
Abstract
A challenge with universal school-based mental health supports is the limited understanding of potential unintended or unanticipated outcomes. In this review, we examined 47 academic and gray literature sources to address the question, “What are the side effects of universal school-based mental health supports?” We discuss how universal supports can positively impact student mental health, enhance school staff’s knowledge and attitudes in addressing mental health topics, and contribute to an improved school climate. However, universal supports can also lead to school staff feeling the strain of resource and time pressures from integrating mental health programming into demanding schedules, voicing frustrations about or exhibiting resistance to mental health supports, and encountering varied, unpredictable outcomes for different student populations across system contexts.
Nearly one in four young people between 9 and 12 years of age experience issues associated with poor mental health (Fusar-Poli et al., 2020; Mental Health Commission of Canada, 2013). Adolescence and early adulthood are critical periods in which poor mental health, if neglected, can precipitate life-long challenges (Hjorth et al., 2016; Lawrence et al., 2019; Smith et al., 2019). Without the appropriate support structures, students with diagnosable mental illnesses are often at an increased risk of dropping out of school and experiencing lower levels of academic achievement, poorer social outcomes, higher rates of unemployment, and increased risk of substance abuse (Doran & Kinchin, 2019; Larson et al., 2017; Mental Health Commission of Canada, 2013). It is not only those students with diagnosable mental health illnesses who experience such challenges; many other school-age children experience stressors and life circumstances that have deleterious effects on their mental health, with the recent impacts of COVID-19 only exacerbating this situation (Valliancourt et al., 2021).
Schools increasingly play a key role in fostering mental health through universal supports that aim to benefit all students (Kutcher & Wei, 2020). In Canada, schools are the most common place where young people receive mental health supports (Georgiades et al., 2019). However, researchers and professional associations have found that although educators recognize students’ mental health needs, a range of barriers and gaps persist in promoting students’ mental health (e.g., Shelemy et al., 2019). One of the most pressing of these is a limited understanding of side effects—the unanticipated or unintended outcomes of existing school-based mental health supports. As discussed later in this chapter, side effects can be positive, negative, or neutral, as perceived by those involved in and affected by educational supports. Understanding the possible side effects of various supports would enable educators and policymakers to make more informed implementation and evaluation decisions and provide a generative basis for future research into the systems and theories that shape mental health initiatives.
In this review, we explore the question, “What are the side effects of universal school-based mental health supports?” We answer this question by integrating scoping review and environmental scan methods, providing a comprehensive picture of the academic literature and policy- and practice-based insights.
Background
Youth Mental Health Defined
The terms “well-being,” “mental health,” and “mental illness” are often used interchangeably to describe an individual’s general mental health across education, health, and community organizations. The research reported here is primarily informed by two descriptions of mental health. The World Health Organization (2022) conceptualized mental health as “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community.”
Our second source definition of mental health is that provided by the Public Health Agency of Canada and restated by Alberta Education (2023), which described it as the capacity of each and all of us to feel, think, and act in ways that enhance our ability to enjoy life and deal with the challenges we face. It is a positive sense of emotional and spiritual well-being that respects the importance of culture, equity, social justice, interconnections, and personal dignity.
Although there are many other descriptions of mental health, we limited our references to those provided by these two well-known and widely used global and Canadian sources. Both definitions stress the positive aspects of mental health, including the knowledge, skills, and capacities to interact effectively with others and contribute to the environment. However, the reality is that not all individuals experience such a state. It is well established that many people suffer from poor mental health, often referred to as “mental illnesses” or “mental disorders” (the former associated with clinical diagnoses). Mental illnesses and disorders represent the most rapidly expanding categories of disease globally, affecting one in five children and one in two adults at some point in their lives (OECD, 2019a).
The COVID-19 pandemic further exacerbated the mental health crisis worldwide, as evidenced by increasing rates of anxiety, depression, and substance abuse (American Psychological Association, 2023). In terms of children and youth, Samji et al.’s (2022) review of 116 articles that examined the impacts of COVID-19 found a significant increase in mental health challenges, particularly for those with neurodiversities or chronic physical conditions. In addition to the personal, social, and economic costs of poor mental health, it is noteworthy that the World Health Organization (2021) identified suicide as the second leading cause of death among 15- to 29-year-olds globally, with rates especially high for vulnerable groups. The risks associated with poor mental health, such as suicidal behavior, are now widely seen as preventable through timely, evidence-based, and often low-cost mental health supports and early intervention efforts. To that end, education systems are uniquely positioned to address youth mental health through “enactment of modern governance practices, the cultivation of positive organizational climate and culture, and the system-wide implementation of multi-tiered promotion and early intervention practices” (Turner, 2022, p. 21).
School-Based Mental Health Supports
Numerous studies indicate that multitiered systems of support in schools can significantly mitigate the negative impacts of poor mental health (August et al., 2018; Fabiano & Evans, 2019). Such systems include tiers of increasing support intensity and complexity offered to children as needed (Table 1). At Tier 1, the universal tier, supports are provided to all students, focusing on mental health promotion and prevention. At Tier 2, the targeted tier, supports are provided to students at risk of poor mental health or who require additional mental health promotion support beyond that provided at the universal tier. Finally, at Tier 3, the individualized tier, students with identified mental health disorders or mental illness diagnoses are provided with specific interventions. Tier placement is guided by whole-school screenings, progress monitoring, and a student’s response to interventions. However, it is the continuum of supports across the three tiers that creates the conditions for every student to be successful in their learning, ensuring schools can “meet students where they are and tailor interventions to the current needs related to skill-building and problem reduction” (Fabiano & Evans, 2019, p. 1).
