
Abstract
Background:
Acupuncture has become an important alternative clinical treatment for Parkinson’s disease (PD), but its efficacy and the underlying mechanisms remain debatable. Using a newly developed magnetic resonance angiography (MRA) method that has higher sensitivity for smaller and distal vessels and a novel tool that can trace vessels and extract vascular features, the immediate effects of acupuncture on intracranial vessels and blood flow in patients with PD as well as correlations with clinical outcomes were quantitatively evaluated.
Methods:
Fifteen PD patients received acupuncture at the Dazhui and Fengchi acupoint positions. MRA was performed before and after 30 min of treatment. The cerebral blood flow (CBF) and the length, volume, diameter, and signal intensity of the intracranial internal carotid artery (ICA) and middle cerebral artery (MCA) were measured. The Unified Parkinson’s Disease Rating Scale part III (UPDRS-III) and Visual Analogue Scale (VAS) were used to evaluate the motor symptoms and the subjective feelings of discomfort.
Results:
Acupuncture significantly reduced UPDRS-III and VAS scores. No significant changes were noted in the overall CBF before and after treatment. However, there was a significant extension effect on the length of the intracranial ICA and MCA and the distal MCA, and a significant increase in the number of branches of the MCA was found. Although acupuncture tended to increase the total volume of the intracranial ICA and the volume of the MCA, no statistical significance was reached. The total intensity was not altered, but the intensity and diameter of the M1 segment were significantly increased, whereas the intensity of the MCA was decreased. A positive correlation between M1 intensity changes and UPDRS-III changes was found.
Conclusions:
Angiographic evaluation suggested that acupuncture had a significant effect on intracranial blood vessels, which is one possible mechanism for acupuncture improving the motor symptoms of PD.
Keywords
1 Introduction
Parkinson’s disease (PD) is the second-most common degenerative disease of the central nervous system after Alzheimer’s disease. It causes an increasingly heavy social and economic burden, affecting more than 1% of adults older than 60 years of age in European and American countries [1, 2]. The prevalence can increase to 4% in even older individuals [1, 2]. By contrast, the incidence of PD in Asian regions is relatively low (0.6%), which may be related to differences in geographical environments, genes, lifestyles, and statistical methods. The use of traditional medical therapies for prevention and treatment was also reported to be an important reason for differences [3]. In the United States, 40% of PD patients have utilized supplementary and alternative medical treatment methods to supplement or even replace conventional medications [4]. The use of traditional Chinese medicine (TCM) accounts for 52.76% of these cases [5]. There is increasing evidence suggesting that TCM can effectively improve nonmotor symptoms, prolong the duration of drug effects, and reduce motor complications [6, 7].
With good compliance and minor side effects, acupuncture has become one of the most commonly used TCM methods in clinics. Studies have shown that acupuncture could relieve motor symptoms [8–12] of PD, such as tremors, stiffness, and bradykinesia, finger movements, and gait and balance disorders [13]. It is associated with good effects on nonmotor symptoms as well, such as fatigue [14], sleep disorders [15], and gastrointestinal dysfunction. Acupuncture can also improve the efficacy and reduce the toxicity of dopaminergic medications when prescribed together [11, 16]. Increasing numbers of physicians and patients are accepting acupuncture in the treatment of PD worldwide [17–20].
However, controversy regarding the effectiveness of acupuncture and its mechanisms remains. Acupuncture is generally applied on the basis of syndrome differentiation under the guidance of the holistic classical TCM theory [21, 22]. It is an advantageous factor that cannot be replaced in the medical field at present. Inconsistent results, however, have been reported [23–25]. Some suggested that acupuncture did not achieve a significant effect with PD [8]. Although studies found that the clinical effect of acupuncture in combination with drugs was superior to that of drugs alone, it was also claimed that the placebo effect could not be ruled out when assessing the effectiveness of acupuncture [26]. The underlying modern medicine basis for how acupuncture takes effect remains not fully understood. There is still a need for a technical approach that can provide more rigorous insight and guidance for the clinical treatment of PD with acupuncture.
The blood system plays an important role in TCM theory, and blood flow improvement was considered as a vital effect for acupuncture to achieve symptom relief and disease treatment. In the meantime, a growing body of evidence has indicated that various aspects of neuro-degenerative diseases are closely associated with changes in cerebrovascular function. Studies have shown that patients with PD have significant decreases in cerebral blood flow (CBF) [27] that are associated with the severity of the disease. Additionally, the change in CBF induced by Madopar had a negative correlation with the Unified Parkinson Disease Rating Scale (UPDRS) scores, suggesting that the improvement of symptoms was associated with the increase in CBF in related areas [28]. Changes in CBF could be used as important markers for disease diagnosis, mechanism investigation, and treatment assessment [29]. In recent years, there have been studies that explored the CBF regulatory effects of acupuncture in Alzheimer’s disease, stroke, and other diseases. Results on acupuncture treatment for PD remain very limited [30–32].
Several methods can be used to measure CBF, such as rheoencephalography, transcranial Doppler imaging, and near-infrared spectroscopy. In comparison, magnetic resonance angiography (MRA), which uses methods such as arterial spin labeling (ASL), provides a powerful means for extensive inspection, including not only quantitative measurement of CBF but also structural observation of the vessels. Recently, a new MRA method was developed, called simultaneous noncontrast angiography and intraplaque hemorrhage MRA (SNAP-MRA) [33]. It can perform three-dimensional (3D) intravascular angiography and plaque imaging simultaneously in a single scan and has high sensitivity for intraplaque hemorrhage, intramural hematoma, and thrombus [34]. Since it is optimized for intracranial artery imaging [35], SNAP-MRA has high accuracy in testing lumen stenosis, enables the visualization of smaller arteries, and shows good ability in testing distal vessels [36]. Furthermore, with the newly developed analysis tool of iCafe software to trace the vessels, quantitative intracranial vascular features can be extracted [37]. It provides a new opportunity to look deeper into the effects and mechanisms of acupuncture on the symptoms of PD.
