
Abstract
To review the clinical efficacy of minimally invasive pedicle fixation combined with anterior small incision focus debridement for single-segment lumbar spine tuberculosis, a total of 31 patients with single-segment marginal lumbar tuberculosis were enrolled in the study. All the patients received quadruple anti-tuberculosis chemotherapy for 2 weeks before surgery and treatment with minimally invasive posterior internal fixation, anterior small incision focus debridement, and bone graft fusion. Those patients with preoperative kyphosis deformity were initially treated with appropriate posterior distraction correction. Except for 1 patient who healed 2 weeks after medical dressing change, the remaining 30 patients healed as expected. All the patients had no screwrelated surgical complications, neurological dysfunction, vascular injury, and other complications. The average visual analog scale scores at 3 months postoperatively were significantly decreased to 1.4 ± 1.5 (P < 0.05). In conclusion, under the premise of treatment using appropriate, effective anti-tuberculosis agents, this surgical procedure for managing patients with lumbar vertebral tuberculosis achieved satisfactory results, effectively reducing the exposure range and fusion segments in simple anterior focus debridement and internal fixation. Using minimally invasive posterior pedicle screw fixation can effectively increase spine stability, reduce fusion segment, and decrease anterior surgical trauma and complications.
Keywords
1 Introduction
The spine is the most common site for bone and joint tuberculosis. The occurrence and the development of spinal tuberculosis can often lead to spinal cord dysfunction, spinal instability, and kyphosis. Surgical treatment of spinal tuberculosis has been applied for more than half a century. Focus debridement, spinal cord decompression, and bone graft fusion are effective approaches for treating patients with spinal tuberculosis and severe clinical symptoms [1 –6]. Lumbar tuberculosis is the most common spinal tuberculosis and is usually treated with surgery, including anterior focus debridement, bone graft (titanium mesh) fusion, internal fixation, posterior decompression, focus debridement, pedicle screw fixation, anteroposterior joint surgery, and other methods. These methods have advantages as well as disadvantages. Currently, anterior surgery is more extensively used for managing patients with lumbar vertebral or intervertebral disc tuberculosis but not posterior appendage involvement. However, this procedure has disadvantages of insufficient internal fixation strength as well as wide anterior exposure-induced damages in vital vessels, organs, and sympathetic chain. With the development of minimally invasive techniques, minimally invasive screws are gradually and widely used in clinics. From July 2010, 31 patients with single-segment lumbar vertebral and intervertebral disc marginal tuberculosis were treated using minimally invasive posterior internal fixation, anterior small incision focus debridement, and bone graft fusion, and have achieved satisfactory clinical results.
2 Patients and methods
2.1 General information
All the patients consented to the procedures, which were approved by the clinical research ethics committee of Qilu Hospital, Shandong University. Thirty-one patients (19 males and 12 females) who had single-segment lumbar marginal tuberculosis but no posterior appendage involvement, were admitted to Qilu Hospital from July 2010 to July 2015 (Table 1). They were treated with one-stage, minimally invasive posterior internal fixation, anterior small incision focus debridement, and bone graft fusion. On average, the patients ranged in age from 21 to 61 years (36.1 ± 17.8 years), and they had an average disease course of 10 months (2–16 months). Among these patients, tuberculosis was found at L2–L3 in 7 patients, at L3–L4 in 10 patients, at L4–L5 in 6 patients, and at L5–S1 in 8 patients. In addition, 6 patients had lower extremity numbness and weakness, and 20 patients had low fever in the afternoons. The major clinical manifestations were lower back pain with average visual analog scale (VAS) scores of 6.6 ± 1.4. According to American Spinal Injury Association (ASIA) grading system, 25 patients were categorized as grade E and 6 patients were categorized as grade D. The preoperative purified protein derivative (PPD) experiments showed +++ in 12 patients, ++ in 13 patients, and + in 6 patients. In addition, the erythrocyte sedimentation rate was normal in 6 patients and 28–130 mm/h in the other 25 patients. The preoperative C-reactive protein (CRP) concentration was 7–210 mg/L. All the patients underwent preoperative X-ray, CT, magnetic resonance imaging (MRI) examinations, and percutaneous puncture biopsy. The examiners found paravertebral abscess in 22 patients, iliac fossa effusion abscess in 9 patients, and kyphosis with average regional kyphosis angle (RKA) of 21° ± 6° in 12 patients. All the patients received preoperatively quadruple anti-tuberculosis chemotherapy (isoniazid, rifampicin, ethambutol, and streptomycin, or pyrazinamide for patients allergic to streptomycin) for 2 weeks and were confined to bed rest. The preoperative erythrocyte sedimentation rate was controlled at < 50 mm/h in 24 patients, but > 50 mm/h in the other 7 patients due to greater iliac fossa abscess.
