
Abstract
Mental disorders are a leading cause of disease burden in Australia. The Australian Burden of Disease Study conducted in 1998–99 [1] found that mental disorders including substance abuse accounted for nearly 30% of all health-related disability and that affective disorders (including depression) was the leading cause of disability for male and female subjects among all health conditions. This burden remains high, with anxiety and depression continuing to be the leading cause of health-related disability in the latest burden of disease study [2].
In 1997 the first Australian National Survey of Mental Health and Wellbeing (NSMHWB) was conducted by the Australian Bureau of Statistics (ABS) [3]. A major finding was the low treatment rates for mental disorder and substance abuse, in which 65% of all those who met the diagnostic criteria for affective, anxiety or substance use disorder did not receive any form of health service in the previous 12 months. The 12 month treatment rate was 40% for affective disorders, 28% for anxiety disorders and 14% for substance use disorders. When people did receive treatment it was general practitioners who were the most common providers [4]. Similar patterns and rates of service use are evident also in the 2007 NSMHWB [5].
One Commonwealth government response to the low treatment rates for these health conditions that were contributing such a high burden of disease was to establish a national primary mental health care initiative. Launched in June 1999 the initiative provided funding for education and skills-based training in mental health for general practitioners. Another response by Commonwealth, State and Territory governments was to increase the awareness among the population of these common disorders, especially depression, with the expectation that more individuals with untreated symptoms would present for treatment. The best known example of an initiative in this area is beyondblue: the national depression initiative [6,7].
Evidence-based treatment for depression and anxiety consists of psychological therapies, such as cognitive behavioural therapy and antidepressant medication (which can also be effective in anxiety disorders). In July 2001 the Commonwealth introduced the Better Outcomes in Mental Health Care (BOiMHC) [7], a programme that provided access to psychological services through the use of locally negotiated service contracts between Divisions of General Practice and psychologists. A total of 114 Divisions of General Practice participated in the programme, which is generally considered to be effective [8,9]. The BOiMHC programme was replaced by the Better Access to Mental Health Care Program, which expanded the access by psychologists, social workers and occupational therapists to rebates for their patients for services provided (on a fee-for-service basis) and listed on the Medicare Benefit Schedule. There followed a dramatic uptake in psychological treatments for common mental disorders [10]. This programme is currently undergoing review by the Commonwealth government.
Antidepressant medication has long been the basis of medical treatment of depression and more recently these drugs have been replacing benzodiazepines for the longer term treatment of anxiety disorders. Selective serotonin re-uptake inhibitors (SSRIs) have been subsidized on the Pharmaceutical Benefits Scheme (PBS) for ‘major depressive disorder(s)’ (fluoxetine the first in 1991), with additional listings for obsessive–compulsive disorder and panic disorder for some medications. In the years under consideration in this paper (2002–2007), sertraline, paroxetine, fluoxetine and fluvoxamine all had PBS approval for one or more anxiety disorders (obsessive–compulsive and panic disorders). While there has been recent debate about the efficacy of antidepressants [11], they remain an effective (albeit not fully satisfactory) treatment option for many patients with depression and anxiety [12]. There is even some evidence for a reduction in suicide rates with increased use of SSRI antidepressants [13], although prescribing may only be a proxy for the recognition and attempt to help a person with suicidal ideation.
Antidepressant medication prescribing has escalated dramatically in Australia [13–15], with venlafaxine (listed on the PBS in February 1999) now one of the most costly drugs subsidized by the PBS [16]. One concern with antidepressant medication is whether patients, other than those with depressive and anxiety disorders, are being prescribed these drugs. In this paper we examined the prevalence of depressive and anxiety disorders in adults in Australia, service utilization for these mental health problems (which may have included ‘psychological’ or pharmacological interventions) and compared these with the dispensed prescriptions of those drugs used to treat these disorders.
