
Abstract
Attention-deficit-hyperactivity disorder (ADHD) is a prevalent and chronic neurobehavioural condition in which individuals have core symptoms of inattention, impulsivity, and/or hyperactivity [1]. Slow reaction time, impulsiveness, poor vehicle handling, inconsistent rule following and reduced attention contribute to unsafe driving in individuals with ADHD [2,3]. Consequently, a meta-analysis of studies investigating driving outcomes for adults with ADHD found that those drivers were 1.88 times (95% CI: 1.42–2.50) more likely to crash than drivers without ADHD [4]. The studies included in this meta-analysis used mixed gender samples, although there was a strong bias towards having more male participants. Similarly, recent longitudinal research involving a predominantly male (91%) sample of adults with ADHD found that they experienced more driving citations, violations, and motor vehicle collisions than non-ADHD drivers [5]. Although males outnumber females in most driving studies of people with ADHD, this is unsurprising given that the male:female gender ratios for community samples are typically around 3:1, and that referral rate gender ratios for clinical groups are even higher, ranging between 5:1 and 9:1 [6]. At present, relationships between gender, ADHD, and crash risk are unclear. However, given the higher referral rates of males with ADHD for treatment [6], and the consideration that males in the general population are at greater risk than females for adverse driving outcomes [7], and early mortality [8], there is clear public health benefit associated with addressing the high crash risk of males with ADHD.
Countermeasures to address underlying executive functioning problems for drivers with ADHD currently focus on pharmacological management [9]. However, between 20% and 50% of adults are considered to be non-responders to stimulant medication [10]. These non-responders tend to have significant residual symptoms that cause functional impairment [11]. A multimodal approach to improve quality of life and functioning of adults with ADHD has been recommended [12,13]. One alternative approach that might complement psychopharmacological management in increasing driving safety is hazard perception training [14].
Hazard perception in driving can be described as the ability to ‘read the road’ and recognize potentially dangerous situations in the traffic environment [14] and has been found to correlate with drivers’ crash involvement [15–18]. There is increasing evidence that video- or computer-based training can improve performance on tests of hazard perception for high-risk populations, such as older drivers over 65 years [19] and novice drivers [20–22]. Importantly, some of these training effects have been found to translate into hazard recognition during real driving [20]. It is unknown whether hazard perception is amenable to training in males with ADHD symptoms. If so, incorporating a relatively simple and brief training program into a clinical management program to improve driver safety for these individuals has considerable merit. We anticipate that such a training program would need to be specifically tailored to maximize attention and minimize distractions, and be delivered in a supportive one-on-one environment with frequent breaks, in order to reduce the impact of symptoms of hyperactivity, inattention and distractibility on the attainment of positive training outcomes.
The principal aim of the study was to develop and test a tailored hazard perception training program for males with ADHD symptoms. We predicted that males with ADHD symptoms who completed a targeted hazard perception training intervention would become faster at responding to hazards in a video-based hazard perception test compared with males with ADHD symptoms not trained in hazard perception.
Methods
Participants
Forty-four participants were assessed for eligibility, of whom 20 males were included in the study. Participants’ symptoms for total ADHD exceeded the threshold of 1.5 standard deviations above the mean for age and gender on the ADHD Current Symptoms Scale for Adults – Self Report Form (CSS-A) [6]. This threshold represents approximately the 93rd percentile and is regarded as indicating clinically significant symptoms of ADHD [6]. Total symptom counts were distributed between the ADHD-combined subtype and the ADHD-inattention subtype with no participants reporting symptoms consistent with the ADHD-hyperactivity/impulsivity subtype. Presence of ADHD symptoms during childhood was reported by all study participants [23], and one-quarter had been formally diagnosed during adulthood, within the past 3 years. In addition, comorbid psychiatric conditions were self reported by 30% of participants.
