
Abstract
Older people are probably no less likely to recover from a major depressive episode than younger adults; however, for various reasons, they are probably more at risk of a relapse [1]. The most obvious reasons are physical illness and cognitive impairment [2]. Previous episodes of depression may also sensitise the elderly to further recurrences [3]. This may be because of chronically elevated glucocorticoid levels causing hippocampal damage, leading to a further increase in corticotrophin-releasing factor, and a vicious cycle of further hippocampal damage with each episode of depression [4,5]. It is important therefore to treat depressed older people more assertively than their younger counterparts, and to ensure that they receive adequate treatment for medical co-morbidities.
Given the growing body of evidence to link the importance of psycho-social factors to healthy ageing and longevity in general [6], one would think that psychosocial factors would also play an important role in the trajectory of a psychiatric illness such as geriatric depression. In their influential meta-analysis, however, Cole and Bellavance were able to identify only nine studies that examined the influence of social factors on the prognosis of geriatric inpatient depression, and these showed essentially no relationship [2]. Factors such as marital status, living circumstances, income, social support, and the presence of an intimate, confiding relationship by and large had no effect on outcome. Other sources, however, suggest that social factors, in particular the extent of a person's social network, have a positive impact on the outcome of geriatric depression [7].
Clearly, psychosocial factors deserve closer scrutiny in this area of research. One construct that is beginning to attract attention, at least in North America, is religiousness. North Americans have high levels of religious belief and practice compared to Australians and Europeans [8,9]. A reasonable question to ask is whether their religious practices, both organised and personal, have a bearing on the course of depression. In a study of 87 medically ill older inpatients with either major depression or subsyndromal depression, Koenig and colleagues found that those with higher intrinsic religiosity scores (a measure of commitment to and motivation by religious beliefs) had more rapid remission than those with lower scores [10]. A 10-point increase in intrinsic religiosity scores resulted in a 70% increase in speed of remission, and this was after controlling for all known predictors of depression course. Bosworth and colleagues found that positive religious coping (‘I look to God for strength, support, and guidance’, ‘I work together with God as partners’, ‘I think about how my life is part of a larger spiritual force’) was related to lower depression scores at 6 months follow-up of their sample of 114 depressed older people [9]. Across the Atlantic, Braam and his Dutch colleagues found that depressed older people who professed religious faith was ‘not important’ in their lives (low religious ‘salience’) were almost six times more likely (Odds Ratio = 5.91) to experience chronic depression than those with high religious salience [11].
Findings from these three studies are highly suggestive of a relationship between religiousness and geriatric depression outcome, but as far as we are aware they are the only published papers that have examined this effect. No Australian studies to date have been conducted on this topic. It was in this context that we decided to examine the effect of religiousness on the course of major depression in a sample of elderly inpatients on the psychogeriatric unit at the Peter James Centre in outer metropolitan Melbourne, as part of a project known as the PEJAMA study (Peter James Measurements of the Aged).
In an earlier study we showed that Australian patients are less religious than their North American counterparts, with just over half rarely or never engaging in religious behaviours [12]. For a significant minority (a quarter to a third) of patients, however, religion was important. We found that 25% attended church regularly, 37% prayed, meditated, or read the Bible at least once daily, and 37% reported high intrinsic religiosity. We wanted to know, therefore, whether this religious group had a different depression course from the non-religious group, as suggested by the studies above. In particular, we were interested in three well-studied dimensions of religious behaviour as the independent religious variables: (1) organised religious activity; (2) non-organised religious activity; and (3) intrinsic religiosity. We also wanted to know whether social support was the mechanism by which religiousness exerted its effect on the course of depression.
Materials and methods
Sample
The sample consisted of 94 consecutive patients with a diagnosis of major depression admitted to the psychogeriatric ward at The Peter James Centre over the period April 2001 to September 2005. Diagnoses were made by an experienced old-age psychiatrist (VP) according to DSM-IV criteria, based on the clinician interview with the patient and scrutiny of the case notes. All patients included in the study:
a) were aged 65 years or over.
b) demonstrated an adequate command of English.
c) had no past history of bipolar disorder; and
d) had no formal diagnosis of dementia and cognitively were able to participate in the interview and complete questionnaires.
The Peter James Centre is a public geriatric hospital and is the secondary referral centre for outer eastern metropolitan Melbourne. It serves a catchment population of 100,000 persons aged 65 years and over. The aged persons’ mental health service of the hospital accepts referrals from general practitioners, general hospitals, psychiatrists, hostels, nursing homes, and other aged care facilities. Referrals are assessed by the Centre's psychiatric community team and are then either managed by the community team or admitted into the psychogeriatric unit. Following discharge from the unit, patients are followed up by the community team until they are well enough for referral back to their general practitioner.