Methods
The 12 month prevalence of depressive and anxiety disorders and utilization of treatment services were obtained from the 2007 NSMHWB conducted by the ABS between August and December 2007. Respondents in this survey were selected at random from a stratified, multistage area probability sample of private dwellings. The population for selection was persons aged 16–85 years who were usual residents of private dwellings across Australia. From all eligible respondents an algorithm randomly selected a householder to complete a personal interview. At this point the youngest (16–24 years) and oldest (65–85 years) age groups had a higher probability of being selected. This was to ensure that sufficient samples sizes were achieved in these age groups to improve the reliability of estimates for these groups. A total of 8841 respondents completed the interview, representing a 60% response rate. The weighting design ensures nationally representative population estimates.
This survey used the World Mental Health Survey Initiative version of the Composite International Diagnostic Interview (WMH-CIDI) [17]. The WMH-CIDI has undergone extensive methodological development and testing and has been used in household surveys in 28 countries. This instrument allows for the identification of mental disorders using both the American Psychiatric Association's DSM IV and ICD-10 criteria. The diagnoses reported in this paper use ICD-10 criteria and were categorized into two classes of mental disorder: (i) affective disorders: depression, dysthymia, bipolar disorder; and (ii) anxiety disorders: agoraphobia, social phobia, panic disorder, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder.
Utilization of services was recorded by asking respondents about lifetime and 12 month consultations with a range of providers for mental health reasons [18]. For this paper we were interested only in 12 month prevalence and 12 month treatment rates. A full description of the methodology of the NSMHWB is reported elsewhere [18].
The data on the number of prescriptions for antidepressant medications were obtained from the Department of Health and Ageing. The data were drawn from two sources. The first was the Medicare Australia records of prescriptions submitted for payment of a subsidy under the Pharmaceutical Benefits and Repatriation Pharmaceutical Benefits Schemes (PBS/RPBS). The second was an ongoing survey of a representative sample of community pharmacies, which provides an estimate of the non-subsidized use of prescription medicines in the Australian community. There are two levels of PBS patient co-payments, one for general and the other for concession patients. These co-payments were AUD28.60 and AUD4.60 in 2005 and AUD29.50 and AUD4.70 in 2006 for general and concession patients, respectively. Concession beneficiaries are those who receive social security benefits because they hold a Pensioner card, a Health Care card or Commonwealth Seniors Health card [19]. The proportion of concession patients in three broad categories in 2003 was 41% low income, 23% sick or disabled, and 36% elderly. In 2007 the proportions were 35%, 24% and 42%, respectively.
De-identified data include details of the drug product dispensed and information on the gender and age of the patients. The use of prescription medicines dispensed to inpatients in public hospitals is not available in this report. In Australia, discharged patients from hospital are typically provided with only a short supply of medications, typically a maximum of 1 month's supply. Further prescriptions are provided by general practitioners in the community.
Prevalence and service use rates were estimated from the 2007 NSMHWB. Data were weighted to adjust for differences in probabilities of selection, differential non-response and other differences between the sample and the Australian population aged 16–85 years inclusive. Rates were computed as proportions for each of the age–sex strata per 1000 population. Standard errors were estimated using jackknife replicate weights. The STATA software package version 10.0 (StataCorp, College Station, TX, USA) was used for analyses conducted using the 2009 version of the confidentialized unit record file [20].
The amount of drug supplied was standardized using the defined daily dose (DDD)−1 1000 population day−1 for all drugs with an anatomical therapeutic chemical code starting with N06A (indicating antidepressants). The DDD is established by the World Health Organization Collaborating Centre for Drug Statistics Methodology. It corresponds to an estimated mean daily dose of the drug when used for its main indication in adults [21]. The number of Australians in each gender and 5 year age group was used to standardize the DDD by population [22]. All calculations were completed using Microsoft Office Excel 2003.
Results
The prevalence and treatment rates of both affective and anxiety disorders was highest in female subjects and peaked in those aged 30–39 years. In male subjects the peak prevalence and treatment rates were in those aged 40–49 years (Figure 1). After 50 years of age, both the prevalence and treatment rates decrease rapidly. The profile across the age span is similar for both genders but the prevalence and treatment for affective disorders is approximately half or less of that seen for anxiety. It would be expected that the population for whom the prescribing of antidepressant medication is highest would correspond to these age groups.