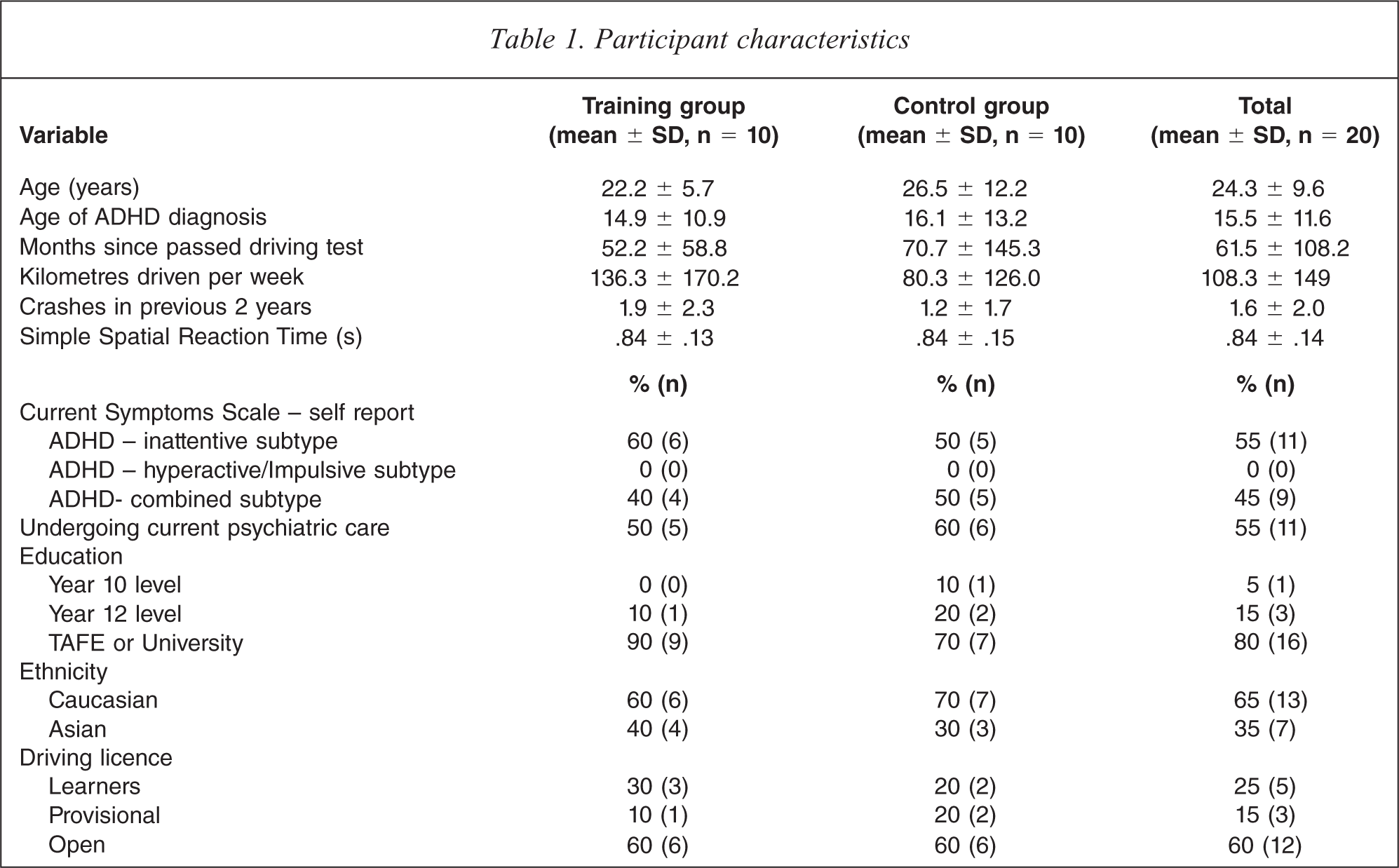
Participants included seven psychiatrist- or paediatrician-referred and 13 community-derived (i.e. non-medically referred) individuals, ranging in age from 16.5 to 58.3 years. Table 1 describes the overall sample and each experimental group in detail. The sample was comprised primarily of students (80%) from middle to high socioeconomic status backgrounds (85%), with English as their first language (65%). The number of kilometres they reported driving per week varied widely (range 0–500 km), and two participants indicated that they currently drove zero kilometres per week. These were both learner drivers, one of whom had held his learner's permit for 5 years. All participants reported normal or corrected-to-normal vision.
