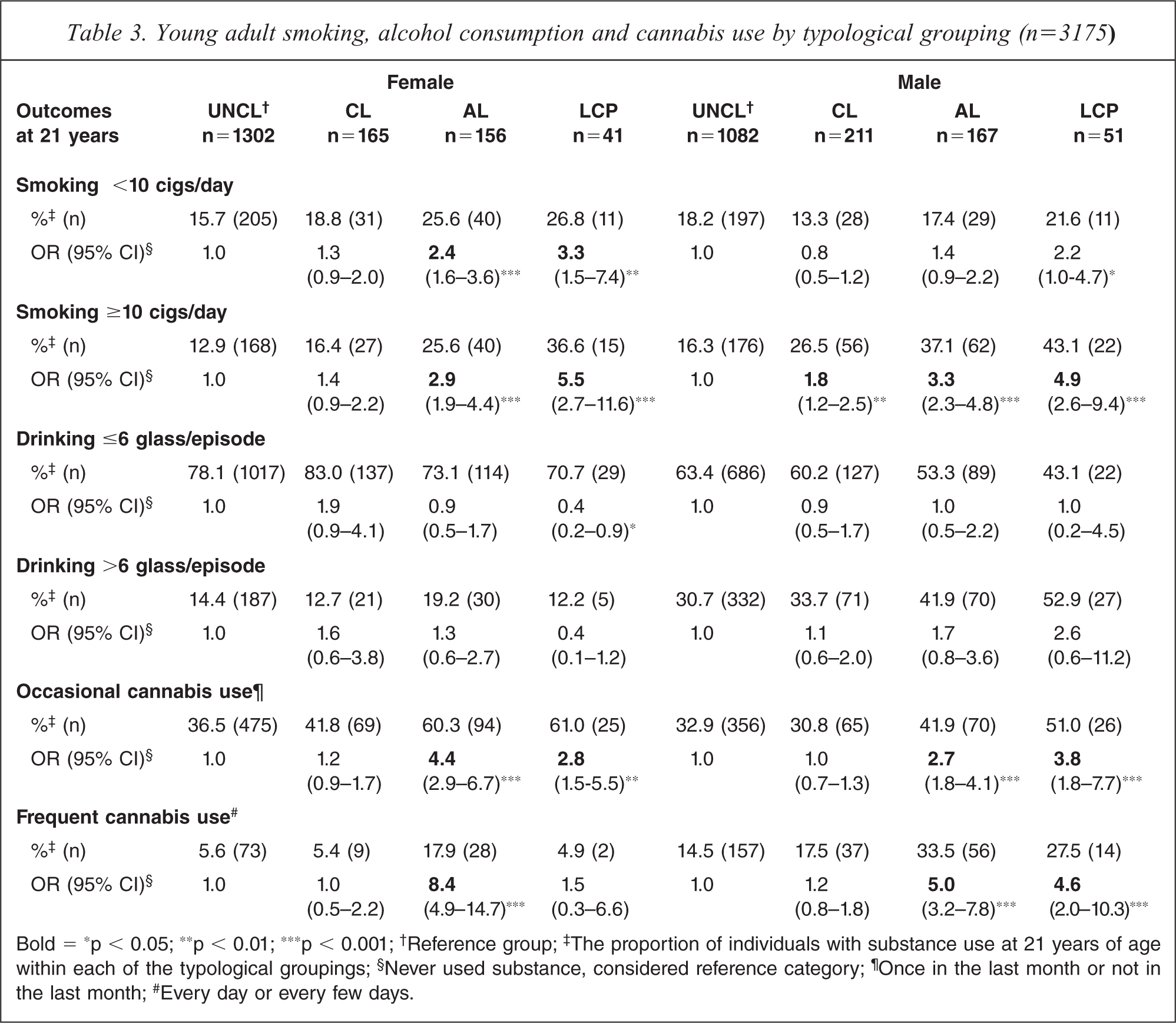
Bold = ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; †Reference group; ‡The proportion of individuals with substance use at 21 years of age within each of the typological groupings; §Never used substance, considered reference category; ¶Once in the last month or not in the last month; #Every day or every few days.
