
Abstract
Background:
Rathke’s cleft cysts (RCCs) are benign sellar and suprasellar lesions. Most are treated conservatively, while others require surgery, usually via a transsphenoidal intervention. However, long-term outcomes of surgical intervention remain challenged by the risk of cyst recurrence, which can manifest years after initial treatment. We aim to assess the long-term outcomes of RCCs and predictors of recurrence post endoscopic endonasal resection.
Methods:
We reviewed our database for the last 10 years (2014–2024). We included all the patients with Rathke’s Cleft Cysts who underwent Endoscopic Endonasal Transsphenoidal (EET) surgery. Demographic data, preoperative, intraoperative, postoperative clinical data and patients’ outcomes were retrospectively collected and analyzed.
Results:
Thirty RCC patients who underwent transsphenoidal surgery were included in this study. The mean age of our cohort was 54.6 years, and 59% were females. Four patients developed cerebrospinal fluid (CSF) leak postoperatively (13.33%), and four patients (13.33%) had permanent diabetes insipidus (DI). During follow-up, recurrence was observed in 16.67% (5 patients) with an average latency of 23 months. Only three patients were symptomatic and required re-operation.
Conclusions:
Following transsphenoidal surgery for Rathke’s cleft cysts, many patients experienced rapid improvement of symptoms. Moreover, recurrence is influenced by numerous factors requiring long-term follow-up. Future studies with larger sample sizes and longer follow-up durations are recommended.
1 Introduction
Rathke’s Cleft Cyst (RCC) is the most common benign, sellar lesion following pituitary adenoma (1, 2). It originates from an embryological remnant of Rathke’s cleft which normally regresses by adulthood. However, failure to regress leads to formation of an epithelial lined, hormone secreting cyst (3, 4). RCC is often an incidental finding during routine autopsy or when Magnetic Resonance Imaging (MRI) is performed for unrelated conditions (2, 5–8). This type of lesion can occur in the sellar, suprasellar, parasellar, or intrasellar locations; in addition, it can also show suprasellar extension. Cysts can be filled with Cerebro Spinal Fluid (CSF) like fluid, mucoid, or gelatinous material (7–9). Accurate differentiation of RCC from other sellar pathologies is essential due to overlapping clinical and radiographic features. MRI is the preferred imaging modality, with intracystic nodules being a key distinguishing feature of RCC. In order to confirm the diagnosis Computed Tomography (CT) scan and histopathological confirmation are often needed (3, 5, 7).
Asymptomatic cases are managed conservatively with observation (2, 5–8). However, cysts can grow in size exerting mass effect on adjacent structures such as the pituitary gland, infundibulum, optic chiasma, or hypothalamus. Symptoms include headaches, visual disturbances, and endocrinopathies (7, 10–14). Symptomatic RCCs are less common and typically present during the fourth or fifth decade of life, with a female predominance (10, 15). The preferred intervention is Endoscopic Endonasal Transsphenoidal (EET) surgery which has been widely used for the past 35 years, and offers favourable outcomes, lower mortality and recurrence rates compared to other surgical approaches (16, 17).
This aim of the present study is to evaluate the recurrence rate and long-term outcomes in patients with RCC who were treated surgically by EET approach.
2 Methodology
We conducted a retrospective study of 30 patients with confirmed diagnosis of RCC who underwent surgical treatment after obtaining approval from the institutional review board at the Ottawa Hospital Civic Campus, between June 2014 and April 2024.
Demographic characteristics, American Society of Anesthesiologists (ASA) Physical Status, radiological data including MRI finding (Figure 1), endocrinological, and ophthalmic assessment, were extracted from patients’ medical records. Intraoperative measures such as histopathological analysis of cyst, surgical time, blood loss, intraoperative Mean Arterial Pressure (MAP), use of lumbar drain, dural sealants, or nasoseptal flaps, and complications. In addition to Length of Stay (LOS), readmission at 30 and 90 days, and postoperative complications were also reviewed and analysed.