General information.
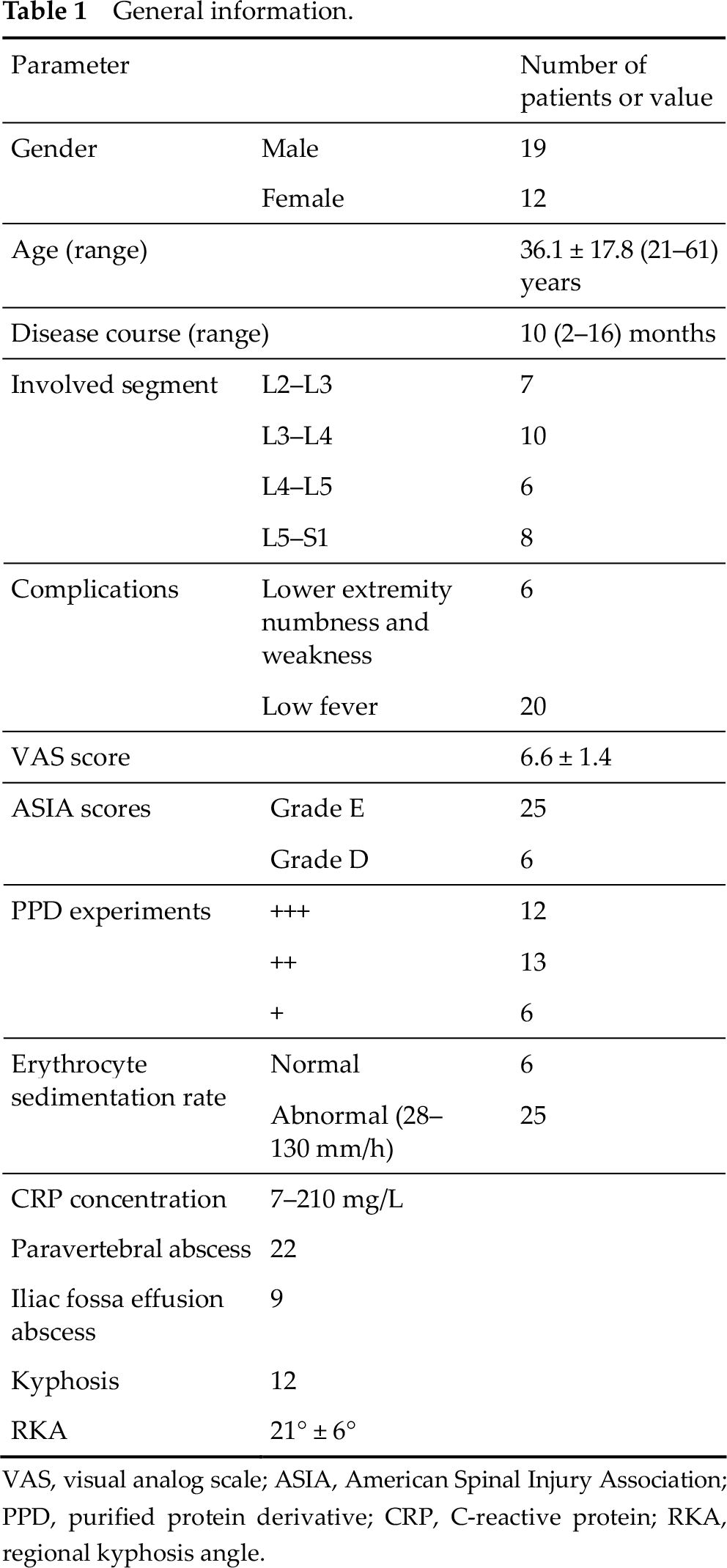
VAS, visual analog scale; ASIA, American Spinal Injury Association; PPD, purified protein derivative; CRP, C-reactive protein; RKA, regional kyphosis angle.