Health problems
In males, CL, AO and LCP antisocial behaviour was associated with increased odds of experiencing four or more health problems (Table 4). AO males also exhibited high risk of experiencing one to three health problems. In contrast, the only female group exhibiting increased risk of health problems was AO females, associated with higher risk of experiencing four or more health problems.
Young adult general health problems by 21 years according to typological grouping (n = 3202)
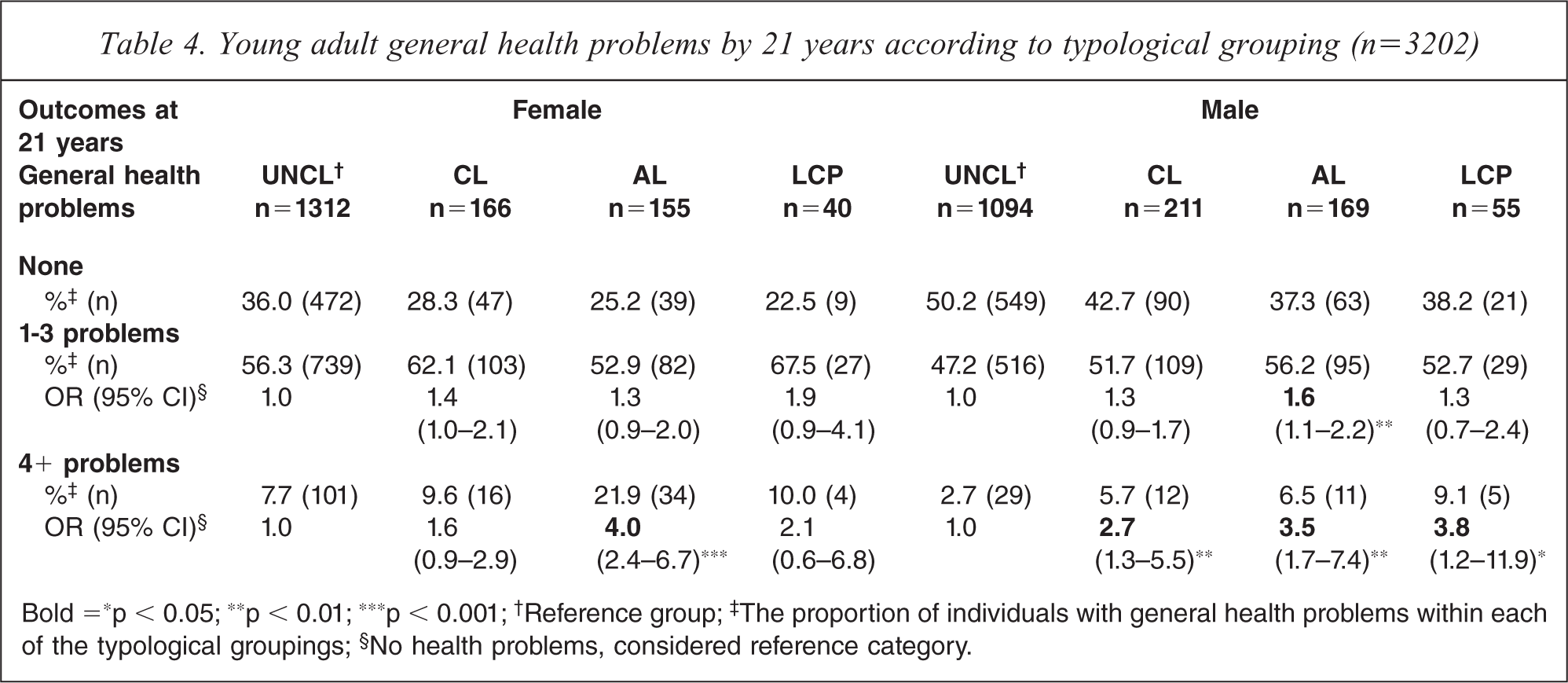
Bold =∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; †Reference group; ‡The proportion of individuals with general health problems within each of the typological groupings; §No health problems, considered reference category.