Procedures and measures
Ethical approval for this study was obtained from the Peter James Centre ethics committee.
Interviews and questionnaires were conducted by one of the authors (VP) within one week of admission and then at 6, 12 and 24 months following admission. If the patient had already been discharged home, follow-up interviews were conducted by telephone.
The following information was collected on standardised forms:
1) Patient demographics (age, gender, marital status, country of birth, and level of education).
2) Cognitive function measured by the Mini Mental State Examination (MMSE).
3) An assessment of mood using the 15-item Geriatric Depression Rating Scale (GDRS).
4) Religiosity using the Duke University Religion Index (DUREL) [13].
5) Physical pain using a visual analogue scale ranging from 0 (‘no pain’) to 10 (‘terrible pain’).
6) Functional status using the Crichton Geriatric Behaviour Rating Scale.
7) Section H of the Cambridge Mental Disorders of the Elderly Examination including information on number of chronic illnesses, alcohol and tobacco consumption, past psychiatric history, and family psychiatric history.
8) Social support using the Social Support Questionnaire [14].
9) Exercise frequency.
Our earlier publication outlines a more detailed description of the psychometric properties of some of these scales [12].
Depression was measured using the 15-item GDRS at 6, 12 and 24 months. The 30-item version of the GDRS has been found to be both reliable and valid when administered by telephone to participants living in a variety of settings [15].
A retrospective file audit was conducted to obtain information on types of treatments received. These were divided into four categories: inpatient electrocovulsive therapy, outpatient maintenance electroconvulsive therapy, antidepressant therapy, and psychotherapy.
Statistical analysis
All analyses were conducted using the software package Statistical Package for the Social Sciences version 14.
Missing GDRS scores were identified at 6, 12 and 24 months. Fourteen of the missing GDRS scores were estimated using a regression equation that predicted depression scores at 24 months from 12 months. Differences between those individuals who participated in the initial analysis and those who were included in the 24-month analysis (including estimated scores) were examined using MANOVA.
Pearson correlation was used in the bivariate analysis of depression scores with cognitive, physical and social variables at admission, 6-, 12- and 24-month scores (including the estimated scores).
Sequential multiple regression was used for the main analysis to determine whether addition of social support variables and then intrinsic religiosity improved prediction of the level of depression at 24 months beyond that afforded by health and treatment variables. Potential predictors of depression at 24 months were selected on the basis that there was a Pearson correlation with significance value of <0.05 at 24 months and if there was a Pearson correlation with significance value of P < 0.01 with any variable at an earlier time point. In order to avoid problems with over fitting of the data set associated with an insufficient ratio of cases per independent variables in the main analysis, only those health and treatment variables that were left in the final model of a backwards elimination regression analysis were included in the main analysis.
The predictor variables were entered into the model in a stepwise fashion. In the first step the predictor variables included number of strokes, duration of exercise, and GDRS scores; in the second step overall social support, frequency of attendance at a club or social function and presence of a partner were added to determine how much extra variance was accounted for by social support predictors; finally, in the third step intrinsic religiosity was added to determine its unique contribution over and above the other variables.
In order to review the extent to which the method of estimating missing data points may have introduced bias, we have also reported the results of using a standard regression model using two other methods for handling missing data: firstly, when no attempt was made to impute any missing data points, and secondly when scores at 12 months were brought forward to substitute for missing 24-month scores.
A repeated measures MANOVA analysis was conducted to determine whether there were any significant differences in GDRS scores between each of three intrinsic religiosity groups (equally divided into low, medium and high) at each time point.
Results
Missing data analysis
At 6 months, 24% of data (or 23 cases) were missing, including four dead, five refusals and 12 who were not contactable. At 12 months 26% (or 24 cases) were missing including four dead, one ill, eight refusals and 10 who were not contactable. By 24 months 40% (or 38 cases) were missing including 12 dead, two ill, 10 refusals and 12 who were not contactable.
Differences between those individuals who participated in the initial analyses and those who had exited at 24 months (including estimated scores) were investigated using a MANOVA including all of the dependent variables, to determine if there were any systematic biases in the missing group (now largely consisting of those who had died). Significant differences were not observed between the two groups in terms of initial level of depression. There were also no differences in the social, religious or demographic variables. However, differences were observed between the two groups in relation to a number of medical/ illness-related variables, including history of strokes (F = 10.31, P < 0.01), functional status as measured by the Crichton ADL scale (F = 6.56, P < 0.05) and chronic illness (F = 6.38, P < 0.05) whereby in each case participants who had exited the study (largely due to death or illness) were found to have already been less healthy on admission. Another difference between the two groups was the age of onset of psychiatric illness (F = 10.52, P < 0.01), with the group remaining in the study having a much later age of onset (x = 58.94, SD = 3.6) than those who had exited the study (x = 29.33, SD = 8.38), suggesting there was a higher proportion of people with chronic depression in the missing group.