In this study, we applied acupuncture to PD patients and motor symptoms were assessed. Before and after acupuncture, pseudo-continuous ASL (PCASL) and SNAP-MRA were performed to evaluate the changes in CBF and vascular features, such as the length, volume, distal length, proximal length, diameter of the M1 segment, signal intensity of large vessels, and signal intensity of the intracranial internal carotid artery (ICA) and middle cerebral artery (MCA). The impact and effects of acupuncture on PD were therefore analyzed.
2 Methods
2.1 Ethics statement
This study was conducted according to the ethical standards of the Declaration of Helsinki and applicable national regulations. It was registered on ClinicalTrials.gov under the number NCT03501004 and approved by the ethics committee of Tsinghua University Yuquan Hospital (Approval No. QHDXYQYY 20180001). All participants provided written informed consent.
2.2 Subjects
Fifteen PD patients diagnosed by the neurologists of Tsinghua University Yuquan Hospital were enrolled from September 2017 to October 2018. Inclusion criteria were: (1) age from 40 to 70 years; (2) meeting the new standard for clinical diagnosis of PD introduced by the International Parkinson and Movement Disorders Society in 2015 [38]; (3) stage 2 to 3 via the Hoehn–Yahr (H–Y) scale; (4) having received a stable dose of anti-Parkinson medication for at least 3 months without any adverse events; (5) having education level of junior high school or above; (6) having a correct understanding of the significance of clinical studies on acupuncture; and (7) displaying good compliance with the researchers’ observations and evaluations. Exclusion criteria were patients with (1) secondary Parkinson’s syndrome; (2) Parkinson’s syndrome; (3) central and peripheral infectious diseases; (4) dysarthria; and (5) severe psychiatric disorders that affect expression, malignancies, disability, and other severe somatic disorders. All patients maintained anti-Parkinson medications with no changes during the study as advised. Demographic information, including gender, age, stage via the H–Y scale, duration of the disease, and daily dose of anti-Parkinson drugs of all participants were recorded.
2.3 Assessment and intervention procedure
Patients were instructed to refrain from anti-Parkinson medication for at least 12 h before the test. Before acupuncture, their motor symptoms were evaluated using the Unified Parkinson’s Disease Rating Scale part III (UPDRS-III). The overall subjective feeling of comfort caused by motor and nonmotor symptoms was evaluated using the Visual Analog Scale (VAS) with 0 representing “no discomfort” and 10 for “unbearable discomfort”. An MRI scanning session followed, after which the patients were removed from the scanner and rested for 30 min. Then, they were treated with acupuncture for 30 min, followed by a reevaluation of UPDRS-III and VAS, and a second MRI scanning session.
2.4 Acupuncture intervention
Acupuncture intervention was undertaken according to the Standards for Reporting Interventions in Clinical Trials of Acupuncture [39]. All interventions were performed by the same acupuncturist who had more than 5 years of clinical experience. Disposable sterile acupuncture needles (Suzhou Medical Products Co. Ltd., Suzhou, China) measuring 0.25 mm × 25 mm were used. Dazhui (DU14) and bilateral Fengchi acupoints (GB20) were selected that had previously shown therapeutic effects with PD patients [40–44]. The Dazhui acupoint (DU14) is located beneath the spinous process of the seventh cervical vertebrae. The Fengchi acupoints (GB20) are located beneath the occiput and in the depression between the sternocleidomastoid muscle and the upper end of the trapezius muscle.
Operation procedures were as follows: routine disinfection of the acupoints was performed, and the needles were inserted 15–18 mm deep at the Dazhui acupoint (DU14) and 15–20 mm deep at the bilateral Fengchi acupoints (GB20). A twist and turn supplement method was implemented by rubbing the needle with the thumb in the forward direction and index finger in the backward direction, twisting it clockwise, and rubbing it firmly to reach a fixed depth and angle. The needles were left in for 30 min before removal.
2.5 MRI data acquisition
MRI scans were performed using an Achieva 3.0-Tesla TX MRI scanner with a 32-channel head coil (Philips, Amsterdam, Netherlands). The subjects rested flat on the examination table and were asked to breathe calmly with eyes closed and remain awake. The void between the subject’s head and the coil was stuffed with sponges to minimize head movement. Scanning started after the subject became familiar with the environment. 3D-SNAP-MRA was performed with field of view (FOV) = 160 × 160 × 60 mm3, matrix = 200 × 200, 150 slices, repetition time (TR) = 10.0 ms, echo time (TE) = 5.6 ms and flip angle (FA) = 11°. PCASL was performed with FOV = 230 × 230 × 132 mm3, matrix = 64 × 64, 22 slices, thickness = 6.0 mm, and TR/TE = 3673/11 ms and FA = 90°. T1WI 3D TFE was performed with FOV = 256 × 256 × 160 mm3, voxel = 1.0 × 1.0 × 2.0, matrix = 256 × 256 × 160, 160 slices, NSA = 1, TR/TE/FA = 7.5/3.7/8, technique = 3D fast field echo (FFE), short interval = 2800 ms, and time = 3 min 46 s.