Multitiered Systems of Support
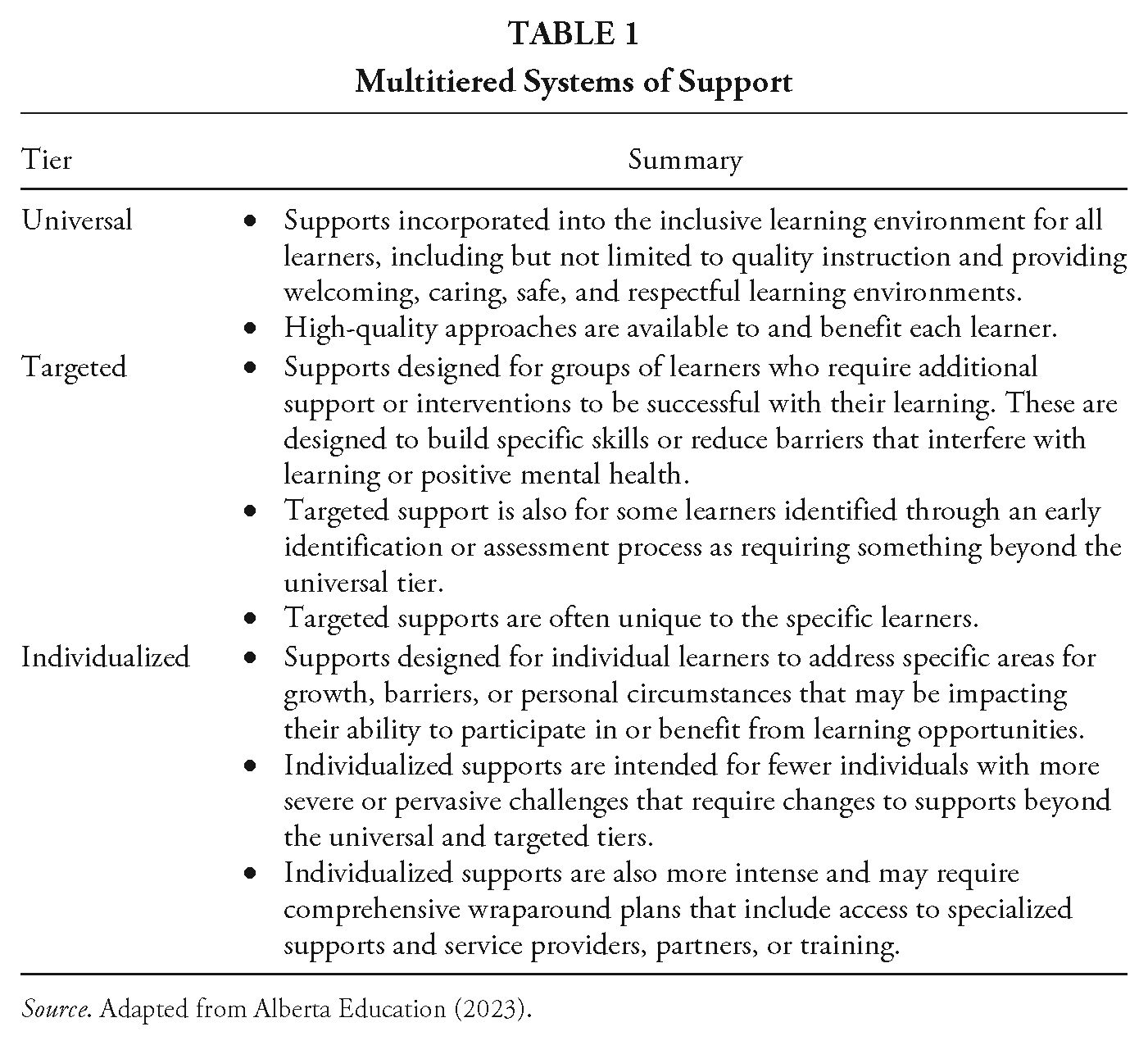
Source. Adapted from Alberta Education (2023).
Whereas targeted and individualized supports for student mental health have received considerable research attention to inform the implementation and evaluation efforts (e.g., Dix et al., 2020), the universal tier remains a challenge for many education systems (e.g., Procter et al., 2021; Punukollu et al., 2020). Universal supports remain a new area of practice and policy in many systems, meaning that resource allocation, including skilled personnel, time, and organizational infrastructure, needs to be more informed by existing evidence. Moreover, despite the intent of the universal tier, cultural, language, and socioeconomic barriers may impede some students and families from fully benefiting from available supports. For instance, even with universal supports in place, the stigma around mental health topics can persist, potentially deterring students from seeking help (Bulanda et al., 2014; Morrison & Peterson, 2016). Finally, universal tier supports must be flexible and adaptable to the needs of diverse student populations, which may be challenging given the systemic constraints schools often face. These challenges underscore the need to understand the outcomes of universal school-based mental health supports, particularly those unintended or unanticipated.
Conceptual Framework
Our analysis of the academic and gray literature was informed by a bespoke conceptual framework designed to chart the main effects and side effects of school-based mental health supports. Specifically, based on an ongoing research project investigating the evaluation of such supports, we integrated recent research into implementation science and educational outcomes.
Implementation Drivers
To map the proposed impacts of mental health supports, we drew on the extensive research by Dean Fixsen and Karen Blase into “implementation drivers.” In brief, implementation drivers represent how support efforts (e.g., programs, reforms, interventions) aim to achieve the intended impacts (Sims & Melcher, 2017). As detailed by Fixsen et al. (2015), there are three categories of implementation drivers: 1. Competency Drivers [coaching, training, staff selection and recruitment] – are mechanisms to develop, improve and sustain one’s ability to implement an intervention as intended in order to benefit children, families and communities. 2. Organization Drivers [systems intervention, facilitative administration, data systems] – are mechanisms to create and sustain hospitable organizational and system environments for effective services. 3. Leadership Driver [technical or adaptive] – focuses on providing the right leadership strategies for the types of leadership challenges. These leadership challenges often emerge as part of the change management process needed to make decisions, provide guidance, and support organization functioning. (p. 2)
Combined, these drivers can induce the systems and processes needed to implement and sustain an initiative successfully. In our review, these implementation drivers provided a means for conceptualizing how the impacts of school-based mental health supports, disaggregated into main effects and side effects, were thought to follow from specific combinations of competency, organization, and leadership drivers.
Educational Outcomes: Distinguishing Between Main Effects and Side Effects
Zhao (2017) contended that “considering both main and side effects can help resolve artificially divisive issues in education and help advance the field” (p. 13). Even a cursory examination of the various educational initiatives implemented in recent years (e.g., the No Child Left Behind Act, direct instruction, school vouchers; see Zhao, 2018) reveals that it can be unproductive and potentially misleading to adopt a myopic focus on main effects—a perspective long known and appreciated in other sectors (e.g., in many health disciplines).
In this chapter, we distinguish between main and side effects we noticed in our review of the research on school-based mental health. Main effects refer to the outcomes of an educational initiative that follow from its underlying theory or logic. Main effects represent outcomes anticipated to emerge from relationships among the variables or phenomena of focus in an intervention, either positive, negative, or neutral. In other words, main effects are those that are anticipated and/or expected.