Mental health symptoms
All three groups of antisocial females were associated with elevated risk of experiencing anxiety and depressive symptoms at 21 years. In males, only AO and LCP groups exhibited elevated risk of experiencing such symptoms (Table 5).
Young adult anxiety/depression (YASR) and delusional ideation (PDI) at 21 years according to typological grouping (N=3137)
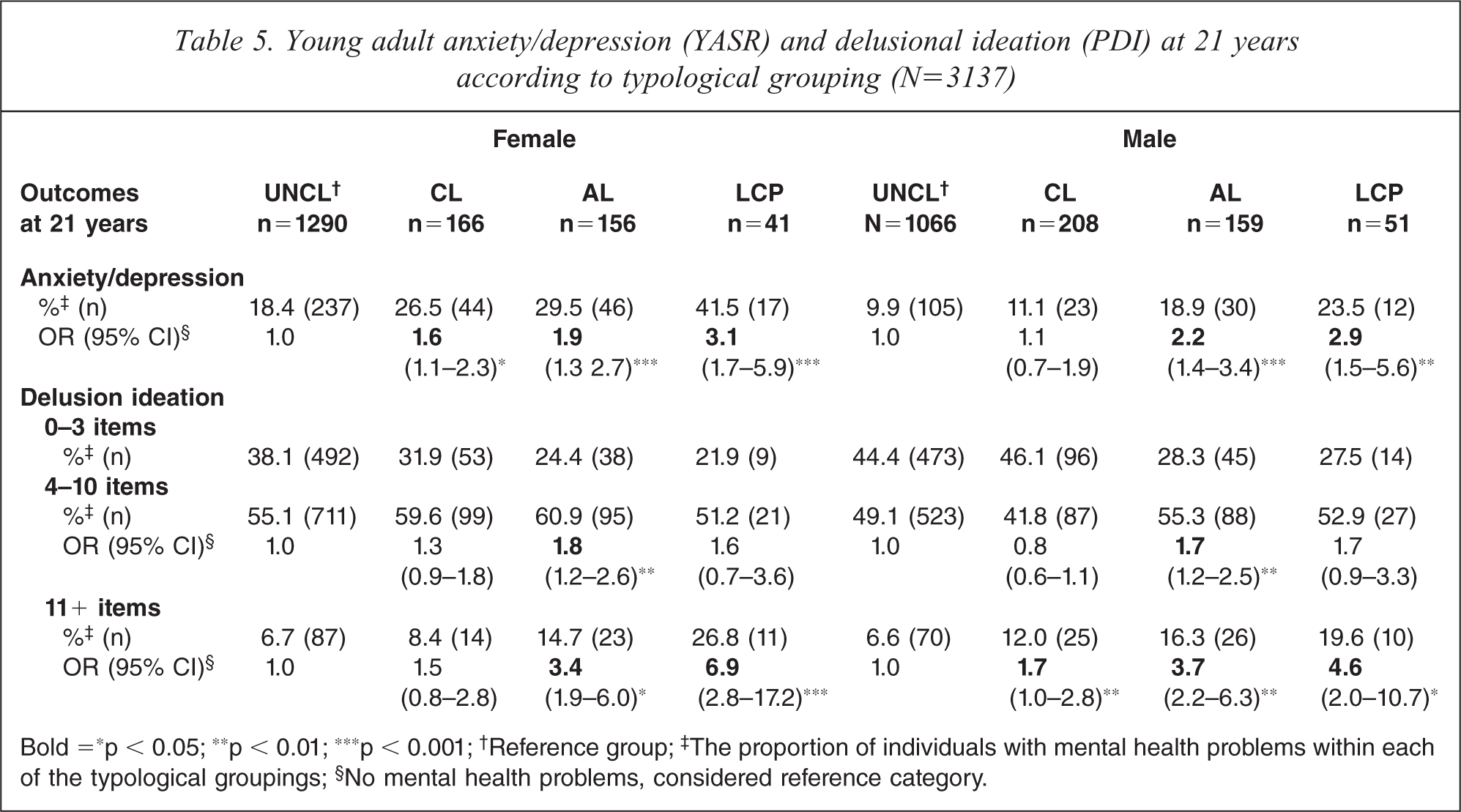
Bold =∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; †Reference group; ‡The proportion of individuals with mental health problems within each of the typological groupings; §No mental health problems, considered reference category.