Demographic characteristics
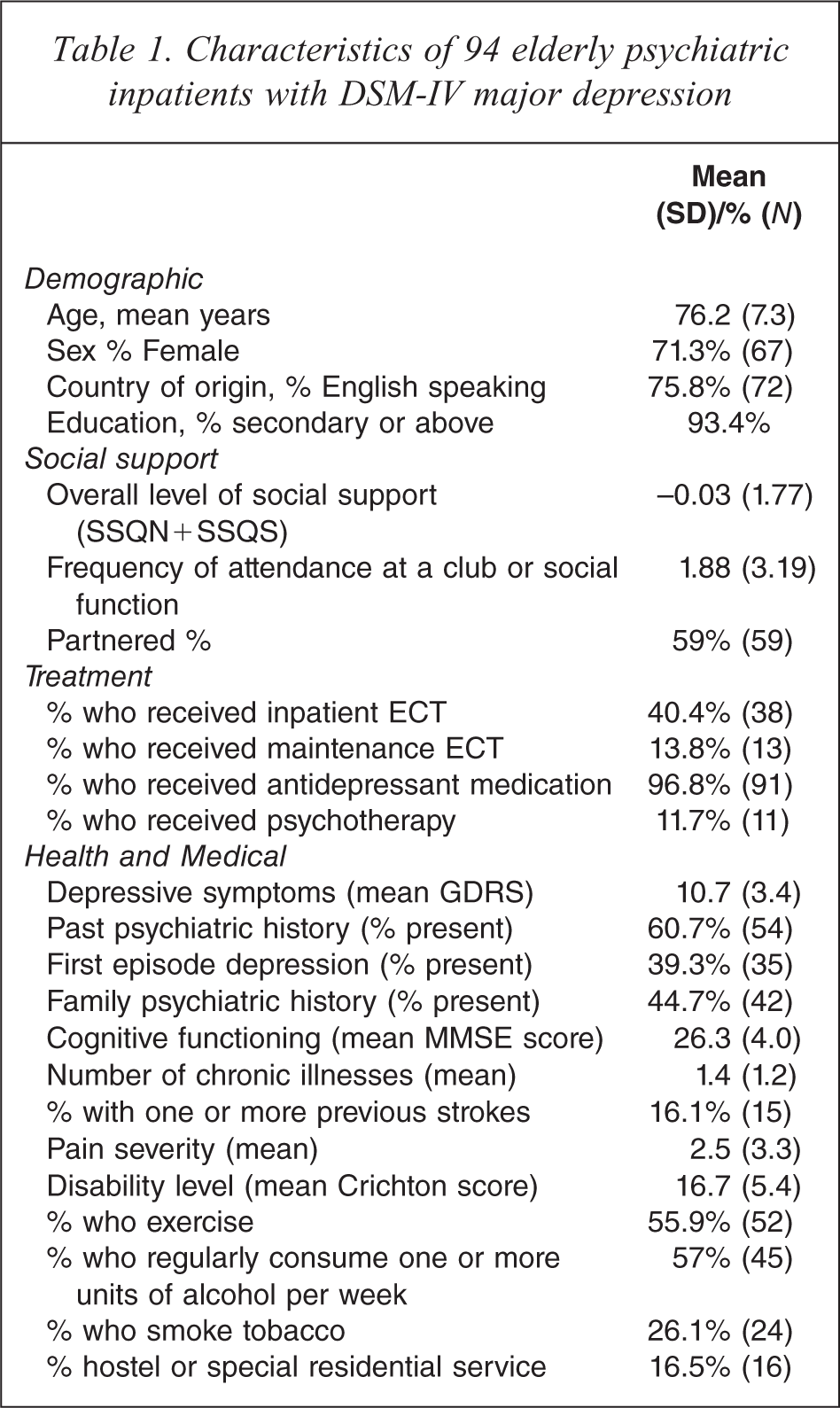
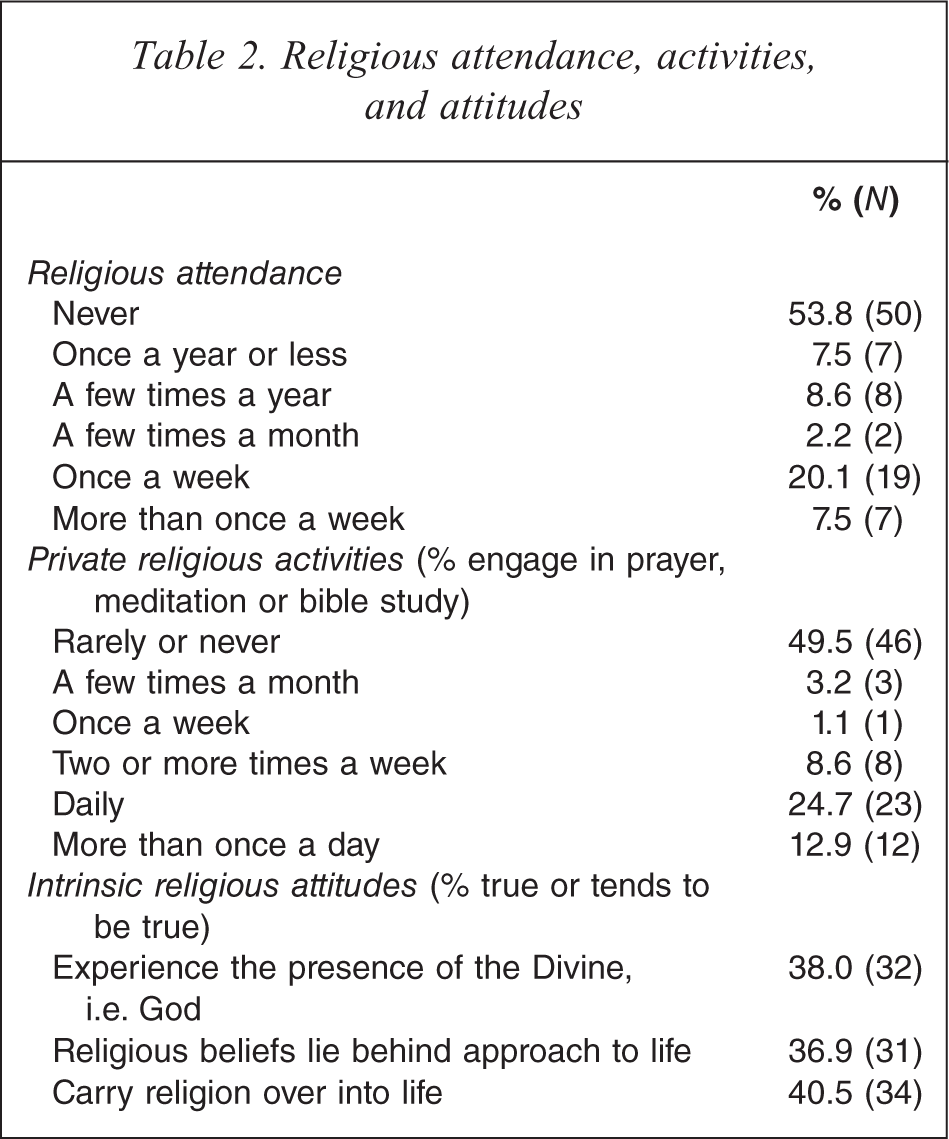
Demographic characteristics of the sample and mean values and percentages of independent variables are summarised in Tables 1 and 2. Participants were mostly women from an English-speaking background, and with at least some secondary education. Most lived independently in their own homes. Mean GDRS score on admission was 10.7 (SD = 3.4), indicating high levels of depression, and 17% had a history of stroke. While a majority were non-religious, just over one-third were intrinsically religious. The religious were all of Christian denomination.
Characteristics of 94 elderly psychiatric inpatients with DSM-IV major depression
Religious attendance, activities, and attitudes
Bivariate correlations
Bivariate correlations between independent variables and GDRS scores on admission and at follow-up are shown in Table 3. In summary, key variables that emerged following bivariate correlations were the following: intrinsic religiosity was linked to lower levels of depression at 6 months and after 24 months; overall level of social support was linked to lower levels of depression on admission and at 6, 12 and 24 months; having a partner correlated with lower depression scores at 24 months; frequency of attendance at a club or social function was linked to lower levels of depression at 24 months; the provision of ECT treatment was significantly related to levels of depression on admission; the provision of maintenance ECT was significantly related to levels of depression both at admission and at 6 months post admission; a history of strokes was associated with lower likelihood of improvement at 24 months; levels of chronic illness correlated with levels of depression at 12 and 24 months; exercise correlated with lower depression scores on admission, and at 6 and 24 months; and number of past episodes of psychiatric illness correlated with higher depression at 6 months.