2.6 CBF determination
The CBF values were processed using MatLab software (MathWorks, Natick, MA, USA) with in-house written and developed scripts. The mean perfusion-weighted imaging was converted to CBF in physiological units with a well-recognized model [45]. This model used pseudo-continuous labeling, background suppression, a segmented three-dimensional readout without vascular crushing gradients, and calculation and presentation of both label/control difference images and CBF in absolute units. The mean CBF of the whole brain was calculated using a subject-specific mask of voxels containing at least 50% gray matter that was generated by segmentation of T1-weighted imaging with the SPM8 toolbox [46].
2.7 Vascular feature extraction
SNAP-MRA data were analyzed with iCafe software to extract the vascular features [37]. To enhance the capacity to distinguish vessels in close proximity, a modified open-curve active contour model was used to trace the vessels. Modifications included reslicing, intensity normalization, rudimentary segmentation before tracing, and a combined tracing approach with both the original image and the Frangi vesselness-filtered image [37]. Then, the arteries were labeled and the features were calculated. It was a semi-automated process that allowed human supervision and correction to ensure optimal tracing quality. Further details on the implementation can be found in a previous publication [37].
Extracted features included total length, the intracranial artery segment visualized in the ICA and MCA, total volume, the volume of the visualized ICA and the intracranial MCA with the calculation based on a cylindrical model with a varying radius along the centerline, total intensity, the mean intensity of an artery with a relatively large radius and vertical orientation including the ICA and MCA, the length of the intracranial segment of the MCA, the volume of the intracranial MCA, the mean signal intensity at each centerline point of all MCA arteries, proximity length (the length of the main artery near the circle of Willis or the length of the M1 segment; distal length), the lengths of M2, M3, and the distal artery, mean of the M1 radius, the mean of the radius of the M1 segment of the MCA, and the number of branches in the artery from the bifurcation to the end of the branch.
2.8 Statistical analysis
All statistics and calculations were performed using the SPSS version 22.0 statistical analysis program (IBM Corp., Armonk, NY, USA). The measurement data were expressed as the mean ± standard deviation (SD). Statistical analysis was performed primarily on the basis of the comparison of efficacy. When the indicators were normally distributed, a t-test was used; otherwise, nonparametric methods, such as the Wilcoxon rank-sum test or Kruskal–Wallis H test, whichever was suitable, were used. Regression analysis was based on linear regression analysis. All statistical analyses were performed with α = 0.05 as the significant limit of difference.
3 Results
3.1 Demographic characteristics
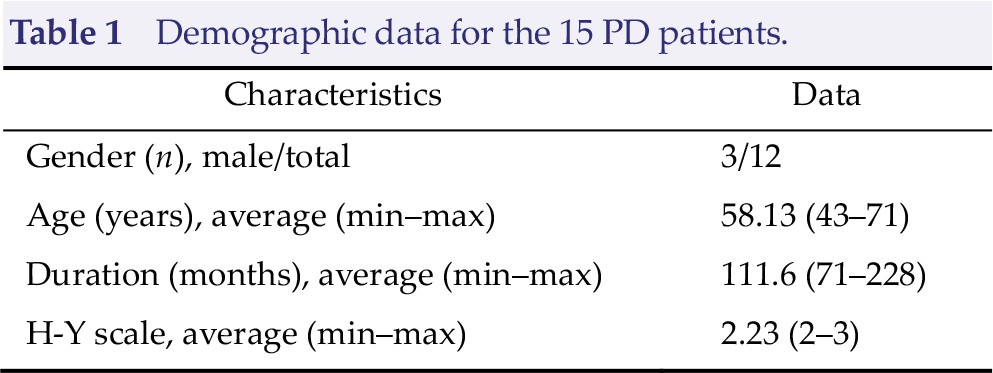
Table 1 details the demographic data for the 15 subjects. The effect of acupuncture treatment on motor symptoms was evaluated with UPDRS-III. The UPDRS-III score before acupuncture was 44.4 ± 9.1 and significantly decreased to 38.6 ± 11.0 (P ≤ 0.001) after acupuncture (Table 2). The VAS was 7.25 ± 0.24 before acupuncture and 5.96 ± 0.35 after acupuncture. The decrease was significant (P = 0.001; Table 2).
Demographic data for the 15 PD patients.
Motor symptoms and subjective comfort data.
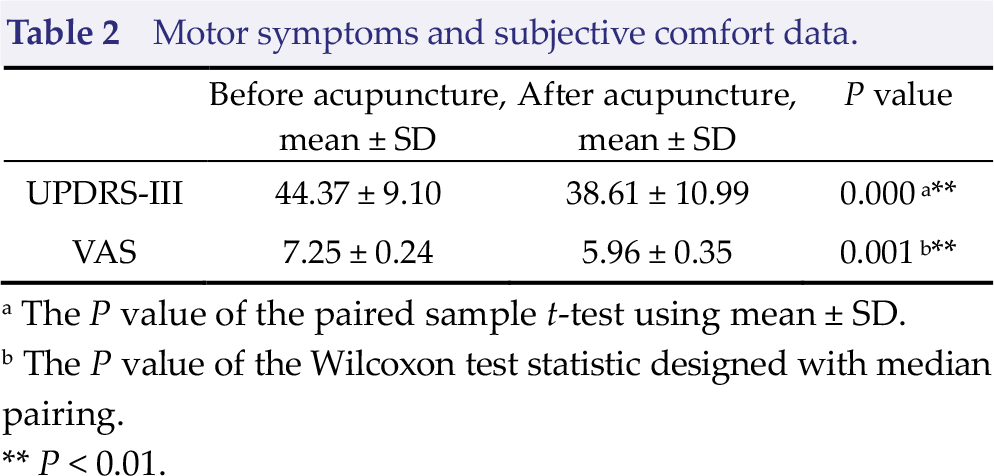
aThe P value of the paired sample t-test using mean ± SD.
bThe P value of the Wilcoxon test statistic designed with median pairing.