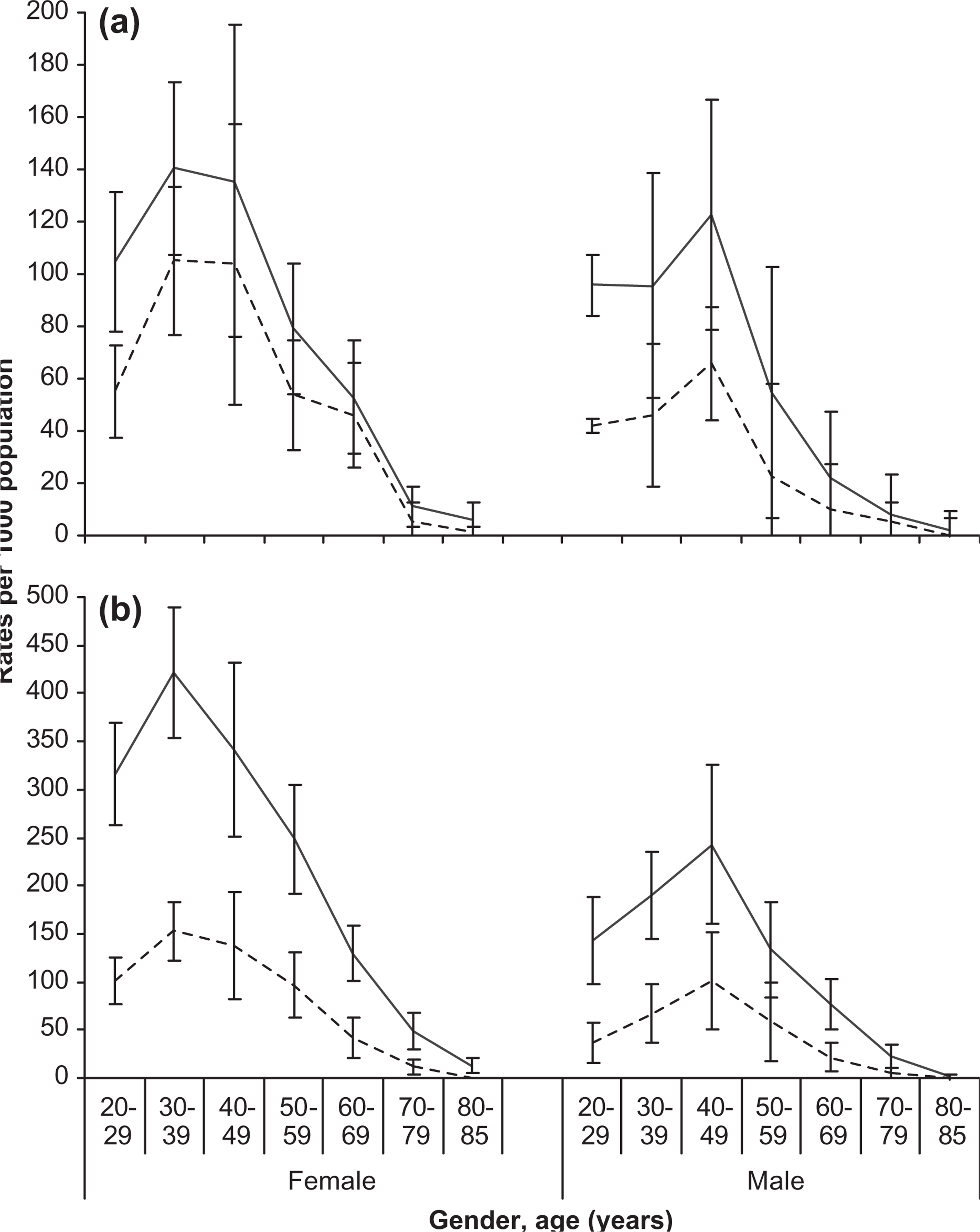
(—) Prevalence and (—) treatment rates (per 1000 population) of ICD-10 (a) affective and (b) anxiety disorders in the last 12 months vs gender and age in 2007 (with 95% confidence intervals). Note the different scales.