2.2 Surgical methods
The patients received systemic anesthesia and were placed in a prone position for minimally invasive posterior screw fixation using the percutaneous approach (for 18 patients) or Wiltse approach (for 13 patients). Those patients with preoperative kyphosis were corrected appropriately with posterior distraction. The patients were then placed in a lateral position for anterior focus debridement and bone graft and / or titanium mesh fusion.
2.2.1 Minimally invasive posterior internal fixation
The surgical procedure of minimally invasive posterior screw fixation via the percutaneous approach [7] includes the following steps: (1) Mark the position of the pedicle segment for screw placement according to the preoperative image. (2) Using C-arm anterolateral imaging, place the outer edge of the pedicle at the 9 o’clock position and place the puncture needle in the internal wall of the pedicle using Jamshidi trocar. (3) Confirm that the puncture needle safely penetrated the pedicle and reached the posterior margin of the vertebral body using the lateral imaging. (4) Replace the needle with the guide pin. (5) Place the pedicle screw and connecting rod with appropriate diameter and length along the guide pin (Fig. 1).
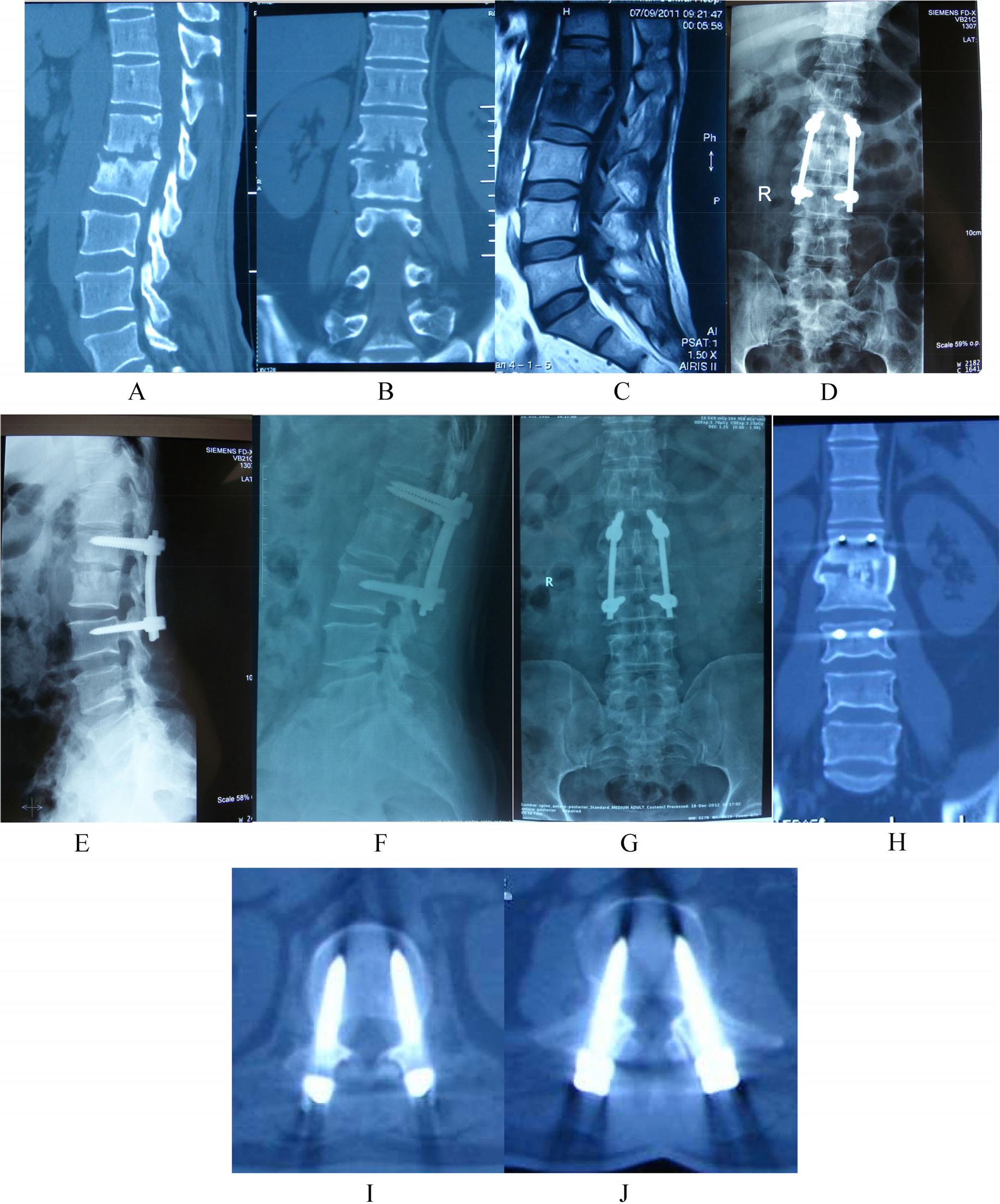