Participant characteristics
Materials
The Current Symptoms Scale – Adult (CSS-A) [6] contains 18 symptoms for ADHD derived from DSM-IV-TRTM criteria [1]. Participants rate symptom presence, childhood onset of symptoms and functional impact using a dichotomous rating scale.
Hazard perception tests
The hazard perception tests involved participants viewing a series of video clips of genuine traffic scenes filmed from the driver's perspective, some of which contained one or more traffic conflicts. A traffic conflict was defined as a situation where the camera car had to slow down or change course to avoid a collision. Participants viewed the traffic clips on a computer (19 inch monitor) and were required to use the computer mouse to click on any other road user (including any moving or stationary vehicle, cyclist, or pedestrian) that was likely to become involved in a traffic conflict with the camera car. They were instructed to try to predict traffic conflicts as early as possible. In one example, the camera car is following another vehicle along an urban road. Further down the road, a taxi performs a U-turn, making it likely that the leading vehicle would eventually have to brake and hence create a traffic conflict with the camera car. It is possible to anticipate this traffic conflict and respond early if one is scanning the road ahead of the leading vehicle and the taxi is detected. However, a driver who is only monitoring the car directly in front (and does not see the taxi) might only respond when the leading vehicle brakes, resulting in a slower response time.
The clips used for the tests in the present experiment were selected from tests that had been previously validated by demonstrating that they could distinguish novice from experienced drivers [24–27]. The selected clips were randomly allocated to one of two tests. Participants’ response times to the 27 traffic conflicts in test 1 and the 25 traffic conflicts in test 2 were measured using custom software (response times were calculated from the point at which it was first possible to detect that the relevant road user was likely to be involved in a traffic conflict to the point when participants clicked on the road user). Note that response times for the hazard perception test were measured automatically by the computer. Hence, experimenter judgement was not involved, and could not account for any difference in response times between groups. The tests were scored by taking the mean of standardized response times (z scores) to each traffic conflict. This ensured that (i) traffic conflicts with longer mean response times did not have an undue influence on the means and (ii) that test 1 could be directly compared with test 2 (bearing in mind that the test order was counterbalanced – see Procedure). For ease of interpretation, the overall standardized scores were converted back to response times in seconds using the overall mean and standard deviation of responses to test 1.
Spatial reaction time test
In order to check for pre-existing differences in simple reaction time and in ability to use the computer mouse between the groups, participants completed a spatial reaction time test. In the test, participants used the mouse to click on high contrast rectangles of differing sizes that appeared one at a time at random locations on the screen. Each rectangle remained visible for 2 seconds, with a random delay (between 5 and 8 seconds) between each presentation. The test was scored by taking the mean response time to the 15 rectangles presented.
Hazard perception training
The training package consisted of a main instructional video and two types of video-based exercise. The main video (18 minutes) gave advice on how to anticipate traffic conflicts and explained how to use the video-based exercises (an example of each type of exercise was included in the main video). Note that the training was presented in terms of hazard perception during real driving and not in terms of how to achieve faster scores on hazard perception tests. Following the main training video, participants completed four examples of each type of video-based exercise. The two exercise-types were presented in an interleaved order so as to provide variety, addressing the faster than normal habituation to sensation experienced by individuals with ADHD [28]. The total duration of the training video material was 34 minutes. All the traffic clips used in the exercises depicted genuine, unstaged events that occurred during normal driving.
Each exercise of the first type (‘commentary drive’) involved participants viewing a continuous video sequence shot from the driver's perspective, while generating a spontaneous ongoing commentary, in which they described out loud what they were paying attention to on the road ahead. The clip was then replayed with an accompanying pre-recorded commentary by an expert driver, so that the participant could see if they had noticed all of the features that the expert described. Each clip contained at least one traffic conflict. These techniques (either using self-generated commentaries or listening to expert commentaries) have been found to improve hazard perception latencies in previous work [21,22]. The expert commentaries were created by asking three expert drivers to provide spontaneous commentaries while watching the video clips, then transcribing and combining these into a single scripted commentary to minimize the chance that anything was missed. The final script was approved by one of the experts, who were all ex-driving examiners. The final scripted expert commentaries were dubbed onto the video clips using a professional voice-over artist.