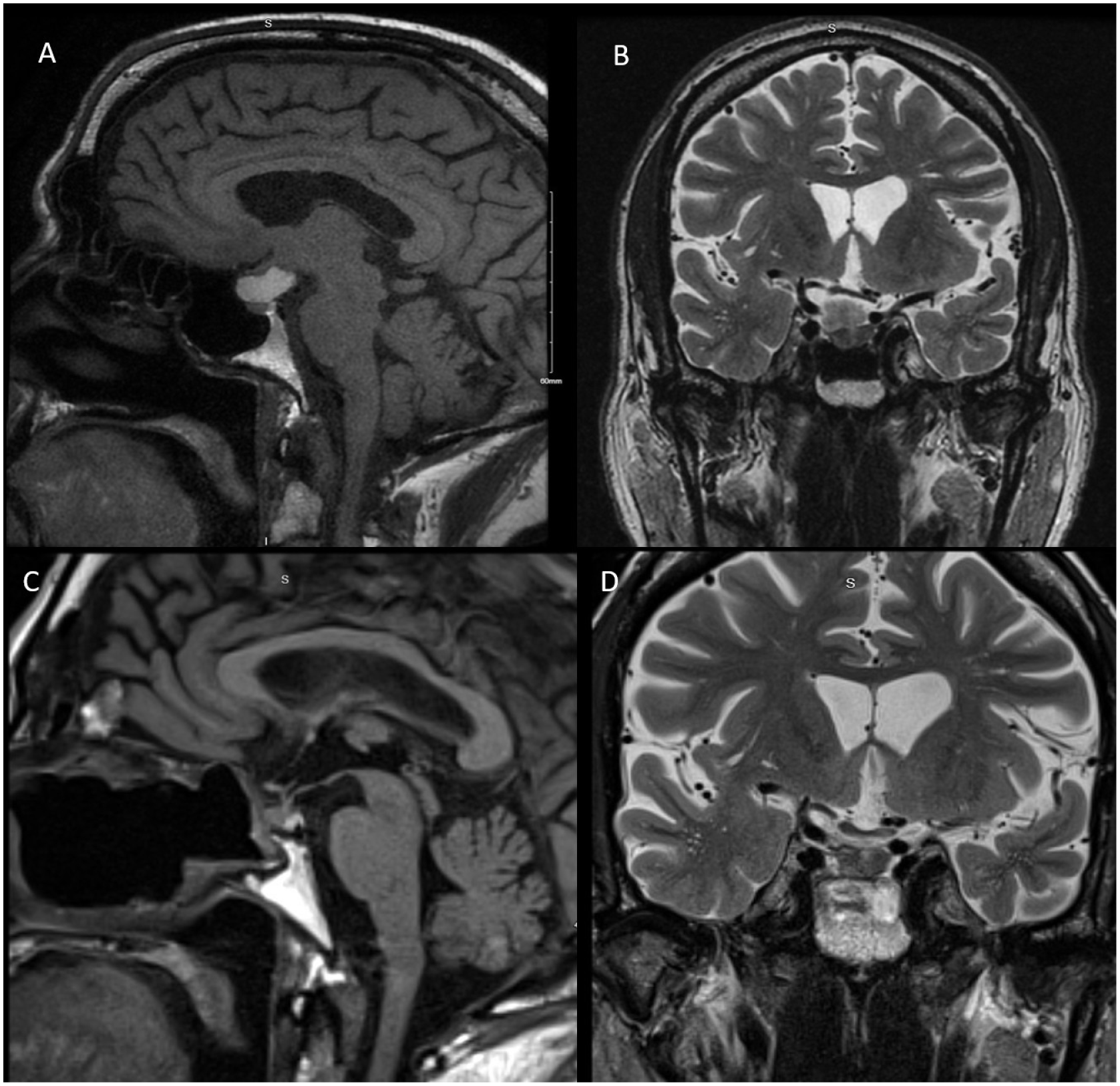
The upper images (A and B) showed are pre-operative MRI scans, and the lower images (C and D) showed are postoperative MRI scans. The preoperative MRI images (A and B) showed sellar and suprasellar cystic mass which measures 2 cm×0.8 cm×2.3 cm. The central part of the lesion is hypointense on T2 and hyperintense on T1 with mass effect on the optic chiasm which is displaced superiorly and on the right optic tract with no invasion of cavernous sinus. The postoperative MRI (C and D) complete resection of cyst with no recurrence at 3 years follow up.