Side effects, on the other hand, have typically been thought of as the unwanted outcomes accompanying an initiative’s main effects. Zhao (2017) suggested three reasons they tend to receive less research attention than main effects: (a) the outcomes of education interventions, particularly those unintended or unanticipated, may emerge over longer time horizons than considered in many research projects; (b) narrow definitions of “outcomes” in education research, which make it difficult to not only observe possible side effects but also to draw together the findings from various studies; and (c) “political, commercial, or other reasons to deliberately overlook side effects” (Zhao, 2017, p. 4). Notwithstanding these challenges with studying side effects, manifold factors contribute to their emergence in implementation efforts, including resource limitations, inherently contradictory aims among some initiatives, and differential functioning of implementation drivers in various contexts (Zhao, 2018). It is also important to consider that side effects are not exclusively negative, particularly in light of the diverse educational side effects discussed in this volume of Review of Research in Education. As defined earlier in this chapter, side effects represent unintended or unanticipated outcomes, which means they can be positive, negative, or neutral, as perceived by those involved in and affected by educational initiatives. In this way, main effects and side effects are two sides of the same coin; any initiative can—and likely will—produce both in varying amounts and intensities depending on the relevant sociocultural and historical contexts.
Combining Implementation Drivers With Educational Outcomes
The conceptual framework for this review integrated Fixsen et al.’s (2015) implementation drivers with the works of Zhao (2017, 2018) and Rigney and Zhao (2022), which encourage an understanding of the main effects and side effects of educational supports as emerging over the short and long terms. In applying this framework, we were careful not to draw distinct lines between the context of any support efforts and the implementation drivers and outcomes described, as might be done in a realist analysis (e.g., Haynes et al., 2018). Analyses of this sort for youth mental health are elsewhere available (e.g., Clarke et al., 2021; Procter et al., 2021). Instead, we focused on disentangling the main effects from side effects while also understanding how those exist against the backdrop of implementation efforts prominent in contemporary academic and gray literature.
Methods
To examine the extant academic and gray literature, we utilized a two-pronged approach that combined scoping review and environmental scan methods. Figure 1 summarizes the processes and results.
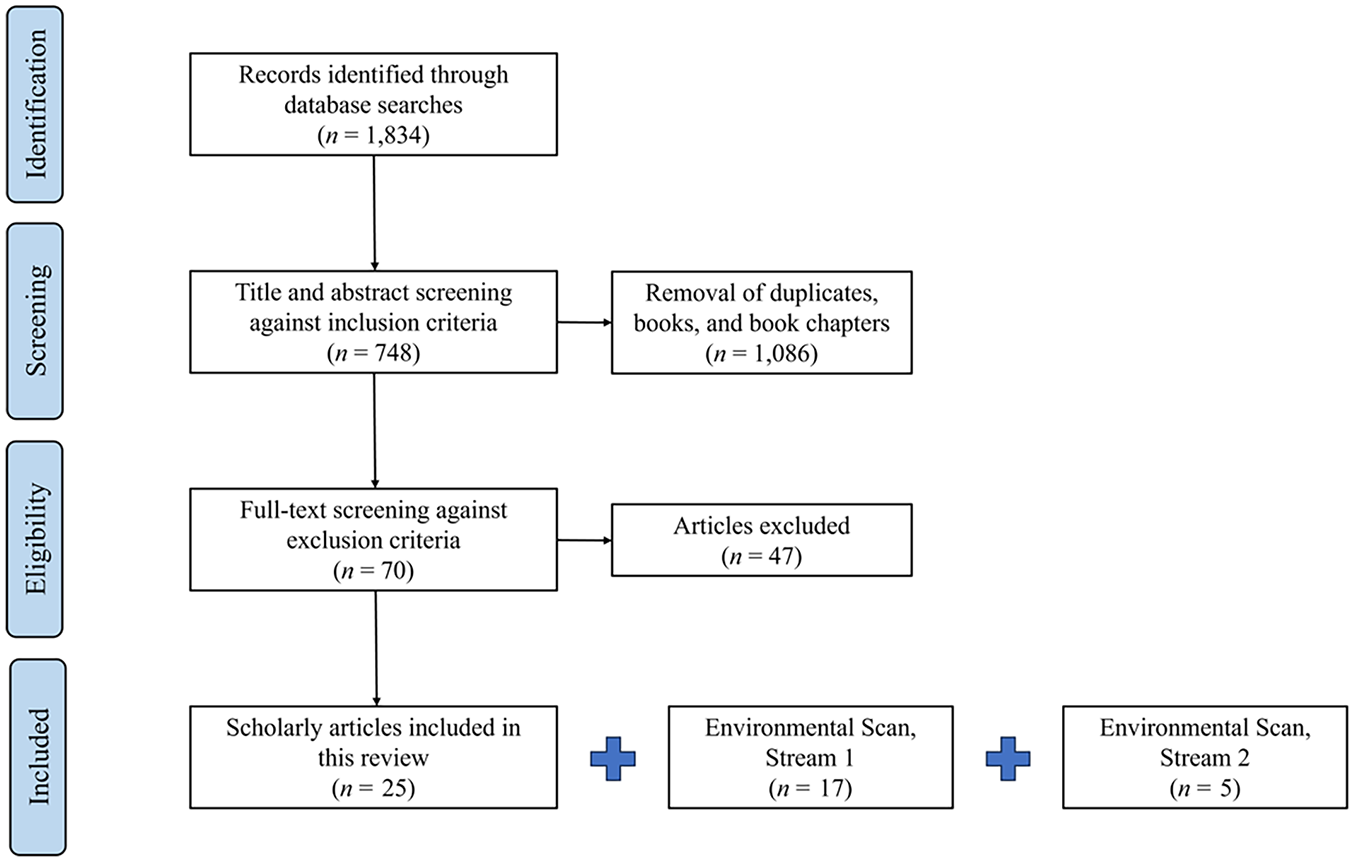
PRISMA Diagram
Scoping Review
The first prong was a scoping review, which provided the methods “to examine the extent, range and nature of research activity . . . [offering] a useful way of mapping fields of study where it is difficult to visualize the range of material that might be available” (Arksey & O’Malley, 2005, p. 21). Such a review is a salient starting point given the burgeoning study of mental health promotion in schools (e.g., Hoover & Bostic, 2021; Marsh & Mathur, 2020; O’Malley et al., 2018) yet the limited previous work synthesizing the available evidence about possible side effects. Four stages framed the review. We began by identifying potentially relevant literature using keyword search strings entered into electronic databases, ensuring search sensitivity (i.e., the ability to retrieve relevant material; McKibbon et al., 2012) by using multiple general terms. Similar to other scoping studies (e.g., Mallidou et al., 2018), searches targeted titles and abstracts. Each search string included a mental health term that was used in both the World Health Organization and Public Health Agency of Canada’s definitions that informed this research (mental health, well-being, or wellness), a term to denote school-based supports (classroom or school), and a term to signify evaluation (evaluation, indicator, metric, measure, or assessment). Electronic databases included Academic Search Complete, CINAHL, Education Source, ERIC, Proquest, Scopus, and Web of Science. Search limits included language (English only), publication type (peer-reviewed academic journal articles), and publication date (January 2010–January 2023).