Images of a 50-year-old male patient with 4 months of lower back pain. He has been treated with focus debridement via anterior small incision, bone graft fusion, and minimally invasive posterior internal fixation via the Wiltse approach. (A)–(C) CT and MRI images showing tuberculosis at L1–L2. (D)–(E) CT and MRI images taken immediately after surgery. (F)–(J) CT taken at 1 year of follow-up showing satisfactory screw location and bone fusion.
The surgical procedure of minimally invasive posterior screw fixation via the Wiltse approach [7] includes the following steps: (1) Mark the position of the pedicle segment for screw placement according to the preoperative image. (2) Make an incision at the center of the segment to place the screw. (3) In turn, cut the skin from the incision, separate the subcutaneous tissue, and longitudinally open the thoracolumbar fascia from the gap between the multi-split muscle and the longest muscle to expose the articular process and the transverse process of the segment for screw placement. (4) Place the screws into the minimally invasive channel. (5) Prepare the channel for left L4 and L5 pedicle screws under direct vision. (5) Place the pedicle screw and the connecting rods with appropriate diameter and length (Fig. 2).
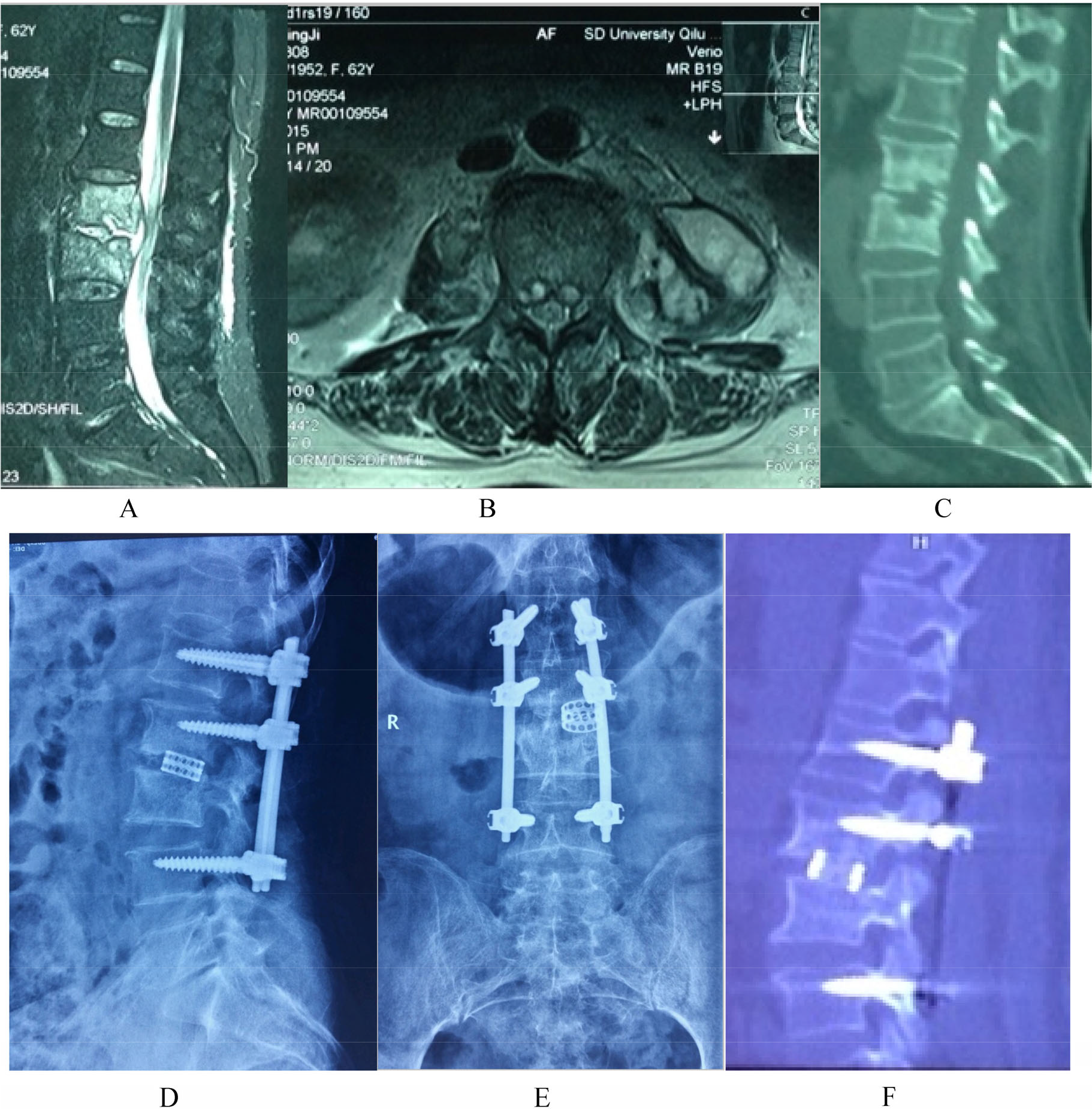
Images of a 62-year-old female patient with low back pain. She was treated with focus debridement via anterior small incision, bone graft fusion, and minimally invasive posterior percutaneous internal fixation. (A)–(C) CT and MRI images showing tuberculosis at L3–L4 and left paraspinal abscess. (D)–(F) CT taken at 1 year of follow-up showing satisfactory screw location and bone fusion.
2.2.2 Anterior focus debridement and bone graft fusion
The surgical procedure includes the following steps: (1) Place the patients in the lateral position. (2) Approach the lesion through the severe diseased side of the vertebral body or from the side with larger psoas muscle abscess. (3) Gradually expose the lesion segment on the intervertebral disc as well as the upper and lower diseased vertebral body with efforts to protect or section the segmental vessels. (4) Accurately position the diseased segments using imaging monitoring. (5) Resect the diseased intervertebral disc as well as its upper and lower sequestrum, pus, granulation tissue, cheese-like material, and involved intervertebral disc. (6) Fully immerse the lesions using isoniazid and clean the residual cavity. (7) Implant bone grafts. (8) Select the filling autologous bone titanium mesh or large iliac bone graft with the appropriate length and place them in the lesion cavity. 9) Close the incision, place a drainage tube, and suture layer by layer.