Mean, standard deviation (SD), and range were calculated for descriptive statistics including LOS, total time of surgery, blood loss, and Mean Arterial Pressure (MAP). Results for intraoperative and postoperative complications as well as surgical reconstruction techniques were reported as percentages.
3 Results
A total of 30 patients who underwent EET approach for the resection of RCC were included in this cohort. The majority were females (59%) and males accounted for (41%), with a mean age of 54.6 years. Nineteen patients had RCC with ASA Class III (63.3%), Class II (23.33%), Class IV (6.6%). Moreover, five cases required reoperation due to cyst recurrence (16.67%) (Table 1). Histopathological examination of cyst fluid or cyst wall revealed that RCC was consistent in all cases. and the average amount of blood lost was 95 mL. The highest Mean Arterial Pressure (MAP) measured intraoperatively was 170 mmHg (range: 118–280 mmHg), while the average of the lowest MAP was 62 mmHg (range: 39–80 mmHg) (Table 1).
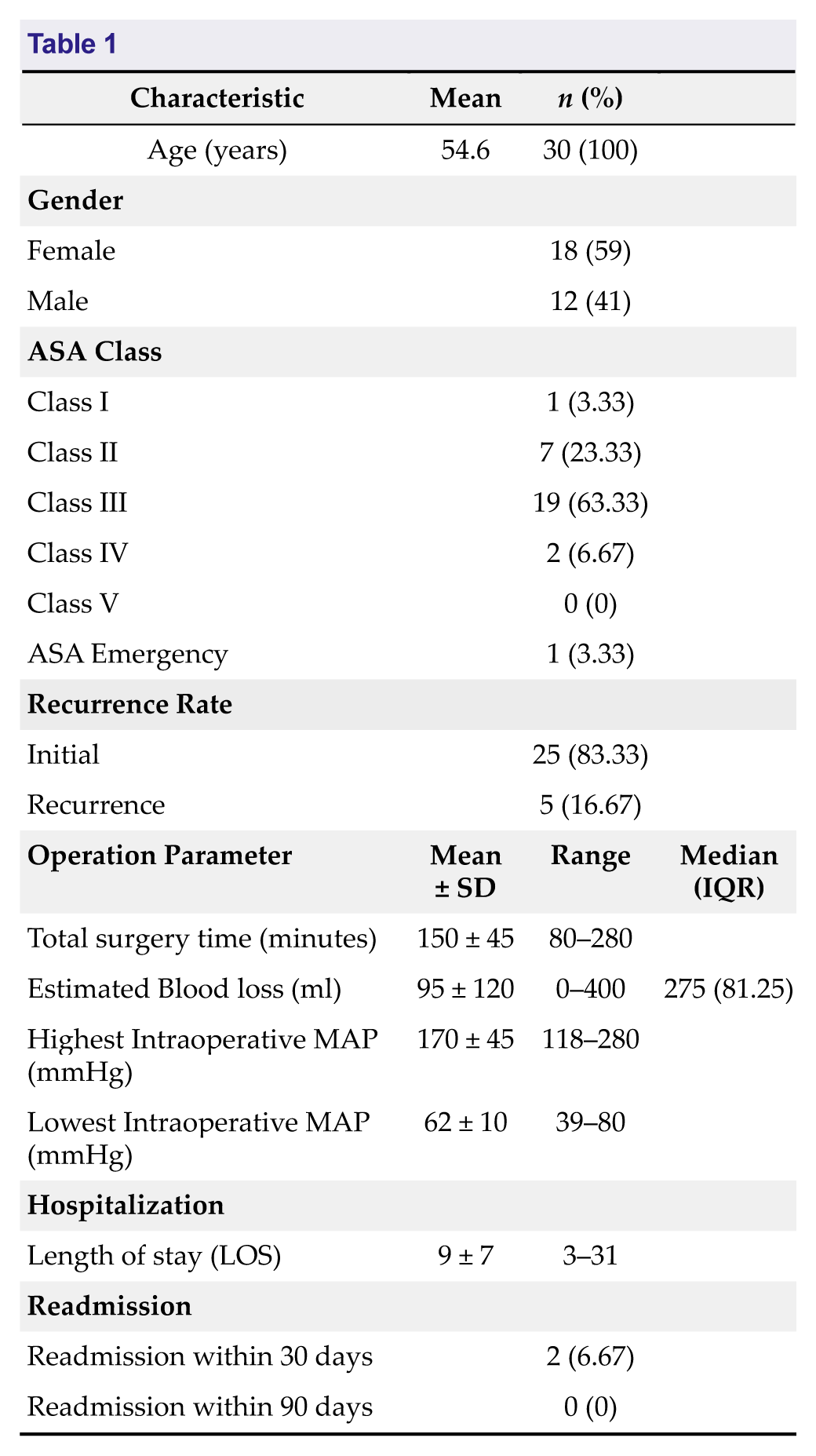
The main intraoperative measures observed in our cohort were as follows: the mean total time of surgery was 150 minutes (range: 80–280 minutes), and the average amount of blood lost was 95 mL. The highest Mean Arterial Pressure (MAP) measured intraoperatively was 170 mmHg (range: 118–280 mmHg), while the average of the lowest MAP was 62 mmHg (range: 39–80 mmHg) (Table 1).