Each exercise of the second type (‘what happens next?’) incorporated a traffic clip that cut to a black screen at a pre-specified point. The cut-point was the earliest point from which all three of our experts could predict the impending traffic conflict accurately. Upon reaching the cut-point, participants were required to list all the things that might plausibly happen next. The clip was then played again. When the cut-point was reached, the video image froze and participants heard an expert talking through the possible outcomes (this ‘expert opinion’ was a combination of the opinions of the three experts used to create the commentary drives). Finally, the clip was played past the cut point so that participants could see what actually happened next (the expert opinion always included the true outcome). This exercise was based on McKenna and Crick's [29] predictions training task. Tasks of this kind have been found to improve hazard perception skill [29] and to distinguish novices from experienced drivers [30].
After each exercise, the occupational therapist conducting the training session interacted with the participant, highlighting hazards that had been missed and answering any questions. This also served to focus attention on the training process.
Control intervention
An intervention was created to act as a control for the hazard perception training. This contained video clips in which driving instructors gave advice on aspects of road safety not related to hazard perception (e.g. vehicle checks before driving and lane discipline on roundabouts). It also contained all the traffic clips used in the hazard perception training (edited without voice-overs or other instruction). This was to ensure that any training effect was not due to simple exposure to additional traffic clips and hazardous situations similar to those seen in the tests. The occupational therapist answered any questions raised during presentation of this information and encouraged participants to keep watching the video when their attention flagged. The control video materials were of the same total duration as the training materials (34 minutes).
Procedure
Recruitment and screening
Following ethics approval from the Behavioural and Social Sciences Ethics Board of The University of Queensland, all medical officers listed with the Queensland branch of the Australian Medical Association as having specialty interests in ADHD were contacted to distribute information sheets to patients with ADHD. Snowballing recruitment occurred through medical networks, list serves, specialty interest groups, schools, universities and colleges of technical and further education. Volunteers were screened for eligibility in a telephone interview using the CSS-A. A large proportion of the total applicants (55%) were rejected because they did not meet strict eligibility criteria relating to number and duration of symptoms and gender. Eligible participants were invited to attend a single session conducted at The University of Queensland. To maximize ecological validity, participants were instructed to prepare for the experiment in the same way they would prepare for real driving, including taking any prescribed medications. One participant in the training condition took medication during the experiment, requesting a break to take Ritalin 10, an immediate-release stimulant medication, to boost his attention span when he noticed that his attempts to remain focused were diminishing.
Assignment to groups
Twenty participants were randomly assigned to receive either the hazard perception training package (trained group) or control intervention video (untrained group), with caveats that there would be equal numbers in each group and participants’ characteristics would be approximately matched for age and driving experience (Table 1). There were two counterbalanced conditions within each group: half the participants completed test 1 as the pre-intervention test and test 2 as the post-intervention test and the other half completed test 2 as the pre-intervention test and test 1 as the post-intervention test.
Order of presentation
In both training and non-training conditions, participants provided informed consent before completing the spatial reaction time test (90 seconds). All participants then viewed a 5-minute video explaining how to complete the hazard perception test (note that this video did not provide any instruction on how to anticipate hazards), prior to sitting the pre-intervention hazard perception test (12 minutes). Following a short break (10 minutes) participants received either training or control interventions before having another break (12 minutes). Finally, the post-intervention hazard perception test (12 minutes) was administered and a de-briefing session of 5–10 minutes concluded the experiment. Participants in the untrained group were then invited to undertake the hazard perception training and offered additional payment to compensate them for their time if they elected to do so.
Setting
Tests and training were individually administered in a dedicated office setting free from external noises, visual distractions and interruptions. To improve attention, participants were provided with optional sensory alerting modifications such as variable pressure cushions, push/pull spouts on water bottles, squeezy balls, music, chewing gum, and theraband across chair legs [26]. Scheduled breaks between testing and training components provided two opportunities during the experiment for participants to leave the office, move around, and have refreshments.
Results
There were no significant differences between the trained and untrained groups for any of the control variables listed in Table 1. To evaluate the training effect, the pre-intervention hazard perception response time was subtracted from the post-intervention hazard perception response time to give a change statistic in seconds (negative values equated to faster hazard perception response times following the intervention). A box plot of the data can be seen in Figure 1. The mean change in hazard perception response time was −0.55 seconds (SD 0.33, 95% CI −0.66 to −0.25) for the trained group and −0.08 seconds (SD 0.28, 95% CI −0.18 to 0.16) for the untrained group and the group difference was statistically significant, t (18) = 3.21, p < 0.005, Cohen's d (standardized group difference) = 1.54.