2.3 Postoperative treatments
The drainage tubes were removed 24–48 h postoperatively. The patients were encouraged to perform strengthening limb functional exercises, and those who showed no significant lower back pain and had lower limb muscle strength at grade ≥ 4 were allowed to walk 10 days after surgery using a brace for 3 months. All the patients were treated with broad-spectrum antibiotics and standardized short-course chemotherapy (isoniazid, rifampicin, and pyrazinamide) for 10 months on average (ranged 8–12 months). In addition, all the patients underwent generalized supportive therapy and regular follow-up for liver and kidney functions. The patients were considered clinically cured if they had (1) no systemic and local clinical symptoms during follow-up; (2) normal or near-normal erythrocyte sedimentation rate; (3) disappeared abscess and recovered trabecular bone noted on X-ray or CT examinations; and (4) no recurrence 3 months after surgery [6].
2.4 Statistical methods
SPSS12 statistical software (SPSS Inc., USA) was used for performing the statistical analysis. The differences in VAS scores of low back pain and corrected angle of patients treated with different approaches were compared using a bilateral t test. P < 0.05 was considered to be statistically significant.
3 Results
The surgery time was 160–240 min and the average blood loss was 100–300 mL. One patient had a surgery site infection (SSI), and healed 2 weeks after medications were administered. SSI did not occur in the other 30 patients after one course of treatment. In addition, no related neurological dysfunction, vascular injury, and other complications occurred. The VAS scores at 3 days postoperatively were 1.3 ± 0.3 and 2.1 ± 1.4 for patients treated with percutaneous screws fixation via the posterior approach and Wiltse approach, respectively, showing significant differences (P < 0.05). The screws were placed accurately and no screw-related surgical complications were observed (Figs. 1 and 2).
Chest and back pain were relieved significantly at 3 months postoperatively, and the VAS scores of lower back pain were 1.4 ± 1.5, which were significantly lower than those scores noted before surgery (P < 0.05). The VAS scores of lower back pain reduced to 1 ± 0.7 at the last follow-up, which were significantly lower than those observed before surgery (P < 0.05), but demonstrated no significant difference with VAS scores at the 3-month follow-up (P > 0.05). The erythrocyte sedimentation rate (ESR) decreased to < 20 mm/h after surgery. The CRP concentration reduced to normal (< 10 mg/L) after surgery. The patients with neurological symptoms were restored to grade E and the patients with kyphosis had postoperative RKA corrected to 15 ± 5 (P < 0.05). All the patients were monitored for more than 1 year, with an average follow-up period of 36.8 months (ranged 12–72 months). At the time of the last follow-up, all the patients met the criteria for tuberculosis healing and had no lumbar kyphosis, internal fixation fracture, prolapse, titanium mesh collapse, and other complications (Table 2).