Bivariate correlations with demographic, physical, social and cognitive variables with depression at admission, 6, 12 and 24 months
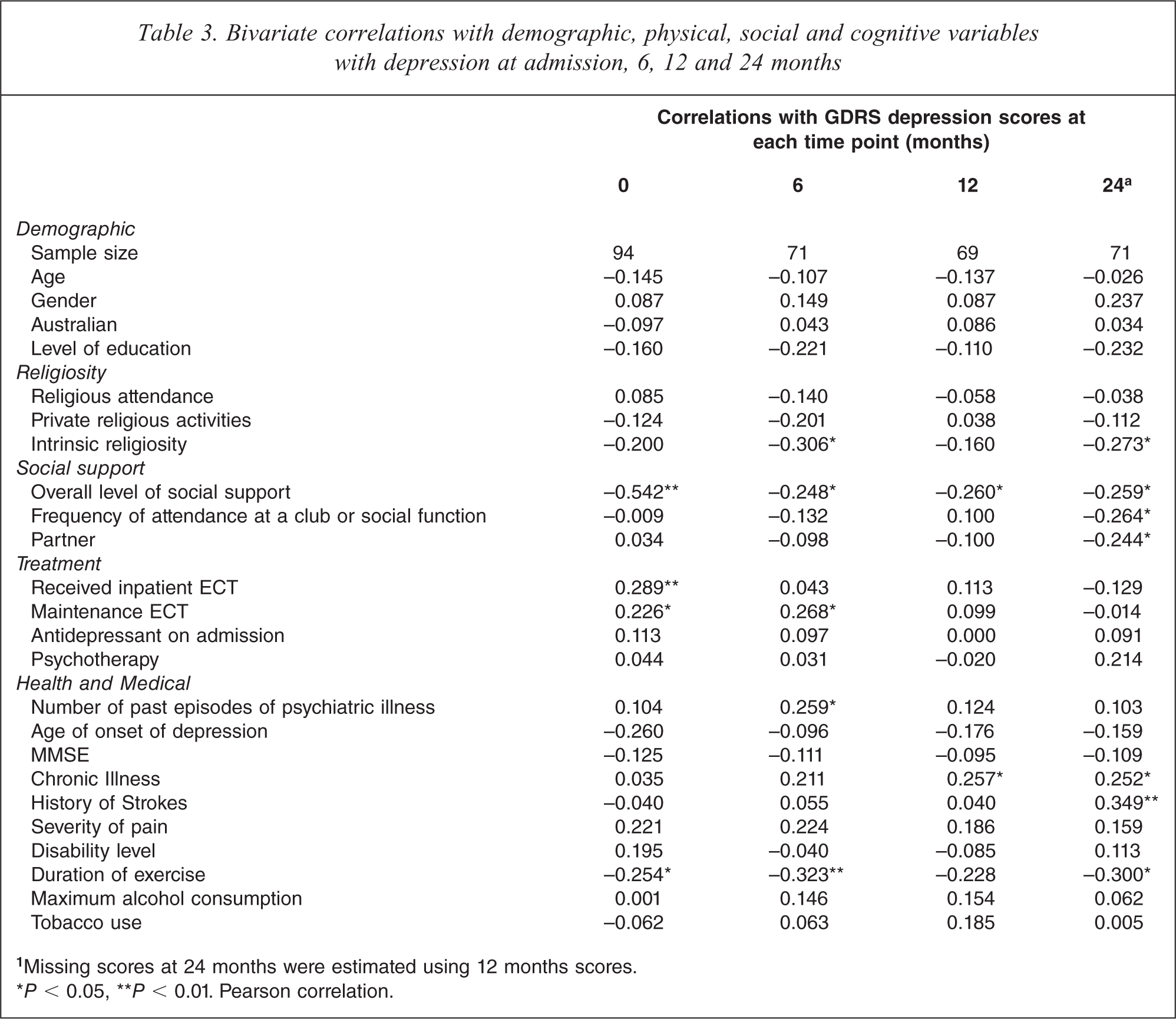
aMissing scores at 24 months were estimated using 12 months scores.
∗P < 0.05, ∗∗P < 0.01. Pearson correlation.
Independent variables that failed to emerge as significant in this study were age, cognitive status, disability levels, pain levels, maximum regular consumption of alcohol, tobacco consumption, antidepressant therapy, psychotherapy, religious attendance, and private religious activities.
Multivariate analyses
All of the main assumptions, including multicollinearity, were satisfied with the exception of two multivariate outliers identified with the use of a P < 0.001 criterion for Mahalanobis distance. These outliers were excluded from the analysis. In a backwards regression analysis using all of the potential health and treatment predictor variables to predict depression scores at 24 months, only number of strokes, duration of exercise and GDRS score were left in the final solution (R 2 = 0.194, F inc (6, 68) = 4.42, P < 0.01).