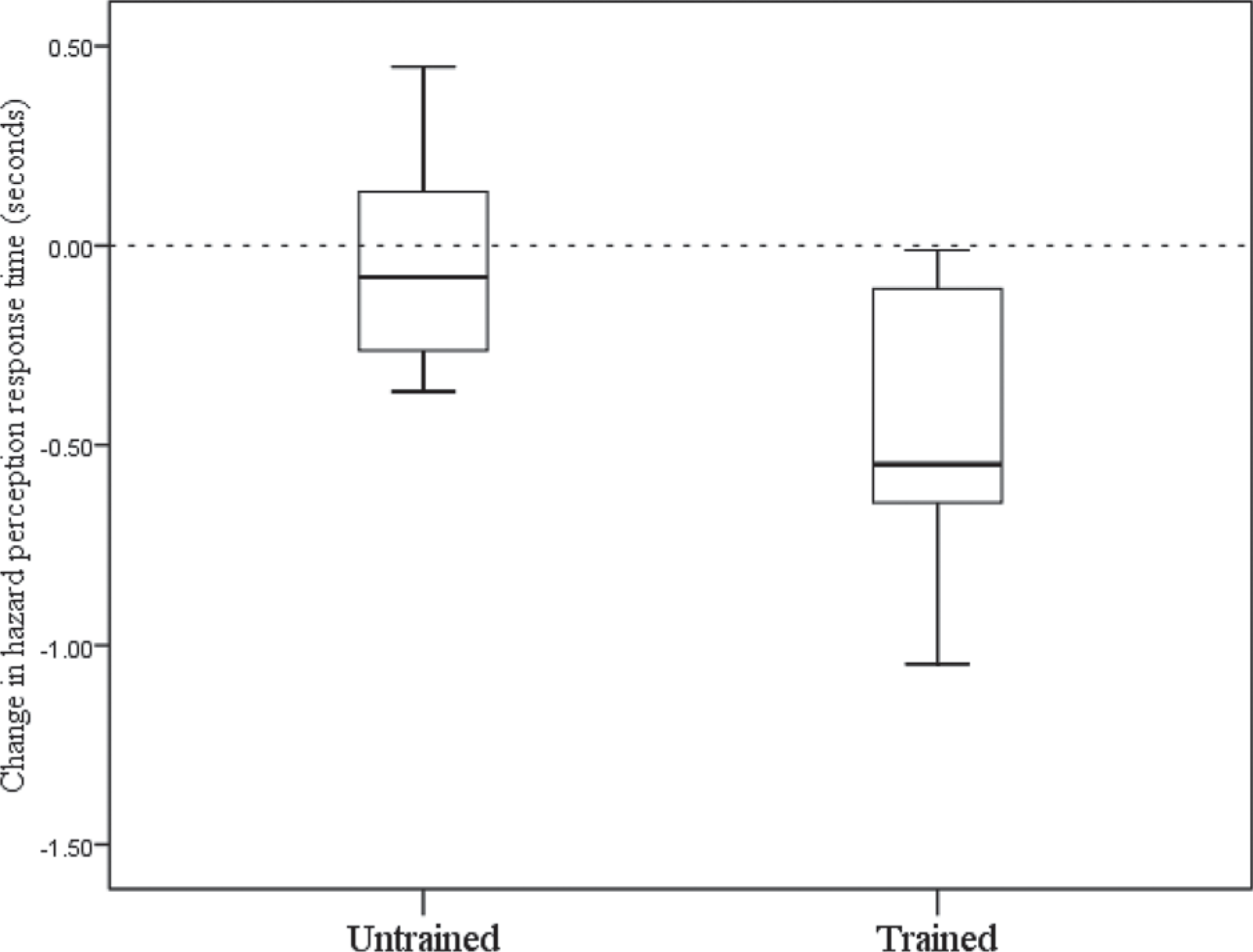
Box plots of the change in hazard perception response times following the training or placebo intervention (negative scores indicate faster responses following intervention). The boxes show the median and quartile values.