Postoperative information.
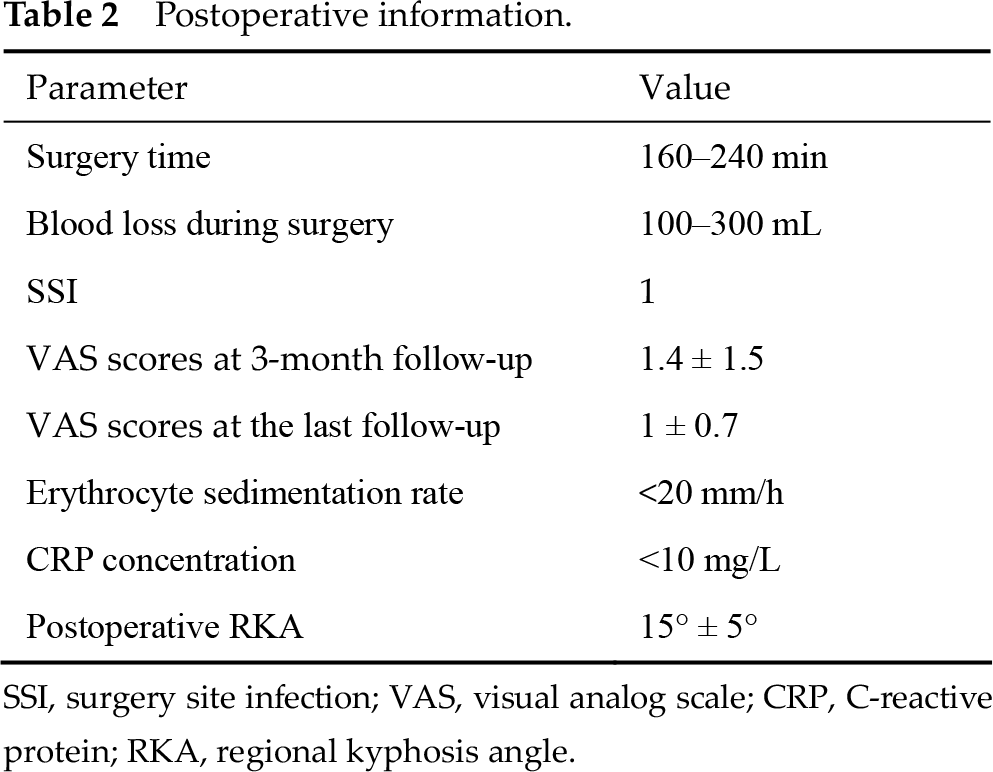
SSI, surgery site infection; VAS, visual analog scale; CRP, C-reactive protein; RKA, regional kyphosis angle.
4 Discussion
4.1 Surgical indications and timing selection [8]
Patients with (1) lumbar spinal tuberculosis which is difficult to control by conservative treatment and absorbed paravertebral flow injection abscesses; (2) medications for uncontrollable severe pain and nerve root irritation; (3) cauda equina dysfunction and bowel dysfunction; and (4) active tuberculous and stable kyphosis associated with corresponding clinical symptoms are generally treated surgically after anti-tuberculosis chemotherapy for at least 2 weeks. Patients with poor general conditions should be subjected to active supportive therapy before surgery. Patients with severe clinical symptoms, high ESR (> 100 mm/h) even after preoperative antithrombotic chemotherapy may also be treated surgically with additional perioperative intravenous isoniazid treatment. In this study, seven patients with iliac fossa injection abscess still had ESR > 50 mm/h after 2 weeks of anti-tuberculosis treatment. After surgery, their back pain and lower limb symptoms disappeared, ESR was effectively controlled, and they had no tuberculosis dissemination and other related complications.
4.2 Selection of surgical approaches
Adult lumbar tuberculosis is, for the most part, marginal tuberculosis combined with paraspinal and iliac fossa injection abscess without attachment involvement. Multiple surgical approaches can be used for such cases, but the use of anterior lesion removal is still the current mainstream surgical treatment. Single posterior lesion removal is also one of the surgical options.
4.2.1 Disadvantages of single anterior surgery
Single anterior surgery has obvious advantages. It can completely remove the lesion under direct vision. However, it has equally obvious disadvantages [9]: (1) When the old vertebral fracture is severe, the residual vertebral body after removal of lesions is insufficient to accommodate the vertebral screw, or strength of the vertebral screw fixation is not strong enough. Thus, normal residual vertebral body and intervertebral disc tissue are often needed, which virtually increases the scope of surgery and trauma; use of intersegmental fixation often results in loose internal fixation, fracture, and other complications, making renovation difficult. (2) During anterior exposure and surgery, there is a likelihood of injuring blood vessels, nerve root, and dural. Other complications due to sympathetic nerve injury such as reverse ejaculation, ureteral, peritoneal, and abdominal organ damage may occur. (3) For lumbosacral stability reconstruction, because of the deep sacral anatomy, internal fixation is more difficult. Thus, it is more likely to damage blood vessels.