The
Step three of the main analysis: the relationship between selected admission predictor variables and depression levels at 24 months
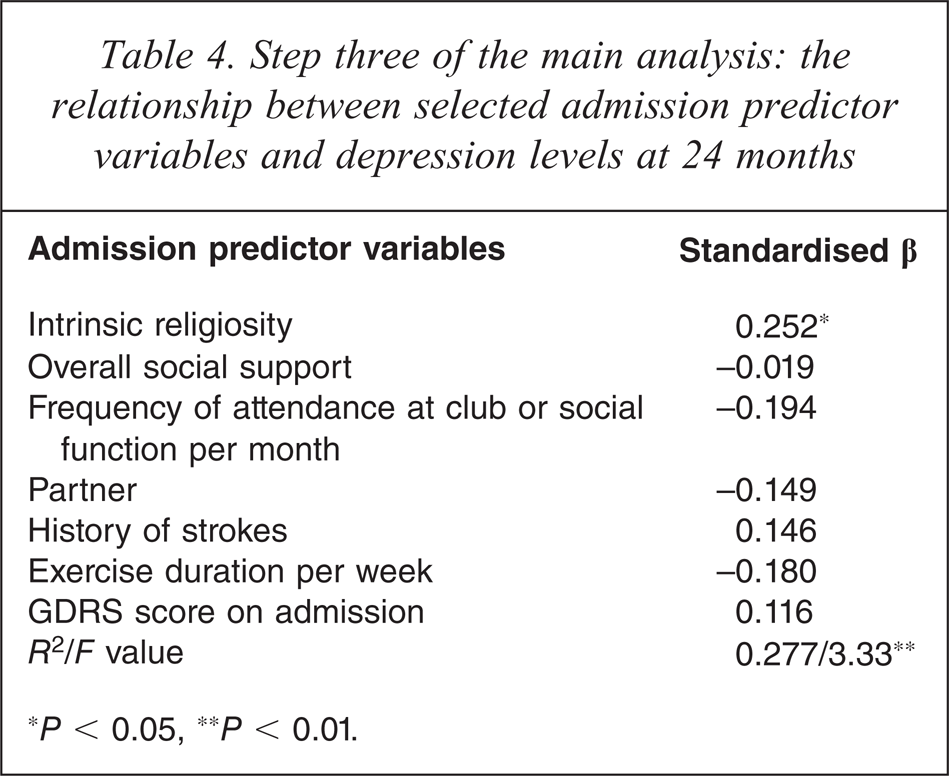
∗P < 0.05, ∗∗P < 0.01.
The two further sequential regression analyses using more conservative approaches to missing data points at 24 months revealed similar results. When there was no attempt to impute missing data points, although the data set was smaller, the results of the analysis were very similar to the main analysis, with a significant model at each of the three steps, including a statistically significant improvement with the addition of intrinsic religiosity (step 3: R 2 = 0.400, F inc (3, 38) = 3.62, P < 0.01; F change = 4.4, P < 0.05), and with intrinsic religiosity again the strongest independent predictor of depression scores at 24 months (standardised β = 0.295, P < 0.05). When 12 months regression scores were used to estimate missing data points (excluding for those who had died) each of the steps was again significant, with the final model including intrinsic religiosity significant, R 2 = 0.282, F inc (7, 69) = 3.4, P < 0.01. However, with this data set, the addition of neither social support variables nor intrinsic religiosity resulted in a statistically significant change in F (F change = 1.8, P = 0.156 and F change = 3.26, P = 0.076 for change to step 2 and step 3, respectively). In step three none of the variables were significant predictors of depression at 24 months; however, intrinsic religiosity remained the strongest independent predictor at a trend level of significance (standardised Beta = 0.214, P = 0.076).
Intrinsic religiosity
Figure 1 provides a graphic example of the impact of levels of intrinsic religiosity on levels of depression at each time point. Participants were divided into three equal groups based on their initial level of intrinsic religiosity. The graph shows that participants with high levels of intrinsic religiosity were less depressed on admission and remained less depressed throughout the 2 years post-admission, consistent with significant correlational findings at 6 and 24 months. Groups with low and medium levels of intrinsic religiosity appeared to remain more depressed throughout the 2-year period. A repeated measures MANOVA analysis revealed a significant difference between the highest and lowest intrinsic religious groups in GDRS scores across all time points, contrast estimate = 2.68, P < 0.05.