Discussion
Our findings supported the hypothesis that male drivers with ADHD symptoms who received a tailored video-based hazard perception training intervention in an office setting would improve their performance on a hazard perception test to a significantly greater extent than males with ADHD symptoms who did not receive training. This is a noteworthy result as no other study has investigated the effect of a training intervention on drivers’ hazard perception ability in this population. The results are consistent with previous findings showing that hazard perception training is effective in improving hazard perception response latencies for other high-risk groups, such as older drivers [19] and novices [20,22]. The effect size was of a similar magnitude to those obtained in previous studies.
One question that arises from these findings is why the intervention effects are so large, given the typically brief durations of this type of training. One possibility is that hazard perception is not inherently difficult but untrained participants are nonetheless unaware that engaging search strategies, even simple ones, can yield substantial dividends. There is evidence to suggest that more experienced drivers are more likely to engage in a proactive search for hazards than their less experienced counterparts [14], allowing them to anticipate such events long before they occur. Prior to training, it may not have occurred to participants to attempt even the simplest anticipatory strategy. If this was the case then any insight whatsoever into the strategies employed by expert drivers provided by the training may have been enough to produce the observed improvement.
The training appeared to benefit some individuals more than others and there are likely to be a number of reasons behind this, including individual differences in variables such as attention, motivation, treatment status, medication, age, education and pre-existing level of hazard perception ability. Hence, it would be beneficial to examine the moderating effects of these variables on the training effect. Similarly, research comparing male and female drivers with ADHD would also be informative. While the effects of individual differences cannot be tested directly using the present data (primarily because research on individual differences necessarily requires larger samples to ensure adequate statistical power), this could be a fruitful line of investigation for future work. It is worth noting that all trained participants were faster post-intervention than pre-intervention, so any such research into the effects of individual differences will most likely be informative as to degree of benefit conferred by the training rather than whether the training is beneficial per se.
One limitation of the current study was the use of a small sample of self-referred drivers, who were symptomatic at recruitment. This is a common criticism of ADHD driving studies [31]. Individuals with ADHD who drive illegally are likely to be under-represented and it is possible that they may benefit less from the training intervention as a result of being, for example, more intractable. The results should be interpreted in the light of this. In addition, future studies could investigate whether training effects generalize to more specific ADHD sub-types. For example, individuals who have predominantly hyperactive-impulsive symptoms might be of interest because these individuals are more likely to have comorbid externalizing disorders that are associated with additional driving risk [32]. A clinical assessment to corroborate self-reported symptoms is recommended for future studies that aim to replicate and extend evidence for the utility of hazard perception training for individuals with ADHD. To maximize diagnostic accuracy, these clinical assessments should ideally incorporate data collected from multiple sources, including a review of childhood and current symptom severity, comorbidities and the functional impact of ADHD across settings.
Further extensions of this study could include determining whether the training effects generalize to real driving (it is possible that training is only improving video test performance), investigating the longer term effects of the training (perhaps the effects shown are too short term to be of practical use), and separating the training package into its component parts (e.g. the two types of exercise) to discover which components are the most beneficial.
While previous research has demonstrated clear links between ADHD and negative driving outcomes, there has been a relative paucity of intervention-based studies, particularly of a non-pharmacological nature. The results of the present study indicate that hazard perception training could be a useful intervention that is practical, quick, and affordable, and has the potential to translate into real world driving outcomes.
Footnotes
Acknowledgements
The authors sincerely thank the participants who volunteered for this study. Funding support from the Occupational Therapy Board of Queensland is gratefully acknowledged. Advice from Professor Geoffrey Mitchell, Discipline of General Practice, School of Medicine, Faculty of Health, The University of Queensland, in relation to clinical considerations of ADHD, was deeply valued. The hazard perception training materials and instructions for hazard perception tests were funded by Queensland Transport. We would like to thank John Burrill and his team for their collaborative input. Filming of some driving clips was partly funded by an Australian Research Council Linkage Grant LP0668078. Special thanks to Chris Hatherly, Ben Evans, Georgina Parker, Johann Eloff, Thomas Wallis, and Shelby Marrington for their help in conducting the filming.