**P < 0.01.
3.2 CBF changes after acupuncture
After acupuncture, obvious changes in signal intensity, shown in gray levels, were frequently noted in SNAP-MRA images, especially in the ICA and MCA M1 segments. Two typical examples are shown in Fig. 1.
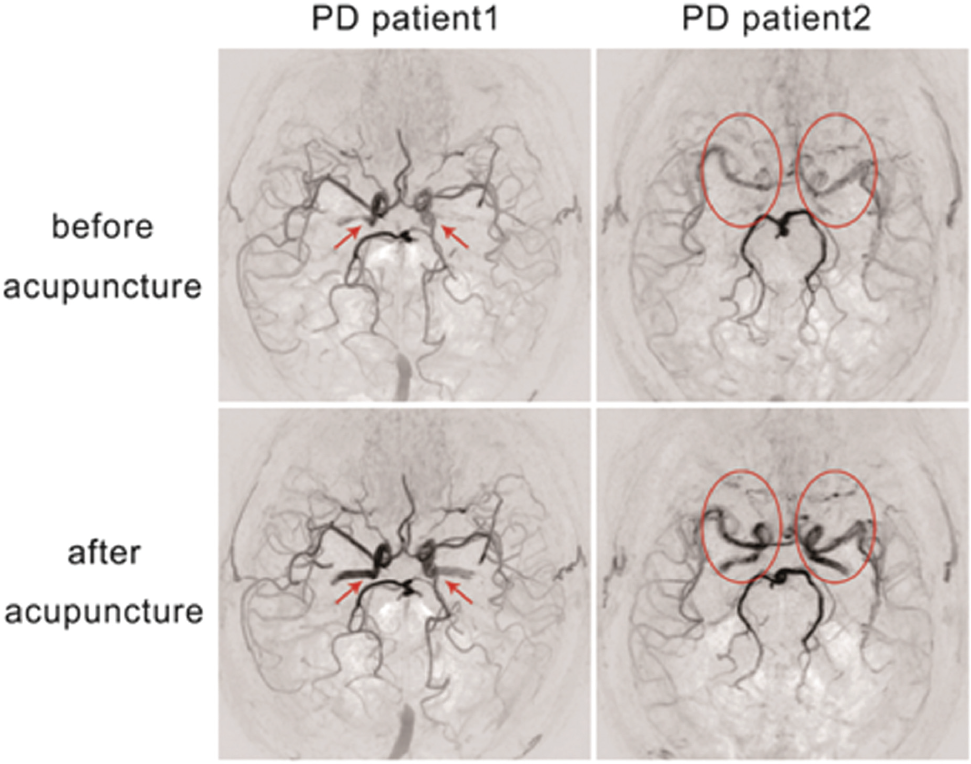
SNAP-MRA images of two PD patients (patient 1: 63 years, female; patient 2: 57 years, female) before and after acupuncture showing that the signal intensity and grayscale of the ICA and MCA M1 segments were significantly different. The signal intensity increased after acupuncture, and the grayscale became higher.
However, the mean global CBF was 31.70 ± 2.97 before acupuncture and 31.55 ± 3.00 after acupuncture, showing no statistically significant difference (P = 0.847).
3.3 Cerebrovascular feature changes after acupuncture
Through vessel tracing, lengthening of intracranial blood vessels, especially the distal MCA, could be seen in most patients after acupuncture. A typical example is shown in Fig. 2.