All identified sources (n = 1,834) were uploaded into Endnote X9.3.3 to remove duplicates, books, and book chapters before subsequent upload into the online systematic review platform Covidence. Two independent reviewers then screened titles and abstracts according to two general inclusion criteria (n = 748): (a) The source corresponded to a theoretical or empirical journal article, and (b) the concepts of mental health and school-based supports were examined or discussed. The same two reviewers then analyzed full-text articles for eligibility in the review (n = 70) against the following exclusion criteria: (a) postsecondary focus, (b) published before 2010, (c) not published in English, (d) did not address school-based mental health supports, and (e) addressed supports at the targeted or individualized tiers rather than the universal tier. A third reviewer resolved any reviewer discrepancies in either title and abstract screening or eligibility analysis. A total of 25 academic articles were found eligible for inclusion in the review.
Environmental Scan
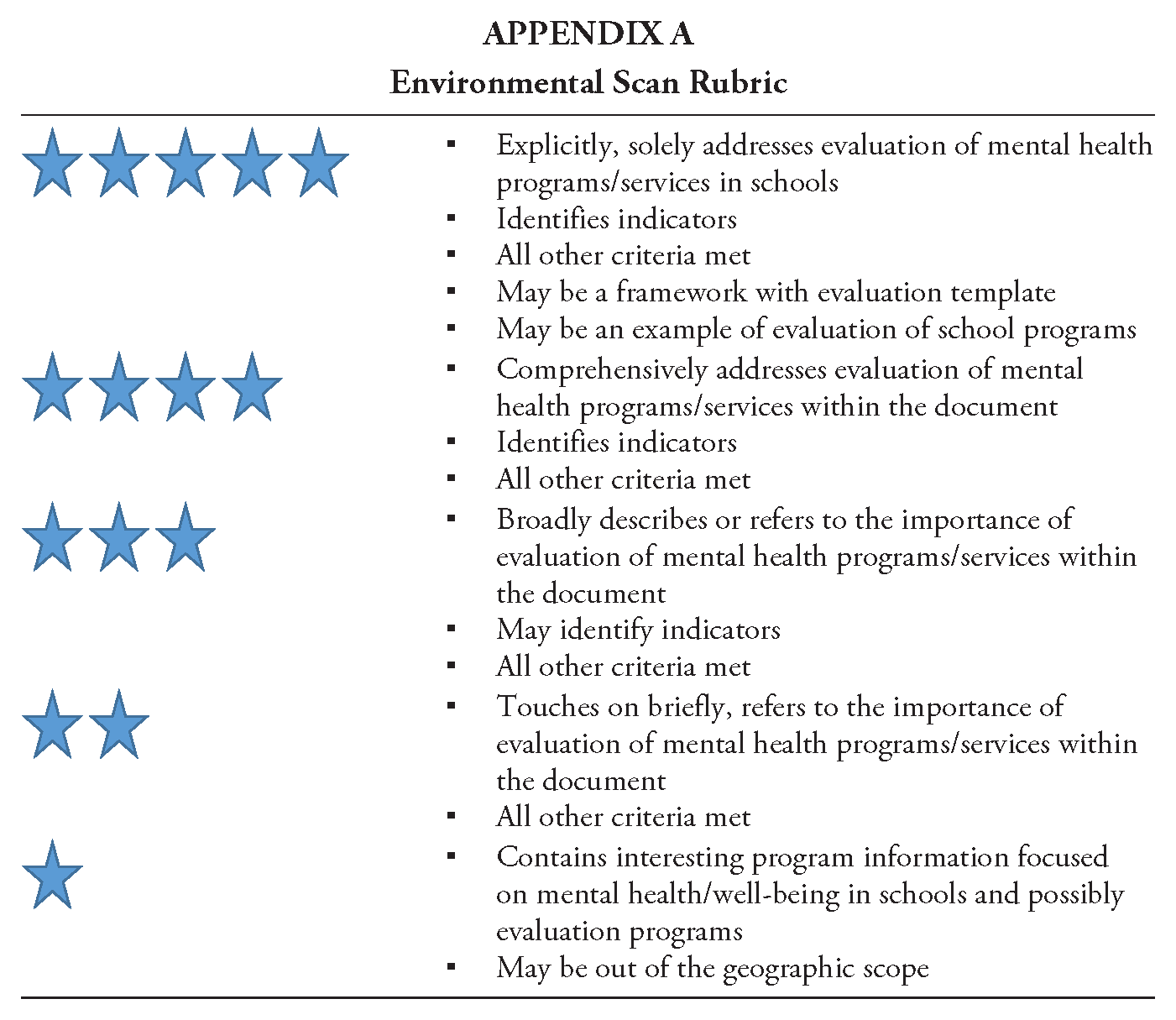
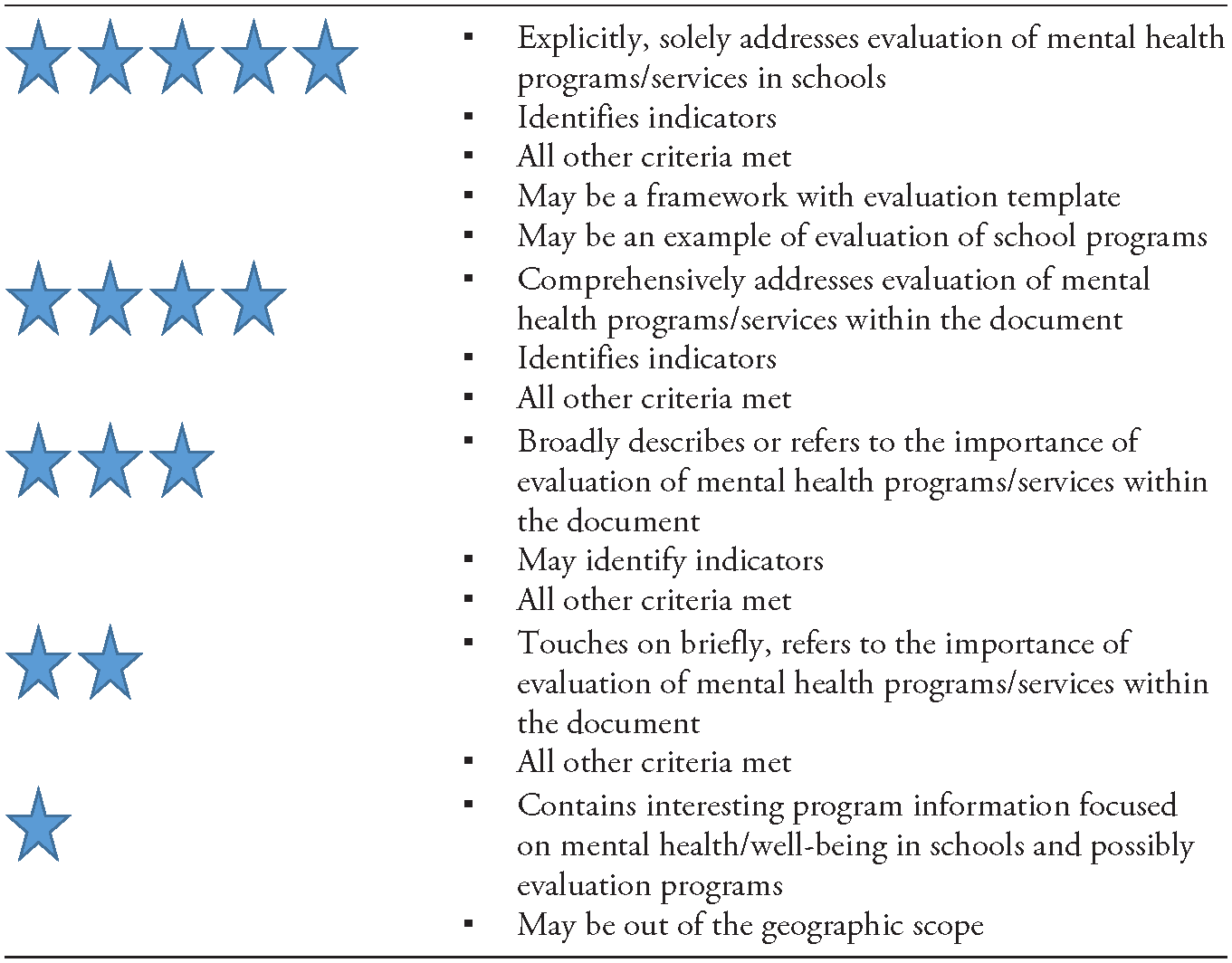
The second prong was an environmental scan of gray literature (e.g., evaluation toolkits, policy briefs) about universal supports to promote student mental health in schools. The purposes of environmental scans are “to learn about events and trends in external environments; establish relationships between them; make sense of the data; [and] extract the main implication[s] for decision making and strategy development” (Costa, 1995, p. 5). Hence, an environmental scan was well suited for understanding the nature and prevalence of education side effects as well as “opportunities, challenges, and likely future developments” (Conway, 2009, p. 2). Data collection involved a two-stream search and review strategy. In the first stream, the same keyword search strings and limiters used in the scoping review were applied to the Google Search Engine. The website of each search result was investigated in-depth for any content relevant to the evaluation