In males, CL, AO, and LCP groups were associated with increased risk of delusional symptoms (11+) at 21 years. AO males also exhibited an increased risk of moderate delusional symptoms. In females, CL antisocial behaviour was not associated with delusional symptoms, whereas AO and LCP groups were associated with elevated risk of delusional symptoms (11+), and AO females also exhibited higher risk of experiencing moderate delusional symptoms (Table 5).
Discussion
Our findings demonstrate that the relationship between young people's antisocial behaviour and later adverse outcomes is not uniform, but dependent on the timing and continuity of antisocial behaviour. Although males were more likely to be classified as antisocial, both males and females exhibited elevations in risky outcomes. Specifically, young people exhibiting AO and LCP antisocial behaviour exhibited increased risk of adverse outcomes across a range of domains. In contrast, those in the CL group (both sexes) exhibit elevated risk in fewer domains.
CL males exhibited elevated risk of court attendance, health problems (minor and major) and more extreme delusional ideation. In contrast, CL females exhibited greater risk of minor health problems and symptoms of anxiety/depression. Other research has confirmed this pattern particularly in males where ‘recovery’ from early conduct problems predicts future low level offending and an isolated, poorly adjusted life style [43,44]. The finding that CL females experience internalizing symptoms in emerging adulthood whereas CL males experience delusional symptoms suggests that antisocial behaviour in childhood may manifest differently in girls and boys throughout life. Interestingly, CL antisocial behaviour was not associated with greater risk of offending behaviour or substance use in emerging adulthood. In contrast to Moffitt's suggestion that true recovery is rare [24], these findings provide some basis to reassure families that antisocial behaviour constrained to early childhood need not lead to broad negative outcomes. It is possible that young people with CL antisocial behaviour exhibited differences in outcomes in areas not measured in this study.
Problem behaviour emerging in adolescence was associated with negative outcomes in almost all domains for both males and females: antisocial behaviour, offending and court attendance, tobacco and cannabis use, and health problems. These findings are consistent with the work of Moffitt and colleagues [12,25]. Antisocial behaviour in adolescence, even with no childhood history of such behaviour, places both males and females at significant risk of poorer outcomes in emerging adulthood. This is particularly important given the high prevalence of antisocial behaviour in young people. For example, in an Australian longitudinal study, up to a third of those aged 13–14 were involved in physical fights and a quarter were drinking alcohol [45]. The relationship between adolescent antisocial behaviour and persistent antisocial behaviour in young adulthood reinforces use of the term adolescent onset rather than adolescent limited [12,46]. Odgers and colleagues [12] reported that although both AO males and females exhibited poorer outcomes in physical health and economic problems, only males exhibited greater risk of violence and mental health problems at 32 years. This suggests that longer term trajectories may differ for AO males and females.
Potential mechanisms underpinning the adverse AO trajectories are not well established. Characteristics such as impulsivity may predispose to negative sequelae in adulthood. Antisocial adolescents may delay participation in protective adult turning points such as marriage or parenthood. Alternatively, antisocial adolescents may be exposed to unemployment, substance use or the criminal justice system, which may act as ‘snares’, embedding them in long-term antisocial lifestyles [47]. Substance use has been reported to impair recovery of antisocial youths [48]. Further research is needed to clarify the causal mechanisms mediating this relationship, and whether different mechanisms operate for males and females.
Consistent with Moffitt's theory, both males and females exhibiting life course persistent antisocial behaviour reported poor outcomes across multiple domains. In contrast to LCP males, who exhibited poor outcomes across all domains except drinking behaviour, LCP women did not exhibit an increased risk of court attendance, frequent cannabis use, or health problems. The differences in court attendance are consistent with evidence suggesting females are treated more leniently by the policing systems [18]. Similar to our findings, the Dunedin study reports that LCP males exhibit stronger associations with drug dependence than LCP females [12,25]. Although rates of alcohol and cannabis use may be similar between genders [49], rates of actual drug dependence tend to be higher in males [50]. Young women attending substance use treatment services report lower rates of cannabis use than men [51]; it is possible that in our sample LCP females exhibited higher rates of other substance-related problems such as heroin use. The lack of relationship between LCP antisocial behaviour and health outcomes in females may reflect better use of health services, which might protect them from health problems. More research using objective measures of health status may help resolve these different findings. Some of these differences may reflect differences in cultural attitudes to illness, rather than health system characteristics.