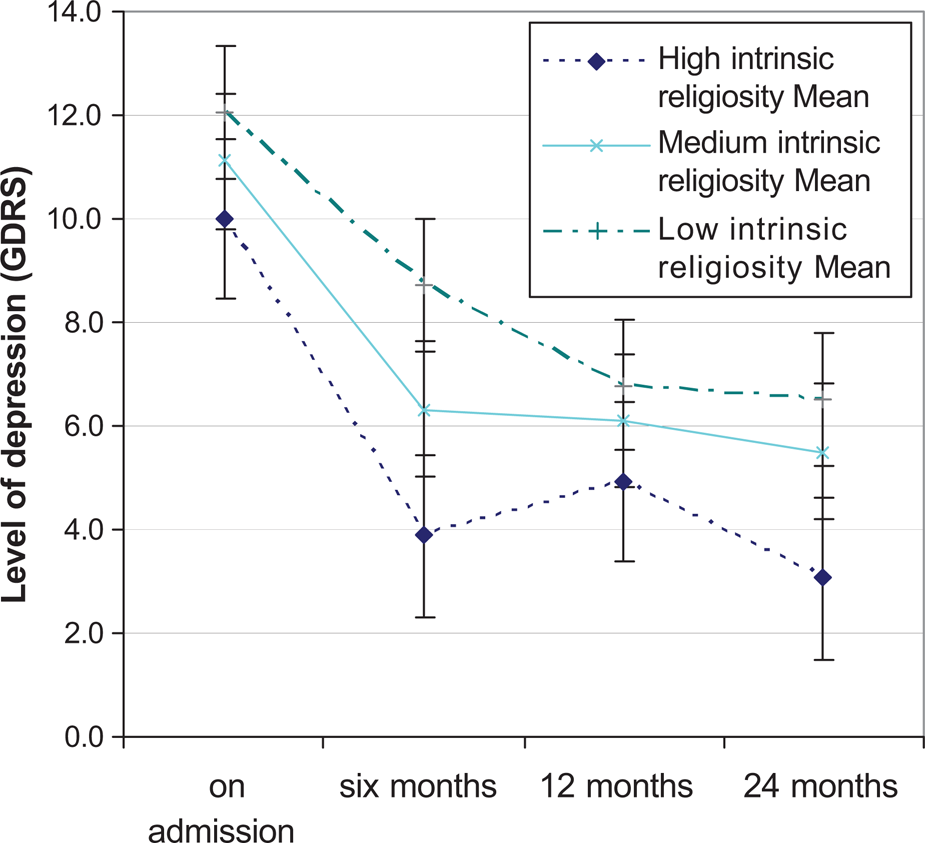
Mean levels of depression (GDRS Score) among participants with low, medium and high levels of intrinsic religiosity. NB: Error bars represent the standard error of the mean (SE = s/=n).
Discussion
Our study found that intrinsic religiosity, a measure of commitment to and motivation by religious beliefs significantly predicted depression scores at 24 months follow-up after an episode of geriatric major depression. Higher intrinsic religiosity on admission was predictive of lower depression scores as measured by the Geriatric Depression Rating Scale (short form), a 15-item patient-rated measure for depression in the elderly. This effect was independent of social support. Patients with high intrinsic religiosity also scored consistently lower on average on the GDRS at each of the four time points measured in this study (admission, 6, 12 and 24 months) than those with medium or low levels of intrinsic religiosity.
These findings are consistent with those of the Koenig study, in which older patients with high intrinsic religiosity had more rapid remission from geriatric depression during a 12-month follow-up than those with low intrinsic religiosity [10]. Our study also found that the positive impact of intrinsic religiosity extended beyond 12–24 months.
Although previous studies have confirmed the positive effect of social support on the outcome of geriatric depression [7], our study found that social support, using different measurement approaches, correlated with lower GDRS scores at each time point, but did not add any unique predictive value for GDRS scores at 24 months in our main multiple regression analysis. This suggests that the predictive effect of intrinsic religiosity on depression outcome was not dependent on social support, but due to some other unidentified mechanism.
Koenig and colleagues suggested that religious faith offers a sense of hope to elderly patients confronting physical illness and disability, making them more motivated to recover emotionally [10]. Religious people may also be more co-operative with treatment and follow-up. Although treatment compliance was not controlled for in our study, it was found to be non-significant in the Koenig study, Another possible mechanism that may account for our main finding is that religious people are more likely to conceal depression because of embarrassment at not living up to the joy and optimism supposedly characteristic of a religious life. This is a possible explanation in studies like ours where a self-rated scale of depression is used as the outcome measure. Although this explanation has some merit, some authors have contended that religion engenders guilt and self-depreciation [16]. If this is true, then religious people should score more highly on self-rated depression scores. Another counter-argument is that religious people might be on the whole more truthful than non-religious people, because of their fear of a punishing God or because of positive commitment to truth-telling, and so are more likely to provide an accurate account of their mental state.
Organised religious activities, such as attendance at church, and private religious activities, such as prayer and meditation, had no predictive effect on the outcome of geriatric depression in this study. These findings are again consistent with previous longitudinal research in this area [9,10]. In the case of organised activities, the lack of an effect may be explained by the fact that measures of organisational religious activity fail to capture the religiousness of people who are too ill or depressed to attend Church [17].