of school-based mental health supports. However, given the increasing likelihood of off-target content in later pages of each Google search, only the first five pages were examined. In the second stream, the search was repeated with a specific focus on OECD countries by including geographic identifiers (e.g., Canada, United States, United Kingdom, New Zealand, Australia). Our focus on OECD countries was chosen due to their comparable levels of economic and social development, facilitating meaningful interpretations across educational contexts. In instances where the two searches returned multiple relevant resources for the same support efforts, we referenced just one here but considered all identified in the analysis of implementation drivers and educational outcomes. All identified sources were screened against an inclusion rubric (see Appendix A). Ultimately, the two searches led to the inclusion of 17 and five sources, respectively.
We applied a charting template to the complete data set of 47 academic and gray literature sources, focusing on contextual information (e.g., publication date, country of study, participants) and our conceptual framework’s implementation and education outcomes dimensions. The process of identifying and categorizing outcomes involved a collaborative and in-depth examination of each source by multiple authors in which we devoted attention to “the frequency and saliency of particular words or phrases in a body of original text data in order to identify keywords or repeated ideas” (Namey et al., 2008). Our team systematically discussed and iteratively refined the categorization of main effects and side effects identified in the literature. This method allowed us to capture a diverse range of perspectives and to ensure the accuracy and relevance of our categorizations. Table 2 displays all included sources.
Contextual Details of Included Literature
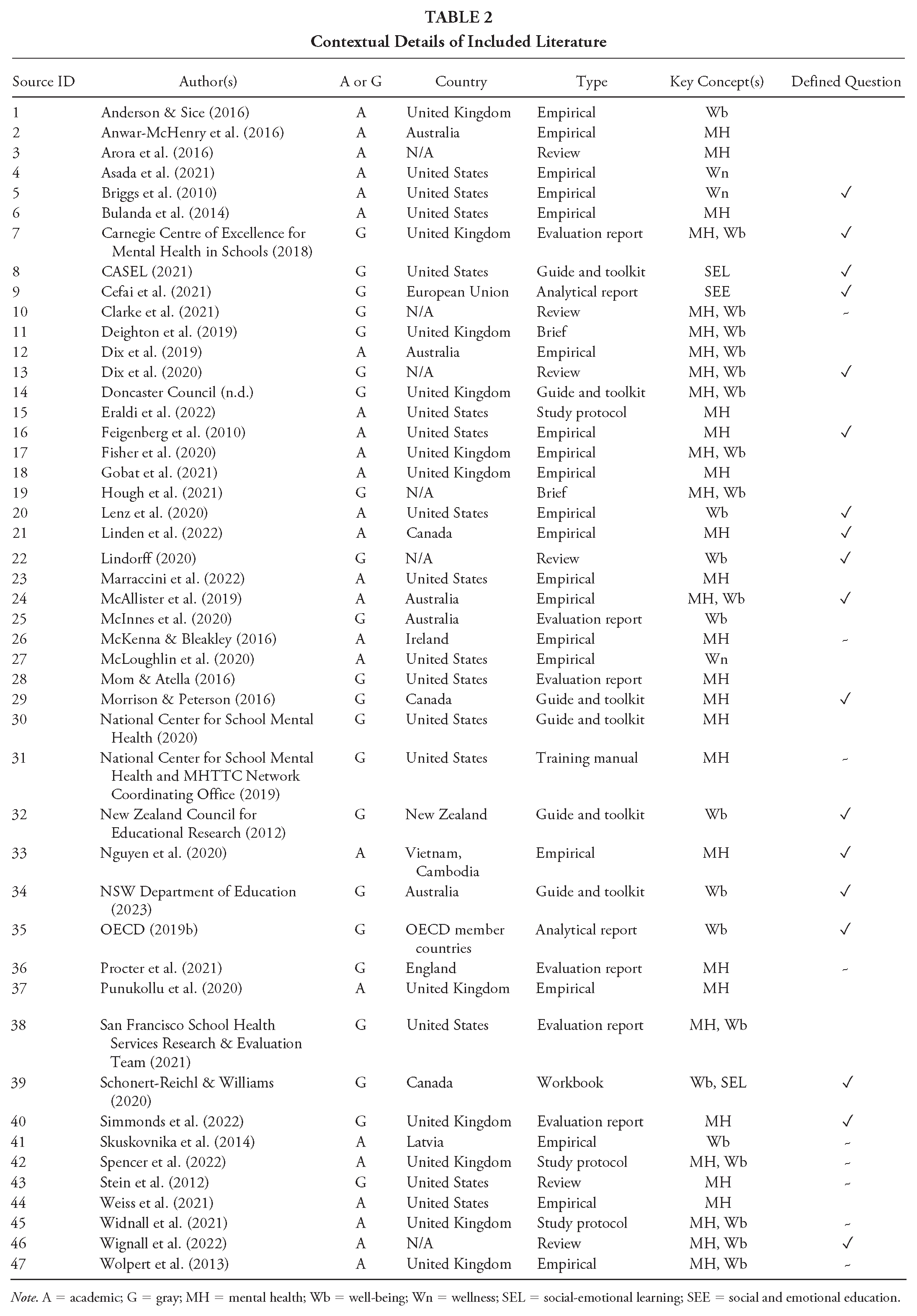
Note. A = academic; G = gray; MH = mental health; Wb = well-being; Wn = wellness; SEL = social-emotional learning; SEE = social and emotional education.