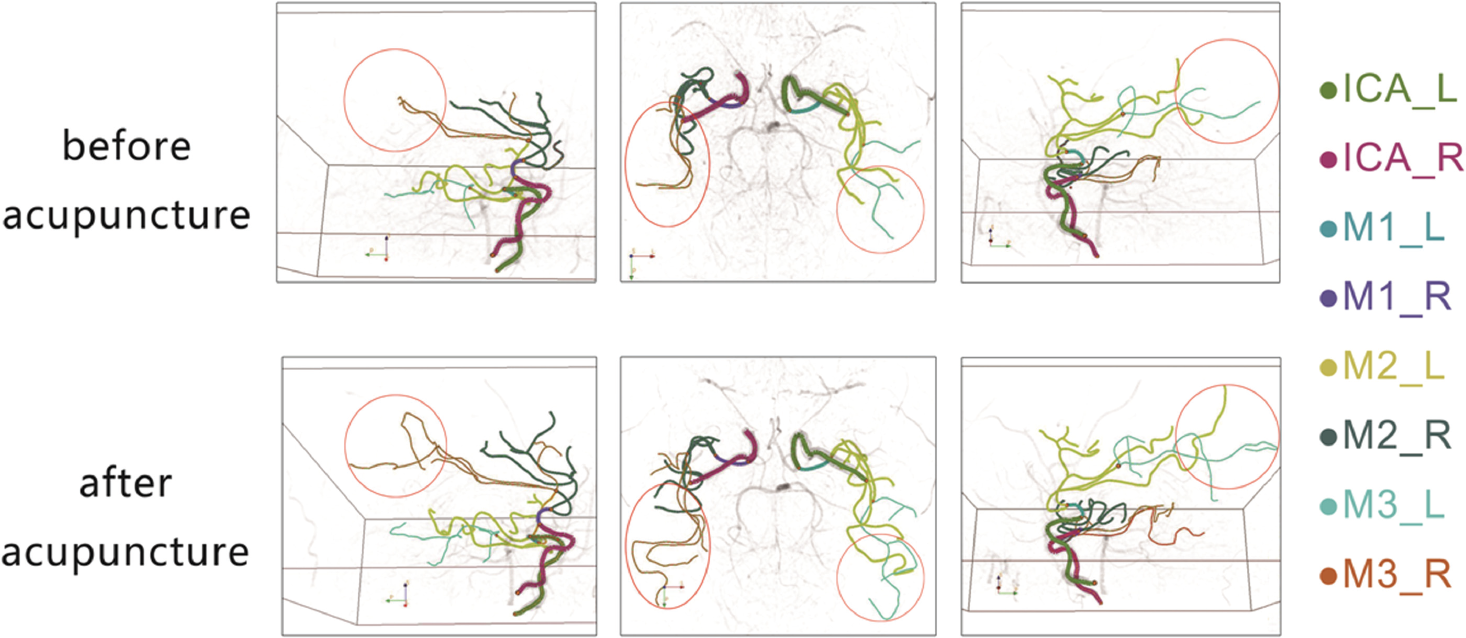
Sagittal and axial views of SNAP-MRA images of a 60-year-old female PD patient. The length of intracranial blood vessels changed significantly before and after acupuncture, and the distal length of the MCA after acupuncture was significantly increased (as shown in the red circles).
Table 3 lists all the quantitative values of the extracted cerebrovascular features. Among the general cerebrovascular features, the total length showed a significant increase (P = 0.012) from 3,509 ± 814 before acupuncture to 3,900 ± 935 after acupuncture. The total volume (P = 0.098) and the total intensity (P = 0.541) did not show a significant difference.
Total and local cerebral blood flow and vascular data.
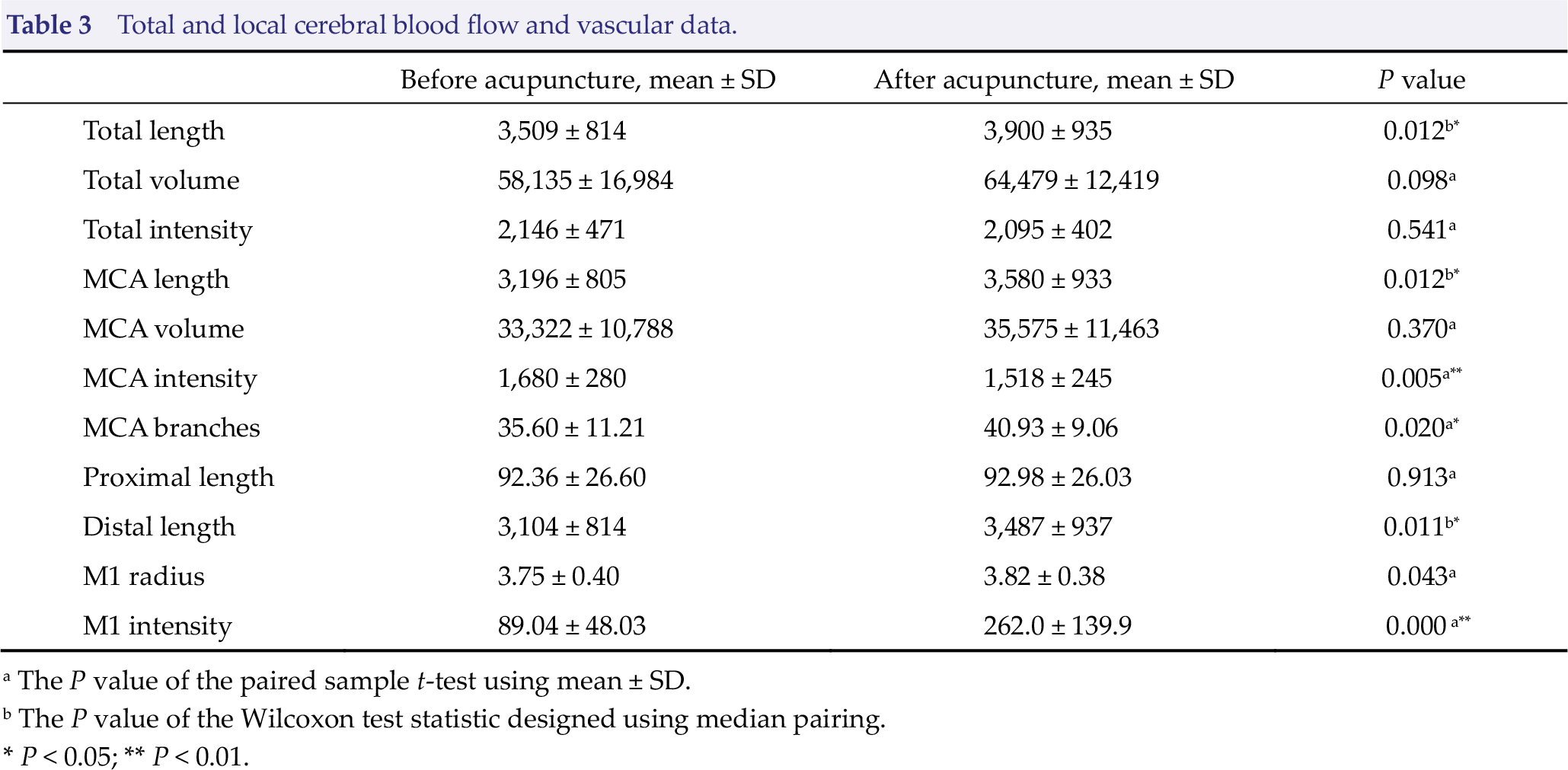
aThe P value of the paired sample t-test using mean ± SD.
b The P value of the Wilcoxon test statistic designed using median pairing.