A variety of potential mechanisms account for the LCP trends. The LCP type is characterized by a range of early and serious risk factors such as genetic influences, neuro-cognitive deficits, poverty and family stress [25]. A complex process of poor socialization may set up the individual for lifelong acquisition of antisocial behaviour [52]. Further research is required to identify how these risk factors may operate differently in girls compared to boys.
There has been little research exploring the mechanism of the relationship between CL antisocial behaviour and adult outcomes. Our data supported an association with health and mental health problems rather than antisocial and offending behaviour. It is possible that CL children may experience ‘snares’ such as poor social or cognitive functioning [53], peer rejection or school failure; while not promoting offending behaviour, such factors may contribute to social isolation and internalizing symptoms in later life. Further research is needed into this group to determine the risk factors associated with adult maladjustment.
Understanding the mechanisms associated with mediating the risk between antisocial behaviour groups and adult outcomes may assist in identifying strategies to improve adult outcomes in young people exhibiting antisocial behaviour. A range of effective treatments have been identified for management of aggression in young people [54]. Further research is required to understand the impact of effective treatments on adult outcomes for aggressive youth.
Limitations
One potential limitation of this study is our reliance on a range of self-report or symptom rating measures rather than objective measures or formal diagnoses. Research supports the validity of self-reported substance use [55,56] and criminal behaviour [57,58]. Official records and formal diagnoses may provide only a limited estimate of the prevalence of certain problems, whereas self-reported behaviours may provide more extensive coverage of problems, and more rigorous examination of risk trajectories. For example, subsyndromal mental health symptoms are associated with significant functional impairment [36,37] and are a common basis for presenting to health services in young adults [59]. It is important to note that onset of actual diagnoses may occur later than 21 years for many disorders [60]. Similarly, it is accepted that the majority of alcohol or cannabis users do not meet diagnostic criteria for abuse or dependence disorders [39,61], yet still exhibit elevated risk of adverse outcomes [38,39]. Future research is required to identify whether syndromal and subsyndromal psychiatric problems exhibit differential aetiological trajectories.
Our study did not control for a number of important confounders or mediating variables. Our reasoning is that we wished to replicate Moffitt's work and examine the effect of gender on adult outcomes as closely as possible. Our construction of antisocial groups only utilizes two time-points of antisocial behaviour, whereas Moffitt's typologies are created using six points across childhood and adolescence [25]. While it is possible that our AO group exhibited severe antisocial behaviour in childhood after our 5-year time point, severe aggressive behaviour rarely emerges after school entry [62].
Another limitation is the sizeable reduction in the sample between the first phase and 21-year follow up. The study experienced significant attrition with only 3173 participants having data on antisocial behaviour at 5, 14 and 21 years. In the present investigation, non-response at 21 years was predicted by levels of antisocial behaviour at 5 and 14 years (P < 0.01). Loss to follow up may influence our results in two different ways. If the associations in those lost to follow up was higher than in the study group, our findings would underestimate the true association. There is a potential threat to the validity of our findings if the association we demonstrated was not evident or was in the opposite direction in those lost to follow up. Given the likely causal pathways and the positive association reported by other authors, this is unlikely. In the MUSP, it is generally the case that those lost to follow up would be expected to have a worse outcome and it is likely that the results presented here underestimate the true associations.
Conclusion
Overall, this study has shown that typologies of antisocial behaviour have serious young adult sequelae across a range of important outcomes such as physical health, substance use, offending behaviour and mental health. Importantly, these findings demonstrate that both antisocial females and males exhibit poor outcomes in young adulthood.
Footnotes
Acknowledgements