Two patients required readmission within 30 days (6.67%). On the other hand, there were no records of readmissions within 90 days. Moreover, the length of stay (LOS) varied among patients, with an average duration of 9 days (range: 3–31 days) (Table 1).
Table 2 summarizes key surgical techniques and surgical complications. Intraoperative lumbar drain was used in two patients only (6.6%), and postoperative drain was used in five patients (16.6%). Twenty-five patients (83.3%) required reconstruction utilizing Nasoseptal flap, and Tissel and Duraform were used in twenty patients (66.6%).
Surgical Reconstruction Techniques and Complications
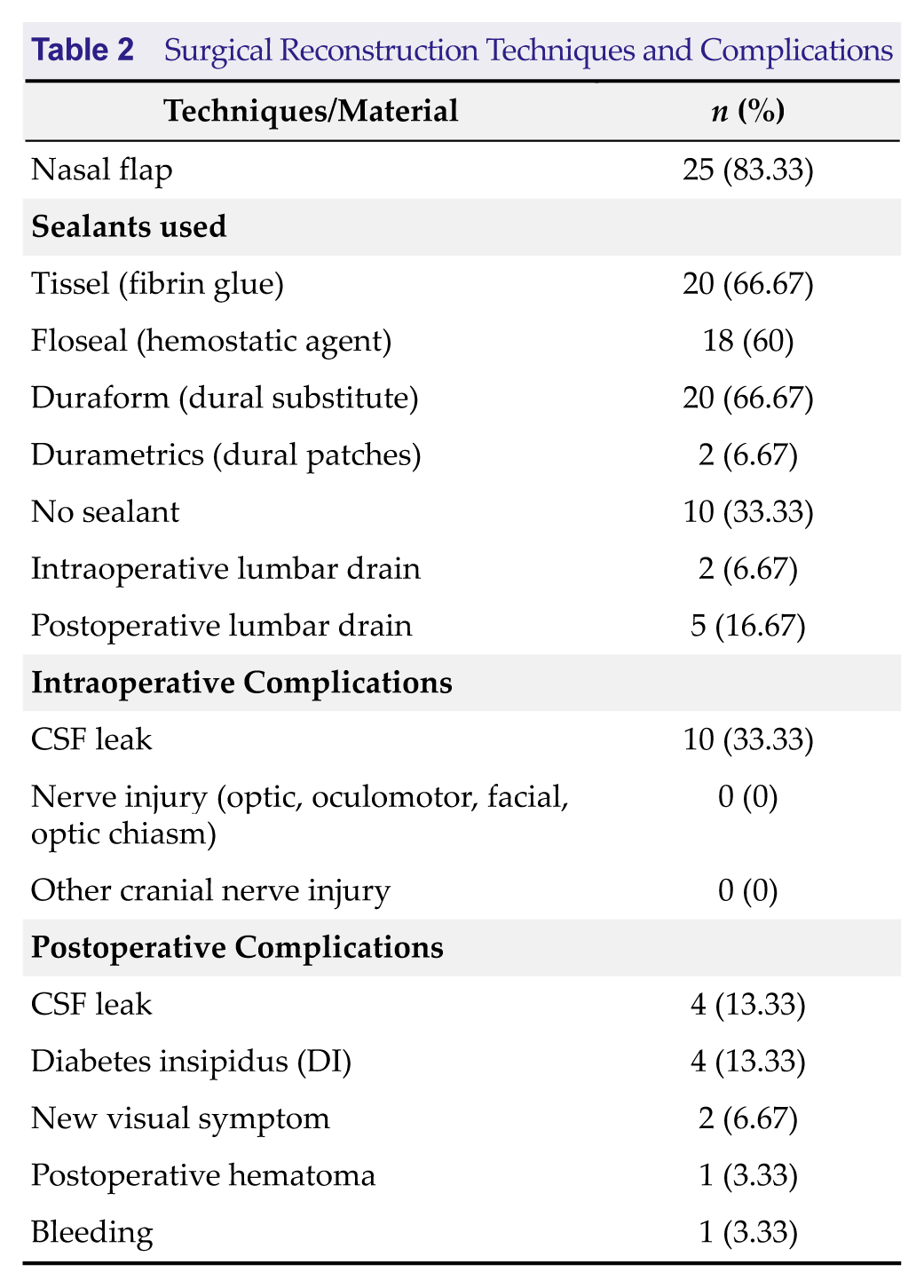
Among postoperative complications, CSF leak and Diabetes Insipidus (DI) were the most frequently documented. Four patients had CSF leak (13.3%). Similarly, four patients developed postoperative DI (13.3%), two of them had permanent DI that required long term medication. Both resection and marsupialization techniques were performed, however due to the small sample size we did not find any difference in postoperative outcome. No cases of Myocardial Ischemia (MI), arrhythmias, vascular injuries, cranial nerve injuries including optic, oculomotor, and facial nerves, or mortality were observed intraoperatively.
Two patients developed new visual symptoms (6.67%). One patient had hematoma and another patient experienced bleeding. No new motor or sensory deficits were reported (Table 2).
4 Discussion