4.2.2 Disadvantages of a single posterior surgery
The posterior approach has several disadvantages [10]. (1) The lesion was removed under indirect view. Blockage of dural mater and nerve root may make it difficult to ensure complete removal of the lesion. In addition, for patients with upper lumbar segmental lesions in combination with iliac fossa abscess, because the distance between the lesion and abscess is far, it is difficult to ensure the thoroughness of curettage. (2) Dural mater and nerve root blockage will make the reconstruction of lesions after removal more difficult. The placement of bone graft or titanium mesh is likely to damage the nerve structure, leading to certain neurological complications. (3) Focus debridement needs to destroy the involved undamaged articular process and joint, and has considerable impacts on the overall stability of the spine and bone graft fusion rate. (4) The exposure of the posterior approach has a greater impact on the paraspinal muscles, resulting in a higher incidence of postoperative residual back pain and other problems.
4.3 Characteristics of small incision anterior debridement, bone graft fusion, and minimally invasive posterior fixation
In summary, a single posterior surgery or a single anterior surgery has problems. Based on the characteristics of lumbar tuberculosis lesions, anterior small incision debridement and minimally invasive posterior fixation were applied. The approach combines the advantages of both anterior and posterior approaches, and overcomes partial shortcomings of the single posterior or the anterior approach.
4.3.1 Advantages of the surgical approach
The surgical approaches had several advantages [11]. (1) Focus debridement was performed through a small incision. If necessary, the incision can be expanded to ensure the thoroughness of lesion removal, reflecting the superiority of the anterior operation in focus debridement. (2) Using the posterior fixation effectively reduced the scope of the anterior approach to only vertebral destruction and the intervertebral space of the lesion, therefore reducing the incidence of complications related to anterior surgery. (3) When preoperative assessment showed that the vertebral remnant is enough, the pedicle screw can be inserted directly into the diseased vertebral body. If there is insufficient remnant, a pedicle screw can be inserted into the segment above the diseased body without resection of the residual vertebral body and intervertebral disc. When the fusion of the anterior graft is satisfied, the posterior screws can be removed to restore the function of the upper motor segment. Or a simple vertebral pedicle fixation can be used to assist the diseased pedicle and to increase the fixation strength. 4) Anterior reconstruction is relatively simple. Even for the lumbosacral segment, the anterior placement of a titanium mesh or iliac bone graft could have greater exposure and is not difficult to operate. 5) Minimally invasive posterior fixation ensures better fixation strength and reduces the effect of the posterior approach on the paraspinal muscles, articular facet joints, and other injuries. 6) When bone graft heals, the trauma caused by the removal of screws using the posterior approach is far less than that of the anterior approach.
4.3.2 Surgical shortcomings
Surgery requires intraoperative conversion from the prone position to the lateral position, which increases the surgery time.
4.4 Preoperative and postoperative issues must be considered
That tuberculosis is well controlled by using anti-TB agents is the premise of surgery. In the case that preoperative anti-TB agents are ineffective, alternative chemotherapy should be considered. Otherwise, the surgery will lead to treatment failure and tuberculosis recurrence. There are certain indications in the operation; thus, the patients with annex attachment are not suitable for the approach. For intervertebral disc fusion, more internal fixation segments may be needed. If bone conditions allowed, more screws may be placed into the pedicle to increase fixation strength. Because all the patients with combined lumbar kyphosis had active tuberculosis and more obvious spinal instability, most of them were subjected to posterior screw rod rotation or distraction to correct deformity initially, so as to facilitate the integration of anterior distraction. The patients in this study were treated using two minimally invasive internal fixations. Minimally invasive percutaneous screw fixation had smaller injuries and better postoperative VAS scores than pedicle screw fixation via the posterior approach. But minimally invasive percutaneous screws are more expensive and should be chosen according to the patient’s financial situation. Moreover, the patients should continuously receive standardized shortterm chemotherapy.
5 Conclusion
Under the premise of appropriate indications and treatments, minimally invasive posterior internal fixation combined with anterior focus debridement achieved satisfactory results for treating patients with lumbar vertebral tuberculosis. This approach can effectively reduce the exposure range and fusion segments in simple anterior focus debridement and internal fixation. The use of minimally invasive posterior pedicle screw fixation can effectively increase spine stability, reduce fusion segment, and decrease anterior surgical trauma and complications.
Footnotes
Conflict of interests
The authors declare that they have no conflict of interests.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81272024).