SSRIs are the most widely prescribed class of antidepressant, accounting for around 60% of the antidepressant DDD 1000 population−1 day−1 for women and 56% for men aged >20 years (Table 1). Total use of antidepressants was 81.35 DDD 1000 population−1 day−1. The drugs grouped into the ‘other’ category follow SSRIs in share of utilization, with the older tricyclic antidepressants (TCA) and monoamine oxidase inhibitors (MAOIs) the least commonly prescribed for either gender. Antidepressant prescribing was higher in female subjects compared to male subjects for all drug classes, as would be expected given the higher prevalence of affective and anxiety disorders and the higher treatment rates in female subjects.
Drug utilization of antidepressants in those aged ≥20 years (averaged August 2004–July 2005)
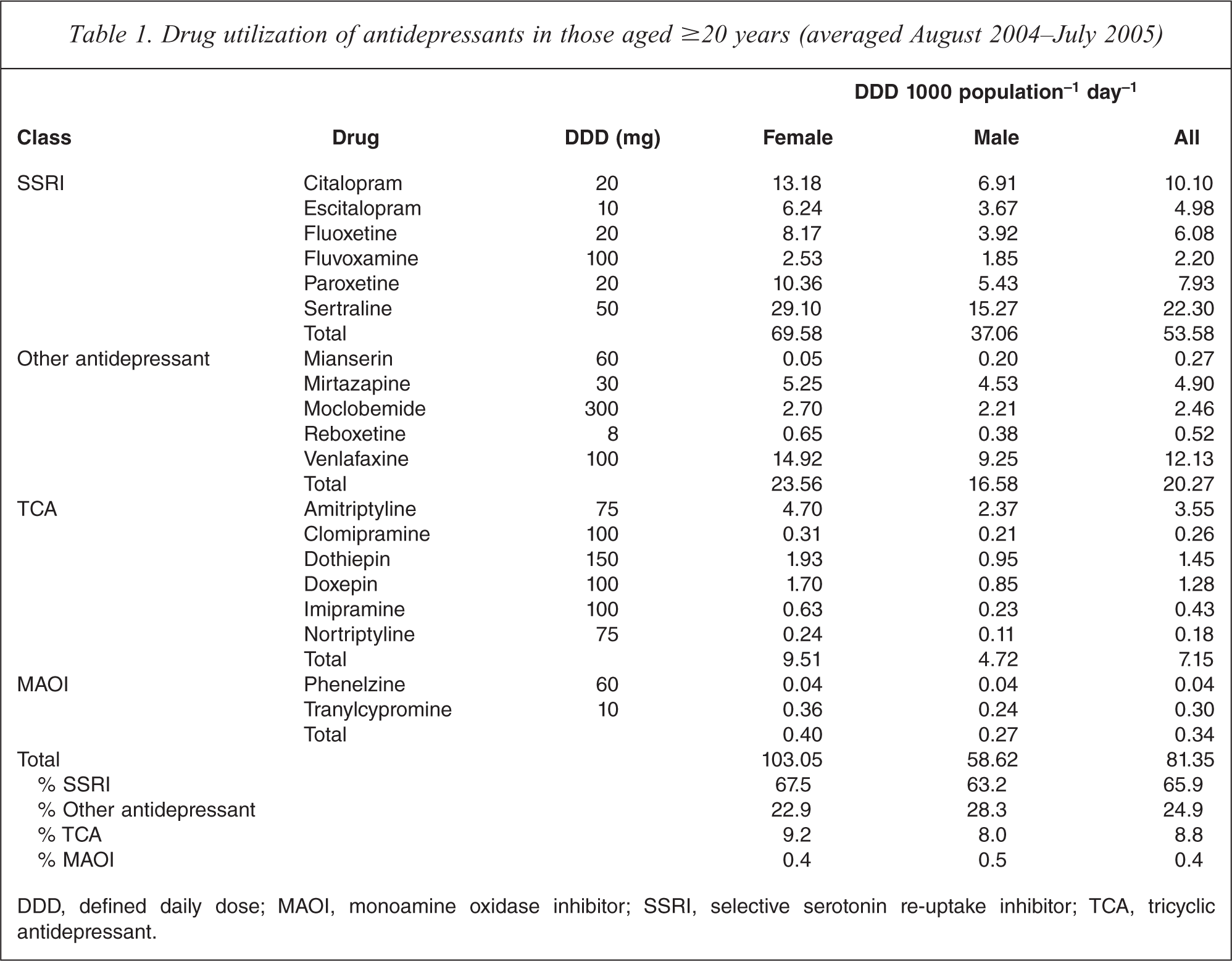
DDD, defined daily dose; MAOI, monoamine oxidase inhibitor; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