Rathke’s cleft cyst was more commonly observed in females, a finding consistent with existing literature. Endoscopic Endonasal Transsphenoidal (EET) approach is the most widely used surgical approach for resection of RCC, providing favourable outcomes with lower rates of recurrence and complications compared to microscopic or craniotomy techniques. (1, 6, 17). In the present study all 30 patients underwent EET, and most patients experienced significant improvement following resection of RCC. According to literature, surgical indications include headaches, visual symptoms, cyst enlargement, or pituitary endocrinopathy. (5, 12, 15, 18, 19).
Visual disturbances are the most common presenting symptom, with the most favourable outcomes, and lowest rate of postoperative complications. (5, 12, 18, 19). This is consistent with our findings where most patients experienced improvement of visual symptoms, whereas two patients (6.67%) had worsened visual outcomes. This is comparable to a multicentre study by Menéndez-Torre et al. (8), which reported visual field normalization in 64.3% of patients and deterioration in 4.8%. In a similar finding by Kim et al. (18), they investigated 40 cases of symptomatic RCC and reported a recovery rate of 77% among patients with impaired visual acuity.
Moreover, endocrinopathies resulting from disruption of hypothalamic–pituitary axis, include DI, growth hormone deficiency (GHD), Adrenocorticotropic Hormone (ACTH) deficiency, hypocortisolism, hypothyroidism, and hypogonadism. Hyperprolactinemia is the most frequently reported endocrine abnormality due to stalk effect, particularly in females often presenting with galactorrhea or amenorrhea. Pre and postoperative assessment include comprehensive ophthalmologic evaluation and basal hormonal profiles (1–3, 6, 12, 13, 17, 19–21). Postoperative evaluation of patients in our cohort revealed no cranial nerve injuries or any new onset of sensory or motor deficits.