*P < 0.05; ** P < 0.01.
Among the local cerebrovascular features, MCA length (P = 0.012) and branches (P = 0.020), distal length (P = 0.011), M1 radius (P = 0.043), and M1 intensity (P ≤ 0.001) showed a significant increase, whereas the MCA intensity (P = 0.005) showed a significant decrease. The other features, namely, the MCA volume (P = 0.370) and the proximal length (P = 0.913), showed no difference.
Correlations between the changes in the distal length and proximal length with the changes in the total length and the MCA length were examined (Fig. 3). There was a linear relationship between the distal length changes and the total length (r = 0.921, P ≤ 0.001) as well as the MCA length changes (r = 0.971, P ≤ 0.001) before and after acupuncture. This correlation was not found with the proximal length changes (P = 0.567 and P = 0.621, respectively).
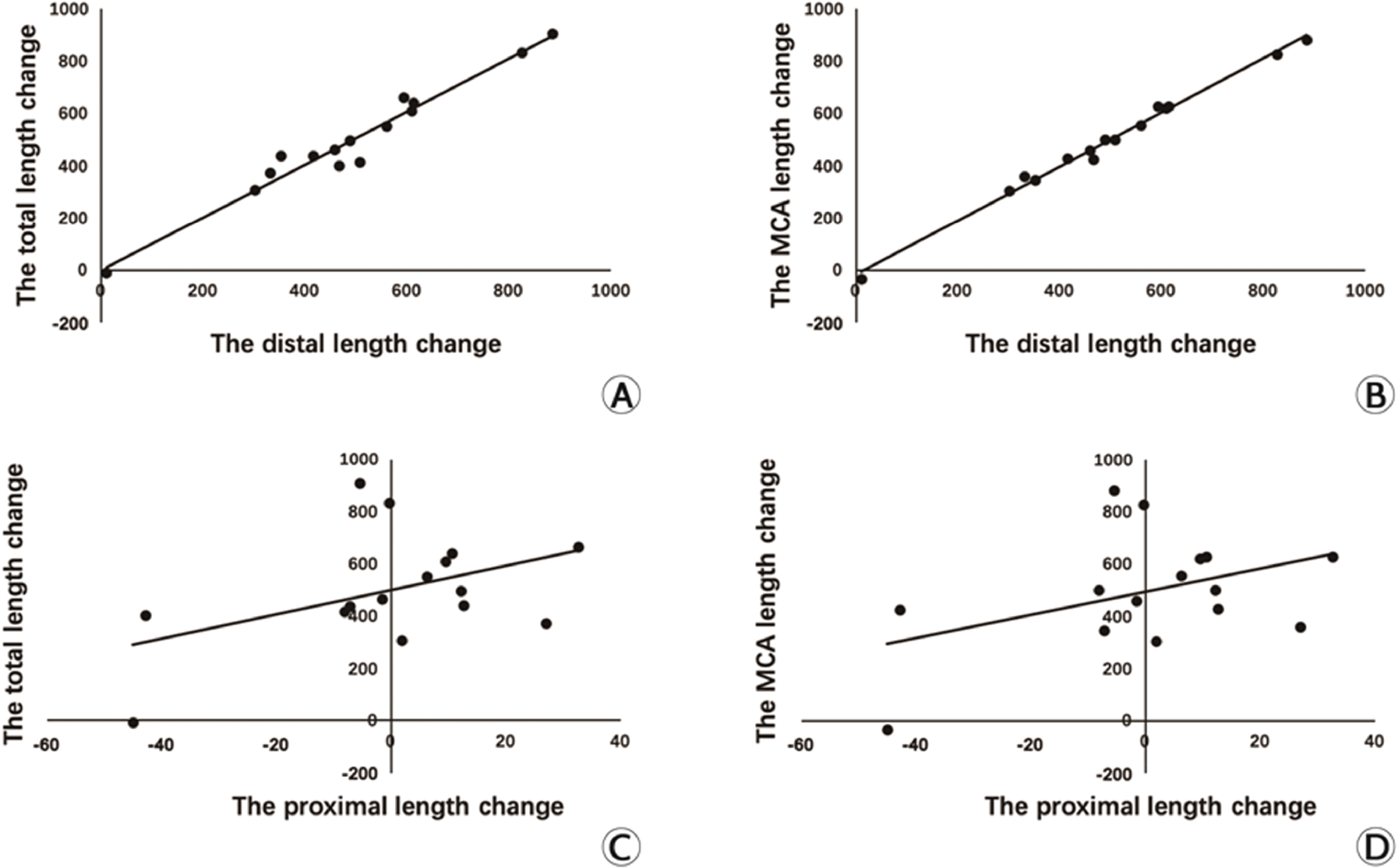
(A) Linear relationship between the distal length changes and the total length changes. (B) Linear relationship between the distal length changes and the MCA length changes. (C) Linear relationship between the proximal length changes and the total length changes. (D) Linear relationship between the proximal length changes and the MCA length changes.