SSRI utilization (for all ages) increased 44% from 36.1 to 51.9 DDD 1000 population−1 day−1 between June 2002 and June 2007 (Figure 2). Venlafaxine utilization increased 75% from 7.4 to 13.0 DDD 1000 population−1 day−1 during the same period. ‘Other antidepressant’ use increased slightly and TCA use decreased slightly. MAOI use was very low and stable: approximately 0.3 DDD 1000 population−1 day−1 (data not shown). Total antidepressant use (i.e. all classes combined) for all ages increased 41% from 56.1 to 78.9 DDD 1000 population−1 day−1 (data not shown) during the period 2002–2007.
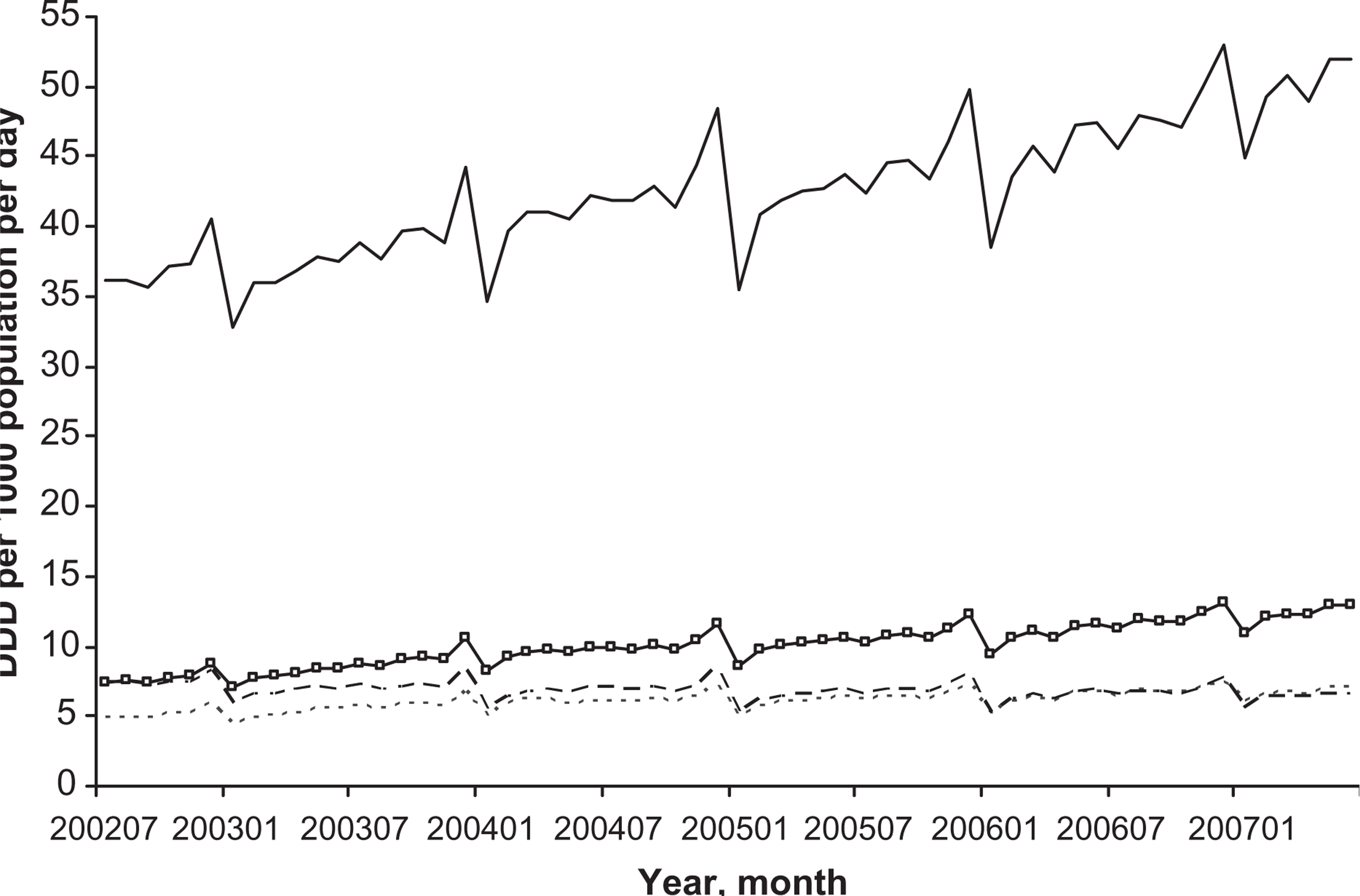
Complete antidepressant utilization between July 2002 and June 2007 vs month (all ages). DDD, defined daily dose. (—) Selective serotonin re-uptake inhibitor total; (–□–) venlafaxine; (—) other; (– – –) tricyclic antidepressant total.
There is a higher level of utilization towards the end of each calendar year. This peak is due to the safety net provisions introduced to the PBS in November 1986. Once the cash-based safety net level is reached in a calendar year, prescriptions on the scheme are either free (concessional patients), or available at the concessional co-payment amount (general patients) [23].
Antidepressant utilization increased with age in both women and men (Figure 3), with use being higher in women. There was a bimodal distribution for sertraline and citalopram (other SSRIs less obvious), with a minor peak at 55–59 years (combined total: women, 115.4; men, 79.4 DDD 1000 population−1 day−1) and a major peak at 90–94 years (combined total: women, 142.9; men, 97.7 DDD 1000 population−1 day−1 in both genders. This corresponds to approximately 14% of women and 10% of men aged 90–94 years taking a standard dose of an antidepressant each day. The age profiles of selected drug utilization were similar across the genders. Sertraline had the highest utilization, with a peak of 53.8 DDD 1000 population−1 day−1 for women and 37.9 DDD 1000 population−1 day−1 for men for those aged 90–94 years. Citalopram had its peak in the same age group (29.4 and 20.6 DDD 1000 population−1 day−1). Venlafaxine was preferentially used by younger people, with peak use in the 50s (women, 21.7 DDD 1000 population−1 day−1; men, 15.8 DDD 1000 population−1 day−1).