Commonly reported complications include CSF leak, DI, and anterior pituitary hormone deficiencies. Less common complications such as meningitis, intrasellar abscess, and intracranial hemorrhage can also occur (5, 17, 22). Kim et al. (18) reported intraoperative CSF leak in 34.4% and in 27.3% of cases, respectively. CSF leak can be managed by nasoseptal flap or lumbar drain. We report Nasoseptal flap was used in 83% of cases, Mendelson et al. (6) using nasoseptal flap for skull base reconstruction of CSF leak. Whereas Intraoperative lumbar drain was used only in 2 patients (6.6%). Similarly, Wait et al. (19) managed CSF leak with lumbar drain in 48% cases.
In the present study, postoperative CSF leak was identified in four patients (13.3%). Cabuk et al. (5) observed a comparable incidence of three CSF leak cases, whereas Mendelson et al. (6) reported no postoperative CSF leaks. The development of postoperative DI is most likely attributed to aggressive cyst resection and may be either transient or permanent. In our cohort, four patients (13.3%) developed DI, with two cases progressing to permanent DI; these findings are consistent with previous studies. Algattas et al. (17) documented seven cases presenting with DI, with permanent DI persisting in three patients postoperatively, while the remainder showed improvement. Similarly, Seo et al. (12) reported postoperative DI in 34.4% of cases, and Menéndez-Torre et al. (8) observed the development of transient DI in 23.9% of cases. Posterior pituitary dysfunction was found to be associated with more aggressive surgical techniques and manipulation. (4, 5, 17).
Our data shows that only 5 cases (16.6%) required reoperation due to cyst recurrence. The only predictor of cyst recurrence is the presence of squamous metaplasia (1, 2, 11, 19). High recurrence rates are associated with inflammation and purely suprasellar cysts although rare (3, 4, 23).
5 Conclusion
Surgical removal of Rathke’s Cleft Cyst using Endoscopic Endonasal Transsphenoidal approach provides favourable outcomes. Recurrence rates are associated with factors such as surgical reconstruction techniques, and CSF leak. Further prospective studies with long term follow-up and larger sample size are recommended to confirm these findings.
Footnotes
Acknowledgements
The authors are thankful to The Ottawa Hospital, Ottawa, Ontario, Canada for providing the necessary facilities during this research. The authors acknowledge the use of Grammarly by Grammarly Inc. (Version 1.2.260.1887) was used for checking spelling, punctuation, and grammatical errors in the manuscript.
Funding Information
There was no funding involved.
Author Contribution
Conception and design: Fahad AlKherayf, Alejandro Vargas-Moreno, Sami Khairy, Nathan Yang. Acquisition of data: Fahad AlKherayf, Alejandro Vargas-Moreno. Analysis and interpretation of data: Fahad AlKherayf, Sara Khalid Dabbour, Wareef W. AlGhamdi, Alejandro Vargas-Moreno, Damanpreet Kaur Lang, Nathan Yang. Drafting the article: Fahad AlKherayf, Sara Khalid Dabbour, Wareef W. AlGhamdi, Alejandro Vargas-Moreno, Sami Khairy, Nathan Yang. Critically revising the article: Fahad AlKherayf, Sara Khalid Dabbour, Wareef W. AlGhamdi, Sami Khairy, Damanpreet Kaur Lang, Nathan Yang, Shaun Kilty. Reviewed submitted version of manuscript: Fahad AlKherayf, Sara Khalid Dabbour, Wareef W. AlGhamdi, Sami Khairy, Nathan Yang, Jessica Rabski, Shaun Kilty. Approved the final version of the manuscript on behalf of all authors: Fahad AlKherayf. Statistical analysis: Fahad AlKherayf, Wareef W. AlGhamdi, Alejandro Vargas-Moreno, Damanpreet Kaur Lang. Administrative/technical/material support: Fahad AlKherayf, Damanpreet Kaur Lang, Shaun Kilty. Study supervision: Fahad AlKherayf, Nathan Yang, Jessica Rabski, Shaun Kilty.
Declaration of Conflicting Interests
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interests, or non-financial interest in the subject matter or materials discussed in the manuscript.
Data Availability Statement
The data that supports the findings of this study is reported in the tables of this article.
Ethics Statement
This study was approved by the Ottawa Health Science Network Research Ethics Board (OHSN- REB) (approval number: 20150769-01H).
Informed Consent
Not Applicable.