Findings
We organize the findings of this review in three sections. The first section presents a number of contextual details for the included sources, including the first dimension of our conceptual framework: implementation drivers. The second and third sections present the main effects and side effects of universal school-based mental health support, representing the second dimension of our conceptual framework. Per the research question guiding this review, we devote primary focus to the topic of side effects. Although we intended to disaggregate each effects section by those occurring in the short term and long terms, only one article discussed what might be considered long-term effects (McAllister et al., 2019), and so our presentation of the findings does not include this component.
Contextual Details
Beginning with publication date, we observed a clear trend of increasing interest in the topic of evaluating school-based mental health supports. Specifically, seven sources were included from 2010 to 2014, eight from 2015 to 2018, and 31 from 2019 to 2021. Regarding the country of focus, the United States (n = 15) and the United Kingdom (n = 12) accounted for 57% of included sources. Those remaining indicated focal contexts of Australia (n = 5), Canada (n = 3), and various other individual or groupings of countries (e.g., OECD member countries). Source type was another point of analysis. Most sources were empirical (n = 20), followed by reviews (n = 6), evaluation reports (n = 6), guides and toolkits (n = 6), study protocols (n = 3), analytical reports (n = 2), briefs (n = 2), a workbook, and a training manual. Among the sources, we also observed considerable diversity in the key concepts employed, including mental health (n = 19), mental health and well-being (n = 14), well-being (n = 8), wellness (n = 3), and other comparatively uncommon concepts (e.g., social-emotional learning). Unexpectedly, only 18 sources defined the key concepts used, and an additional nine sources provided generic descriptions.
For the purposes of analyzing the main effects and side effects of school-based mental health supports, we consider only the subset of empirical articles and evaluation reports (Table 3). Among this subset, there was considerable diversity in how outcomes were evaluated. The most common approaches involved mixed methods (n = 6), pretest/posttest designs (n = 4), or process evaluation (n = 3). Additionally, quantitative and qualitative methods were nearly of similar prevalence (n = 21 and n = 17, respectively).
Methodological and Implementation Details of Included Empirical Articles and Evaluation Reports (n = 26)
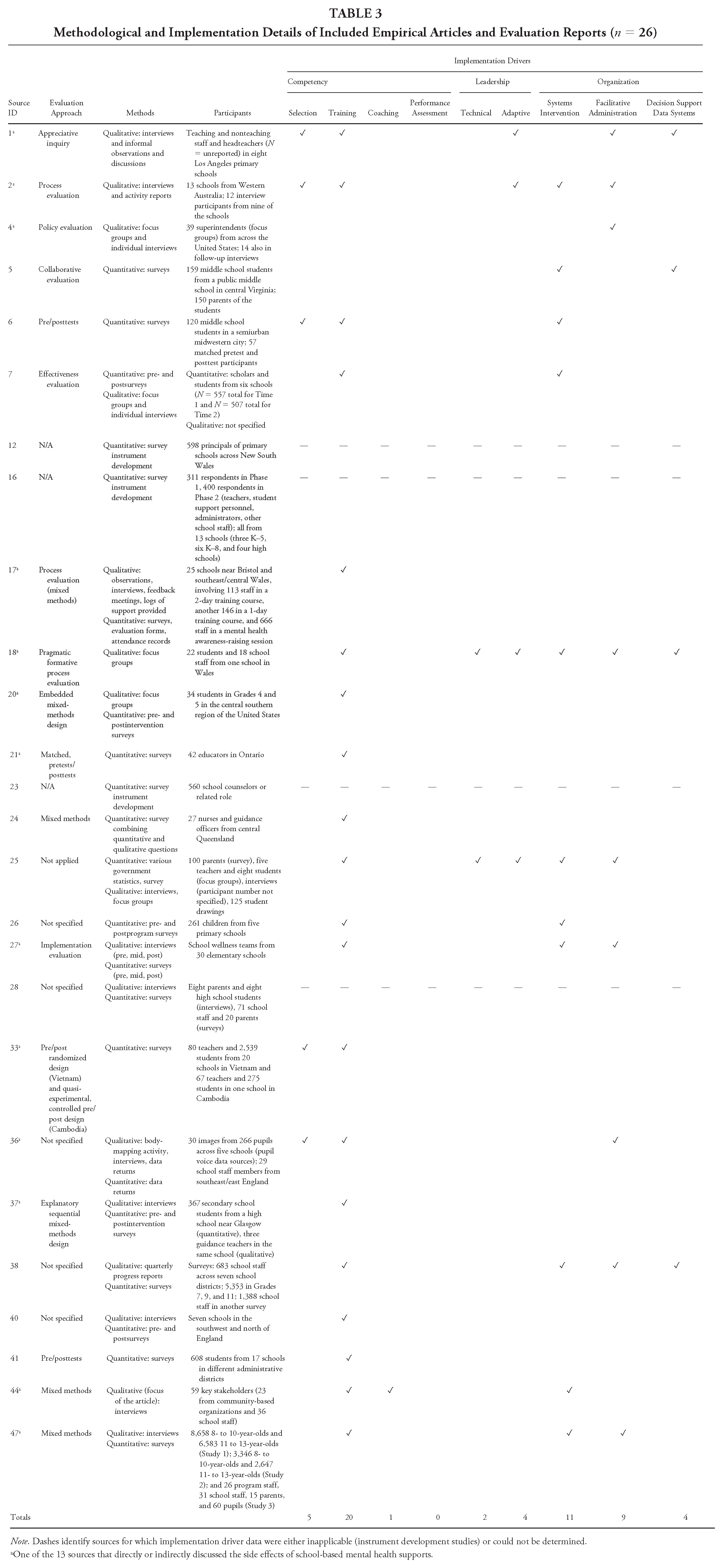
Note. Dashes identify sources for which implementation driver data were either inapplicable (instrument development studies) or could not be determined.