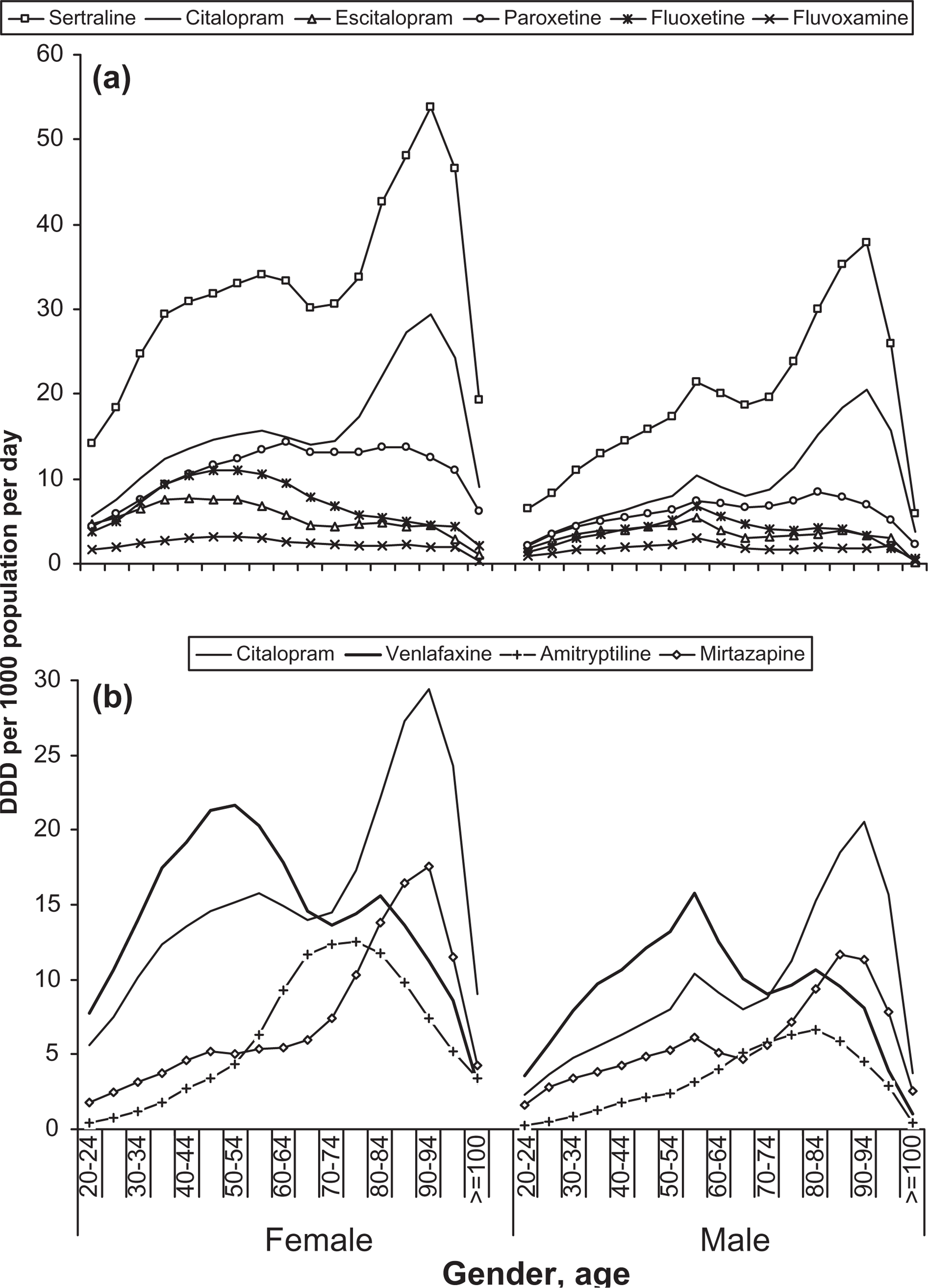
Drug utilization of selected antidepressants vs gender and age (average of August 2004–July 2005). (a) Selective serotonin re-uptake inhibitors; (b) other drugs (citalopram is common to both). Note the different scales.
Discussion
Antidepressant prescribing has grown dramatically in Australia in the last decade [13]. This is not unexpected given the findings in the 1997 NSMHWB of the low treatment rates for affective and anxiety disorders [3] and the attempts since then to increase the treatment rates. Regarding type of antidepressant, SSRIs now dominate the market, with an increase of 44% to 58 DDD 1000 population−1 day−1 over the study period. Sertraline was the most commonly prescribed antidepressant, followed by venlafaxine and citalopram. The use of venlafaxine increased 75% between June 2002 and June 2007.