Measures of stroke, chronic illness, and physical disability failed to attain predictive significance in our study, which is not consistent with past research in the field [18]. The absence of a physical examination to assess level of active disease, and the lack of radiological assessments, may be partly responsible for this difference.
This study is the first, as far as we are aware, to investigate the impact of religion on outcomes for a sample of psychogeriatric inpatients, in this case with major depression. It is also the first to follow up the impact of religion on depressed elderly inpatients to 24 months, and the first on an Australian sample. Its findings also add weight to previous literature demonstrating the positive impact of intrinsic religiosity on the outcome of major depression in the elderly.
Admittedly, we need to highlight some design limitations that temper the study's validity. First, it is possible that low statistical power was responsible for the failure of some variables, such as social support, duration of exercise and number of strokes, to attain statistical significance in the multivariate analysis. Second, the lack of blindness may be considered a problem. The psychogeriatrician (VP) who performed the initial assessment on patients, and who was therefore privy to information about patients’ religiosity, also performed the follow-up depression assessments at 6, 12 and 24 months. However, one has to remember that the Geriatric Depression Rating Scale is a patient-rated scale in which patients have to respond ‘Yes’ or ‘No’ to 15 statements. The likelihood of the rater either consciously or unconsciously influencing the outcome of these answers over the telephone is therefore minimal.
The main limitation of the study was the high rate of attrition at 24 months (40%). Some authors would consider this to be unacceptably high [19]. However, a drop-out rate of such magnitude is not unusual for prognosis studies in the elderly. Depressed older people, in particular, have higher mortality and morbidity rates than non-depressed older or younger patients. A minority will have chronic depression, making refusal more likely, and many may change their accommodation, making them difficult to trace. Our attrition rate over a period of 24 months was certainly no less than, for example, that reported in the Braam study (163/340 or 48% lost to follow-up in a 12-month period) or the Koenig study (20/87 or 23% lost in 12 months) [10,11]. In any case, although dropouts in this study were more likely to be disabled from stroke and chronic illness, they were no different in terms of religiousness, and so their absence in the 24-month analysis is unlikely to affect the main findings of this study.
To what extent can this study be generalised? The sample in this study consisted of elderly inpatients with depression severe enough to warrant admission to hospital, or medication-resistant or non-compliant patients where either electroconvulsive therapy or supervised medication treatment were considered necessary. Generalisation of our sample to community-dwelling depressed older people should therefore be exercised with caution. Nevertheless, our sample would be representative of a section of community-dwelling older people with depression at the more severe end of the spectrum. Furthermore, it is probable that intrinsic religiosity would have as great an effect on those with milder or subsyndromal depressions living in the community as on those with more severe depression requiring inpatient treatment. The study sample was also entirely of Christian denomination—not by design, but because the outer east of Melbourne is recognised as its ‘Bible belt’. The study's findings therefore may not generalise to populations with a greater multi-faith mix.
We recommend further research on the impact of religiosity on depression prognosis, looking in particular at community samples, younger patients, and people from non-Christian faiths. Valid and reliable instruments would first need to be developed for other religious groups. It would also be worthwhile studying religiosity's effects on other mental illnesses, such as anxiety disorders and addictions. Theoretical mechanisms also need to be elucidated. It would be useful to determine whether religious people are more hopeful and less suicidal than their non-religious counterparts while suffering from major depression, as this can influence the setting for treatment. The possibility of religious people being more compliant with treatment is also worth exploring. The hoary question of whether religious people conceal their depression also needs to be answered.
This study has at least a couple of clinical implications. First, only 6.3% of Australian and New Zealand psychogeriatricians routinely ask about their patients’ religiosity [20]. We encourage all psychogeriatricians to take a religious history from their patients so that they might make more informed judgements about depression prognosis. The difference in prognosis between somebody with low intrinsic religiosity and somebody with high intrinsic religiosity may be, on average, as much as 4 points out of 15 on the GDRS at 24 months post-admission. Second, we encourage psychogeriatricians to validate their patients’ religiosity. This can be done in a number of ways: for example, ensuring referral and access to hospital chaplains and chapels, and enlisting the support of the patient's faith community (if requested by the patient).
This paper also raises an important social policy question. Religion has traditionally been a source of existential meaning for older people in the face of personal loss and social change. The findings of this paper suggest that the religious older person is more likely to recover from depression than his non-religious counterpart. If so, then to what extent should religion be actively promoted as a tool to enhance adaptation to the inevitable losses of old age?
Footnotes
Acknowledgements
Professor Yvonne Wells at the Lincoln Centre for Research on Ageing, Australian Institute for Primary Care, La Trobe University for comments on the paper and guidance with the statistical analysis.