One of the 13 sources that directly or indirectly discussed the side effects of school-based mental health supports.
Turning to the first dimension of our conceptual framework, we examined the explicit mention of implementation drivers. Competency drivers were the most common category (n = 26), present in all but two sources. Within this category, the primary approach to driving the implementation of school-based mental health supports was to provide training (n = 20) for either school staff or students to learn about when, where, and with whom to use various practices and support strategies. It was comparatively less common for support efforts to recruit staff with specialized skills (n = 5), provide coaching supports (n = 1), or conduct performance assessments of staff training, recruitment, and coaching efforts (n = 0). Organization drivers were the second most common category (n = 24), mentioned in all but eight sources. Among these, interventions that enabled schools to better interact with external systems (e.g., through formalizing relationships with community partners) were the primary approach to driving implementation efforts (n = 11). Facilitative administrative supports were nearly as prevalent (n = 9), which represented efforts to align school policies, procedures, structures, culture, and climate with the mental health needs of students and school staff (e.g., by developing school mental health teams). In contrast, decision support data systems were seldom mentioned in the included sources (n = 4), meaning it was unclear whether many supports were informed by data collection, analysis, and reporting to enable continuous improvement. The final and least commonly mentioned category was leadership drivers (n = 6), present in only four sources and encompassing both adaptive (e.g., establishing communication channels for school staff to voice successes and concerns) and technical (e.g., ensuring clarity on the details of new initiatives) approaches to leadership (n = 4 and n = 2, respectively).
Main Effects
In our analysis of the 26 articles that discussed the main effects of school-based mental health supports, we identified three overarching categories. These categories are summarized in the following, incorporating a selection of citations from the overall data set.
Positive Impacts on Student Mental Health
The most common category of main effects for universal school-based mental health supports concerned the positive impacts on student mental health (e.g., Asada et al., 2021; Lenz et al., 2020; McKenna & Bleakley, 2016; Mom & Atella, 2016; Nguyen et al., 2020; Punukollu et al., 2020; Simmonds et al., 2022; Skuskovnika et al., 2014). Specifically, supports were found to promote the development of mental health literacy (e.g., Carnegie Centre of Excellence for Mental Health in Schools, 2018), instill a deeper understanding of mental health concepts across diverse student groups (e.g., McKenna & Bleakley, 2016), and improve emotional expression, self-discovery, and empathy among students (e.g., Lenz et al., 2020). Moreover, universal mental health supports contributed to higher engagement in class, stronger connection to the school community, and improved academic performance (e.g., Mom & Atella, 2016).
Enhanced Knowledge and Attitudes
A second category of main effects highlighted that universal school-based mental health supports can enhance school staff’s knowledge and attitudes about mental health topics (e.g., Bulanda et al., 2014; Linden et al., 2022; McAllister et al., 2019; McLoughlin et al., 2020; Punukollu et al., 2020; Weiss et al., 2021). Linden et al.’s (2022) evaluation of the “Bell Let’s Talk in the Classroom Guide,” for example, found that not only did teachers’ confidence in delivering mental health content improve, but also their worries about mental health conversations in the classroom decreased (e.g., thoughtfully addressing the topics of emotion and empathy; McKenna & Bleakley, 2016). Other specific influences included empowering school staff to believe they can effectively promote student mental health (e.g., McAllister et al., 2019), fostering open discussion and destigmatization of mental health topics (e.g., Mom & Atella, 2016; Punukollu et al., 2020), and heightening staff sensitivity to the social and emotional challenges that students encounter (Weiss et al., 2021).
Improved Schoolwide Climate
The third and final category of main effects was an improved schoolwide climate through fostering inclusive, positive learning environments (e.g., Anderson & Sice, 2016; Asada et al., 2021; Dix et al., 2019; McInnes et al., 2020). Included sources found that universal mental health supports could encourage, among both school staff and students, improved collaboration and the diminution of barriers to productive exchanges (e.g., Anderson & Sice, 2016; Skuskovnika et al., 2014), promote the advancement of policies and practices that prioritize student mental health (e.g., Dix et al., 2019), and create the conditions to foster more positive relationships and learning outcomes (McInnes et al., 2020).
Side Effects
A total of 12 academic articles and one gray literature source directly or indirectly discussed the side effects of school-based mental health supports (see Table 3). Three categories crystalized in our analysis of these sources, detailed in the following in order of apparent prevalence.
The Strain of Resource and Time Pressures
The most frequently discussed side effect was that of school staff feeling the strain of resource and time pressures resulting from the integration of mental health programming into already demanding school schedules (e.g., Anwar-McHenry et al., 2016; Fisher et al., 2020; Linden et al., 2022; McLoughlin et al., 2020; Nguyen et al., 2020; Punukollu et al., 2020; Weiss et al., 2021). Resource pressures were most acutely felt in terms of insufficient training to adequately support students’ mental health needs (e.g., teachers experiencing concerns about “doing something wrong”; see Procter et al., 2021, p. 43), challenges due to lacking supports for integrating new practices with existing curriculum materials (e.g., Nguyen et al., 2020), and the misalignment of support efforts with existing policies and guidelines (e.g., Anwar-McHenry et al., 2016). Time pressures included the need to adapt content in order to make it accessible for students (e.g., Punukollu et al., 2020) and the need to take time away from other instructional topics due to supports being poorly integrated with existing structures and processes (e.g., Fisher et al., 2020; Weiss et al., 2021). A clear representation of these side effects was encapsulated by Punukollu et al. (2020) in their description of teachers’ experiences with an initiative that combined peer support and mobile application efforts to promote student mental health: Teachers felt pressurized to juggle several roles, including lesson delivery, supporting academic success and supporting pupil mental health. Therefore, although it was a benefit that the programme prompted help-seeking, teachers felt they did not have adequate time, supervision or training to adequately support pupils with mental health difficulties. (p. 515)
Another way the strain of resource and time pressures emerged was the balance of flexibility and fidelity in implementing new schoolwide supports. An example of this challenge can be seen in Fisher et al.’s (2020) evaluation of the uptake of a mental health first aid training package. Although trainers for the initiative recognized the need for flexibility in its delivery to school staff due to factors such as timetabling, Fisher et al. noted that this meant “in some schools insufficient numbers of staff received MHFA [mental health first aid] training and extent of delivery of the peer support service compromised intervention dose and reach” (p. 10). Similarly, other sources discussed how, despite the apparent desirability of flexibility in engaging with new support efforts, the lack of structure could result in fewer school staff participating or the number of participants decreasing over time (e.g., Linden et al., 2022).