The main finding of the present study is the poor alignment between the prevalence and self-reported treatment rates of affective and anxiety disorders in the community and the populations for whom antidepressant medications are being prescribed, with very high prescribing rates in those aged >85. This must be a concern for clinicians and health policy makers, especially given the escalation in the prescribing of expensive newer antidepressants. The prevalence and treatment rates of affective and anxiety disorders are highest in those aged <50 years, after which both decline rapidly. Prescribing of antidepressants, however, generally has a bimodal distribution, with peaks in those aged in their late 50s and early 90s. These results do not necessarily imply that the population aged <50 years are receiving suboptimal pharmacotherapy, but taken with other literature they do raise concerns about the potential over-prescribing for older Australians. Although improved awareness of depression among both patients and practitioners [7,24,25] could result in more people coming forward and getting treatment, this is not likely to account for the large amount of use in the elderly. The very high use of antidepressants in elderly people (≥80 years) especially warrants further exploration especially given the information that pharmacotherapy, generally, in this population is excessive [26,27]. The reasons for the different profiles of prescribing antidepressants across the age span cannot be ascertained from the present study but may, in some instances (e.g. citalopram), reflect a cohort effect.
The present findings confirm those of previous studies of antidepressant use in Australia regarding increases in use over time and more use in female than male subjects [14,28–31]. The finding that there is increased prescribing of antidepressants in the elderly has been reported in some studies in Europe and the USA [32–35] but other studies show a decrease in prescribing with age [36–38]. There is no evidence that the change in prescribing is due to a change in prevalence of depression in Australia [18] or overseas, where there has been a sharp increase in antidepressant prescribing [39].
Of course it is likely that antidepressants are prescribed for reasons other than depression and anxiety disorders [40]. Off-label prescribing (i.e. outside of approved or subsidized indications) is not uncommon. This can take three forms. First, it is possible that these medications are being prescribed for depressive and anxiety symptoms that do not reach the threshold for a diagnosis of a mental disorder. This could be seen as early intervention, but preferred clinical practice would be psychological rather than pharmacological at this stage. Second, the medications may be prescribed for diagnosable disorders for which they do not have marketing approval (e.g. somatoform disorders or eating disorders). Third, they may be prescribed for common emotional distress or insomnia, which do not constitute subthreshold symptoms of a mental disorder. The present study cannot provide information on the conditions for which antidepressants were being prescribed.
Of particular concern is the very high prescribing in those Australians over 80 years. The NSMHWB did not include respondents over the age of 85 in the survey, therefore we do not have epidemiological data on people aged 90–94, for whom the antidepressant utilization is highest. It could be that high rates of depression and/or anxiety symptoms accompany the physical illness and dementia found in this age group and that this drives the prescribing. If so, the efficacy of this is not well studied and the authors are unaware of evidence of a sudden escalation in the prevalence of diagnosable affective or anxiety disorders after the age of 85.
A strength of the present study was that it used the most recent estimates of both prevalence and treatment of affective and anxiety disorders by gender and age for Australia. In addition there was complete capture of all subsidized dispensing of antidepressants by gender and age in the Australian community. These data have been age-standardized and so there is no bias due to differential gender populations in each age group. There are several limitations to the study.
Beyond gender and age characteristics, the NSMHWB does not allow us to determine characteristics of antidepressant users. In particular, we were unable to link the prescribing information to individuals with diagnosed affective and anxiety disorders. We were unable to ascertain the indication for which the medication was prescribed. The PBS data do not include prescriptions for which the averaged dispensed price is below the patient co-payment. The data on under co-payment and private scripts do not allow for gender or age stratification.
Antidepressant medication can be a valuable part of the treatment of affective and anxiety disorders, especially when psychological therapies are ineffective. It is important, however, that our service delivery system and the clinicians working in it facilitate the right treatment being provided to the right patients. This study suggests a significant mismatch between the population being treated for affective and anxiety disorders and the populations being prescribed the pharmacological treatments for these disorders. The design of the present study does not allow further conclusions to be drawn on the reasons for this but, taken in conjunction with other literature, it suggests that older Australians may be receiving antidepressant medications for reasons other than the treatment of conditions for which these drugs have marketing approval.
Footnotes
Acknowledgements
The prescribing data were provided by the Drug Utilisation Subcommittee, Pharmaceutical Benefits Branch, Australian Government Department of Health and Ageing. This study was funded from existing salaries and there were no conflicts of interest. We acknowledge the assistance of Mr Greg Merlo in the analysis of the prescribing data.