3.4 Correlation between the vascular characteristics and clinical outcomes
Linear regressions were performed to analyze the correlations between changes in cerebrovascular characteristics before and after acupuncture and changes in clinical symptoms and subjective comfort feelings (Table 4). The results showed that there was a positive correlation between the changes in signal intensity of the M1 segment and the changes in the UPDRS-III score (r = 0.911, P ≤ 0.001, Fig. 4). Changes in the other vascular characteristics showed no correlation with the changes in UPDRS-III nor VAS scores.
Linear regression analysis of vascular characteristics changes with UPDRS-III and VAS changes before and after acupuncture.
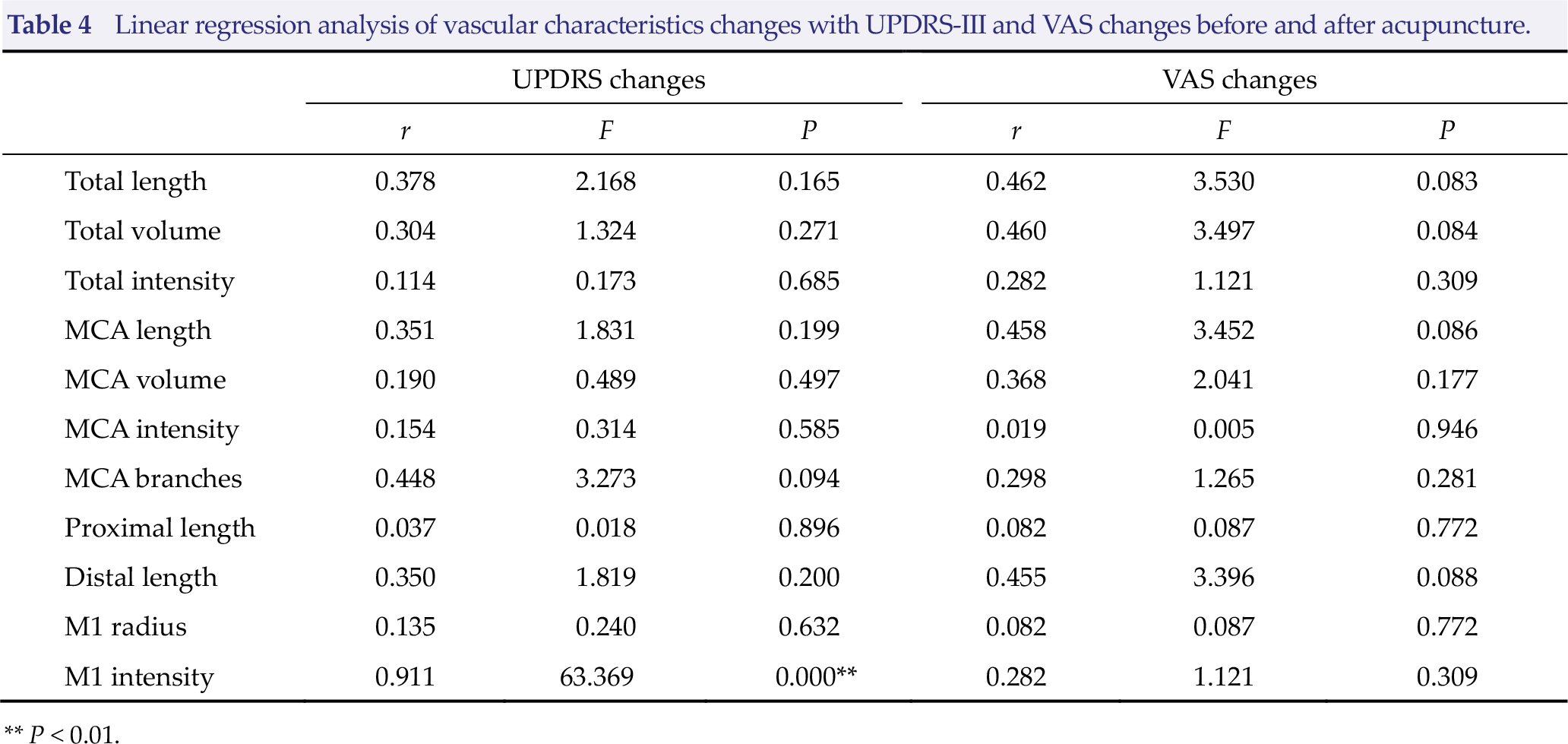
** P < 0.01.
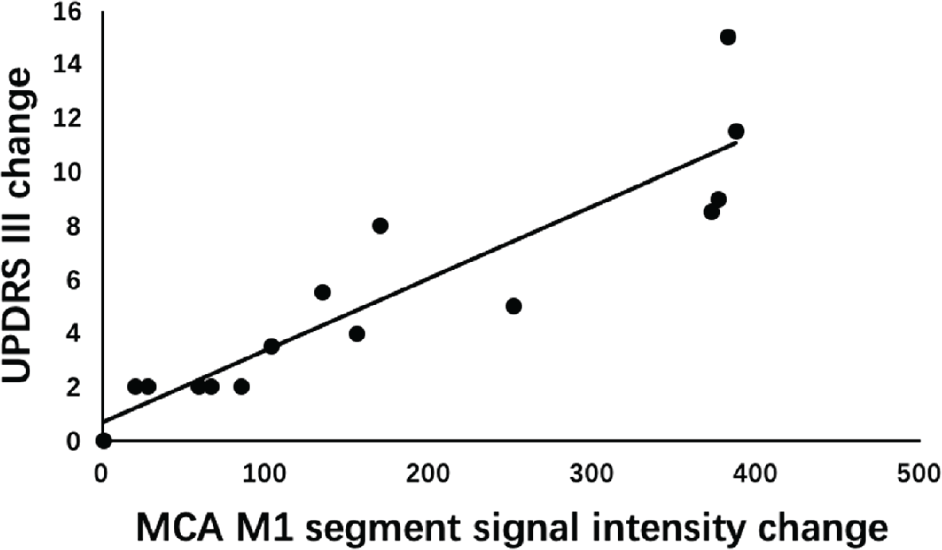
Linear regression analysis of MCA M1 segment signal intensity changes and UPDRS-III changes before and after acupuncture.
4 Discussion
In this study, PCASL and SNAP-MRA were used to visualize the changes in the intracranial blood vessels before and after acupuncture in a real-time and quantifiable manner. These are groundbreaking results. With the newly developed quantitative analysis tool iCafe, brain vessels were traced and various features were extracted and analyzed. These methods helped to clearly and intuitively display the physiological and pathological mechanisms of acupuncture, which is of great importance for further exploration of TCM and acupuncture in the field of brain science.
After acupuncture at the Dazhui and Fengchi acupoints, the PD patients showed improvement in both movement performance and subjective feelings evaluated with UPDRS-III and VAS scales, respectively. During the procedure, various cerebrovascular characteristics changed.
It was revealed that acupuncture significantly increased the total length of the intracranial ICA, the total length of the MCA, and the distal length of the M3 segment. Since the increase in the proximal length of the MCA was not significant, the increase in the total length of the intracranial ICA and total valid length of the MCA resulted from the increase in the distal length of the M3 segment. The M3 segment of the MCA provides blood to most parts of the dorsolateral side of the cerebral hemisphere, including the anterior central gyrus, posterior central gyrus, middle frontal gyrus, inferior frontal gyrus, superior parietal lobule, supramarginal gyrus, and temporal lobe. These regions are important components of the cortex– striatum circuit, which plays a decisive role in the control of a patient’s sensation and movement. Previous studies showed that blood flow in frontal and parietal lobes was reduced in patients with PD, whereas dopamine had a therapeutic effect by improving blood flow in the corresponding brain regions [28]. There is direct contact between the cerebral micro-vascular system and dopaminergic nerve endings, which is considered to be one of the mechanisms for the improvement of CBF responses and motor symptoms caused by anti-PD drugs. Lengthening of the distal M3 segment blood flow implied blood supply improvement to these regions, which could lead to functional enhancement. This could be the reason behind acupuncture improving the motor symptoms of PD patients.