Mixed Attitudes and Commitment
Another common side effect was for school staff to voice frustrations about or exhibit resistance to mental health supports, particularly when there existed conflicting views on the importance of mental health to academic goals or when teachers felt constrained due to various contextual circumstances (e.g., Anderson & Sice, 2016; Anwar-McHenry et al., 2016; Asada et al., 2021; McLoughlin et al., 2020; Punukollu et al., 2020; Weiss et al., 2021). The potential for mental health supports to engender mixed attitudes from school staff was perhaps best represented in Weiss et al.’s (2021) evaluation of an initiative that aimed to shift acute mental health supports from hospital settings to community settings, involving 92 New York City middle and high schools: “Teachers valued their educator roles and responsibilities and recognized that they, and their schools, are assessed by regulators and parents on specific academic indicators. Therefore, they were wary of taking time away from teaching to focus on mental health” (p. 433). Similarly, Gobat et al.’s (2021) evaluation of a whole-school restorative approach to improving student mental health addressed how the implementation of new initiatives could run counter to existing sociocultural contexts (e.g., school policies), which could contribute to school staff becoming discontented with change efforts more generally. At the same time, several sources found that mental health supports can generate positive outcomes that might be unexpected given the underlying program theory, such as building momentum in mental health promotion beyond the initial efforts (e.g., Anderson & Sice, 2016) and spurring the development of community partnerships (Anwar-McHenry et al., 2016).
Variable Program Effectiveness and Impact
The third category of side effects represents the variable effectiveness and impact for universal mental health supports. Specifically, several sources discussed that although support efforts were successful in achieving intended outcomes in the aggregate (e.g., overall improvements in students’ self-reported ability to engage in emotional expression), those outcomes could take on a varied, unpredictable nature for different student populations and in different system contexts (e.g., Gobat et al., 2021; Lenz et al., 2020; Nguyen et al., 2020; Wolpert et al., 2013). Such variability was observed in Wolpert et al.’s (2013) evaluation of the Targeted Mental Health in Schools program in England. Although positive impacts were observed for all groups of students, one component of the program (self-help information booklets) “was associated with deterioration in well-being for children with emotional problems in the context of staff having received action learning sets” (p. 281). Another example of variable program effectiveness was observed in Gobat et al.’s (2021) process evaluation. Despite the universal mental health supports improving the participating school’s reputation in the local community, this reputation boost was also felt as a burden due to oversubscription.
Discussion
What can we make of the various main effects and side effects of universal school-based mental health supports uncovered in this review? Similar to others who have focused primarily on main effects, our general impression of the existing evidence is that although there are challenges to implementing and evaluating universal supports, the outcomes are overwhelmingly positive. The sources included in this review discussed how universal supports can positively impact student mental health, enhance school staff’s knowledge and attitudes in addressing mental health topics, and contribute to an improved school climate. However, such main effects tell only part of the story. Considered alongside the implementation drivers and side effects examined here, we can draw several overarching interpretations of the findings.
First, although it is the combination of implementation drivers (competency, organization, and leadership) that creates the conditions for successful change efforts (Sims & Melcher, 2017), we observed few descriptions of universal supports that made use of more than three: 2.5 was the average. That the competency driver of training was the most common is, to some extent, reassuring, considering prior reviews have noted its importance for ensuring teachers have the skills and confidence to support student mental health (e.g., Clarke et al., 2021). However, other competency drivers were concerningly absent, particularly coaching and performance assessment. The former is essential for providing “‘craft’ information along with advice, encouragement, and opportunities to practice and use skills specific to the innovation” (Fixsen et al., 2015, p. 12), going beyond the initial learning made possible through training. We question whether some of the negative side effects observed in this review, particularly the challenges school staff encounter regarding the balance between fidelity and flexibility in implementing support efforts, might be mitigated by greater attention to coaching, as intimated in some practice-focused resources (e.g., Cefai et al., 2021; National Center for School Mental Health & MHTTC Network Coordinating Office, 2019). Relatedly, when conducted with formative intent, performance assessment ensures that the other competency drivers can be consistently modified to meet school staff’s professional learning needs related to universal supports. Such adjustments may be a potent mechanism for assuaging some school staff’s concerns about how mental health initiatives can augment academic goals.
We observed similar gaps in the organization and leadership drivers mentioned in the included sources. Although it is certainly possible these drivers were present in some initiatives but not described, this situation would nonetheless be cause for concern. That is, to omit the critical role of leadership and organizational drivers of change (e.g., see Procter et al., 2021) is to seemingly accept the increased likelihood of negative side effects, such as those related to strain of resource and time pressures.
A second insight we stress based on the findings from this review is that the side effects of universal mental health supports are not simplistically negative or positive. Although these supports can provide crucial aid for students struggling with mental health issues, especially when integrated with targeted and individualized supports, they may also inadvertently generate negative outcomes among some school staff and students. Furthermore, the effectiveness of universal supports can vary significantly based on student needs, the competence and cultural sensitivity of the staff implementing the supports, and the broader school environment. And yet, it is important to underscore that our understanding of these dynamics is still developing. Further research is needed to fully comprehend the multifaceted outcomes of universal mental health supports in schools, optimize their benefits, and mitigate any unintended adverse effects.
Limitations
Several limitations should be considered alongside the findings of this review. First, the exploratory design of our review may have introduced bias due to the wide range of sources included, leading to an overrepresentation of certain perspectives or methodologies. As an example, in our analysis of implementation drivers, only the competency, organization, or leadership drivers explicitly mentioned in each source were captured by our analysis. For empirical studies that investigated general efforts to promote mental health in schools rather than specific supports (e.g., Asada et al.’s [2021] study of superintendents’ perceptions of and experiences with policy implementation), our approach may have missed implementation drivers that were unique to some study contexts and thus were not explicitly mentioned. Second, as is common with scoping reviews and environmental scans, the quality of the included sources was not appraised, which could potentially impact the reliability of the findings. Although the purpose of such reviews is to provide a broad overview of the existing literature, the lack of quality assessment means that the results of both high-quality and lower quality studies were considered equally. Third, our literature search may not have captured all relevant studies despite our efforts to conduct a comprehensive search across multiple databases. There may be relevant gray literature, such as dissertations or conference proceedings, that was missed. Articles not written in English were also excluded, which could contribute to language bias. Lastly, due to the broad nature of a scoping review, the depth of analysis is inherently limited. The large number of studies included in this review allowed for a wide-ranging overview of the topic, but it also limited our ability to deeply analyze the results of each study. Future systematic reviews or meta-analyses could address some limitations by conducting a more focused analysis of a narrower set of high-quality studies.
Footnotes
Appendix
Environmental Scan Rubric
|