Additionally, blood flow in the striatum, globus pallidus, and other basal ganglia regions of the dopaminergic pathway was decreased in patients with PD. It primarily depends on the deep perforating branch in the horizontal segment of the MCA [47]. Our results revealed that acupuncture significantly expanded the diameter of the M1 horizontal segment and increased the number of vessel branches. This could also contribute to the therapeutic effect of acupuncture.
Despite the visible differences in local image signal intensities being observable, especially in the ICA and MCA M1 segment (Fig. 2), the quantified CBF of the whole brain showed no significant difference before and after acupuncture. This implied that acupuncture modulated and balanced the distribution of the cerebral blood supply rather than increasing the whole brain CBF. Thus, whole brain CBF might not be a sensitive indicator of the effect of acupuncture. Analysis of regional CBF might be needed to further demonstrate the influence of acupuncture on brain functions [48].
Among the cerebrovascular features that were altered by acupuncture, changes in the intensity of the MCA M1 segment showed a linear relationship with that of UPDRS-III scores. It again implied that the local blood flow improvement likely plays an important role in acupuncture treatment. The other features demonstrated no quantitative improvement in movement performance or subjective feelings, as revealed by linear regressions, and this might be due to confounding factors, such as individual variation or limitations in the sample size. Further systematic and comprehensive studies should be carried out to elucidate the quantitative role of these features. Moreover, improvement in analysis methods might also be needed.
There were certain limitations in this study, including the relatively small sample size. Because of the cost of vascular-neuroimaging research, most neuroimaging studies have a small sample size. Some researchers suggested [49, 50] that the statistical power of neuroimaging studies could be obtained with 12–15 subjects in each group. This study only included PD patients with moderate symptoms. Whether acupuncture would have the same effect in patients with severe conditions requires further research. The lack of a control group was another limitation of this study. This is also a general challenge to current acupuncture studies. An appropriate control group that would not receive any treatment or treatment with sham needles having a puncture effect could be applied to specify the effects of acupuncture and rule out the placebo effect.
5 Conclusions
In this study, acupuncture at the Dazhui and Fengchi acupoints improved movement performance and subjective feelings of PD patients. As revealed by quantitative analysis based on SNAP-MRA, various cerebrovascular features were altered by the treatment, which might account for the therapeutic effects. Moreover, blood flow in the M1 segment showed a correlation with improvement in motor scores. These findings shed new light on the application of acupuncture to treat PD.
Footnotes
Ethical approval
Consent
A written informed consent was obtained from all participants.
Conflicts of interests
The authors declare that there is no conflict of interests regarding the publication of this article.