
Abstract
Background
Musculoskeletal injuries, such as neck and back pain, during a surgeon's career are common. However, studies on ergonomics are limited with regard to seated otolaryngologic procedures. Key elements of an ergonomic operating environment include the height of operating tables and surgical chairs. Surgeons benefit from proper support and positioning to prevent musculoskeletal injuries and reduce occupational risk.
Objective
The purpose of this study was to evaluate operating table and surgical seat heights, and determine whether adjustments can be made for various surgeon physiques.
Methods
Operating tables and surgical seat dimensions were measured at local hospitals, and the information was complemented by an online search of other models.
Results
Five unique operating tables and five unique surgical stools were identified, both in the local hospital and in a search on the Internet. Of available tables, the greatest range was 63.5–124.5 cm, which reaches above the maximum suggested working height of 76.2 cm. The surgical stool with the widest range was adjustable from heights of 50.8–72.4 cm. This combination of operative table and surgical stool provided the greatest range of heights.
Conclusion
Of the available tables and stools measured, the combination of surgical table with a range of 63.5–125.7 cm and surgical stool with a range of 50.8–72.4 cm provided the greatest versatility for diverse physician heights. In ergonomic terms, this combination may reduce physical fatigue and create a potentially safer working environment for seated surgeons.
Indeed, many head and neck surgeons experience significant discomfort in their practice. In a national survey of 325 otolaryngologists from the United Kingdom, 70% reported pain in the back, neck, or a combination of both. 5 Of those with pain, 53% attributed their symptoms directly to performing surgeries. 5 Another survey, on microlaryngeal surgery in the United States, found that 83% of otolaryngologists experienced musculoskeletal symptoms during surgery. 6 The severity of symptoms led surgeons to take breaks during surgery, seek medical treatment, or alter practice patterns, such as scheduling fewer surgeries or pursuing premature retirement.6,7 Similarly, another survey of otolaryngologists who performed endoscopic sinus surgery identified that 76% experienced physical discomfort associated with surgery. 8 Most notably, the study determined that only 9% of the respondents considered themselves at least moderately knowledgeable of ergonomic guidelines. 8
The prevalence of musculoskeletal symptoms among surgeons, including otolaryngologists, presents the need for research in ergonomics. Ergonomics refers to the scientific study of people at work and incorporates anatomy, engineering, physiology, and psychology. The goal of ergonomics is to reduce stress and eliminate injuries associated with muscle overuse, bad posture, and repeated tasks. 9 In the surgical setting, ergonomics is used to design workspaces, displays, and equipment to fit the surgeon's physical capabilities and limitations. Currently, studies related to proper support and positioning during seated otolaryngology procedures have not been explored as thoroughly as with laparoscopic procedures.10–13 Ergonomic insight will allow head and neck surgeons to make informed decisions and arrangements in their surgical environment to reduce physical strain and prevent occupational injuries. The purpose of this study was to determine whether optimal combinations of surgical beds and stools exist to create an ergonomic environment for the greatest number of surgeons when seated.
Methods
Surgical bed and stool manufacturers and models were identified at three hospitals affiliated with the University of Texas Health San Antonio, San Antonio, Texas. In addition, two common manufacturers were found online by using Medical Expo 14 for a total of five surgical tables and five surgical stools. The measurements of bed and stool dimensions were recorded in centimeters (cm) and inches (in), and were cross-referenced with product catalogs. Measurements for surgical stools included the range of seat height and armrest height (Figs. 1 and 2). The measurements for surgical tables included length, width, range of height, range of Trendelenburg and/or reverse Trendelenburg angles, and corresponding heights while angled (Figs. 3 and 4). In this study, we correlated the measurements of products readily available with those of a surgeon's ideal position defined by ergonomic studies of the workplace. Therefore, because this was a quality assessment study, institutional review board authorization was not required by the University of Texas Health San Antonio.

Sketch of minimum seat elevation and minimal armrest height.
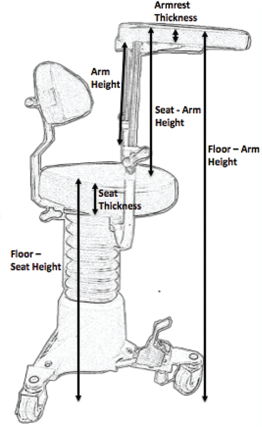
Sketch of maximum seat elevation and maximal armrest height.

Sketch of an operating table at minimal elevation and Trendelenburg angle.

Sketch of an operating table at maximal elevation and minimal Trendelenburg angle.
Results
Surgical Stools
The results of five commercially available surgical stools that are used by otolaryngologists are summarized in Table 1. The average seat height in the lowest position was 51.6 cm (20.3 in) with range of 48.3–53.34 cm (19.0–21.0 in), and the average seat height in its highest position was 71.9 cm (28.3 in) with a range of 68.6–73.7 cm (27.0–29.0 in). Armrest elevation was not reported for the online models. However, from those available in the hospital, the floor to armrest height ranged from 76.2 to 90.2 cm (30.0 to 35.5 in) at the lowest position, whereas the maximum elevation ranged from 105.4 to 116.8 cm (41.5 to 46.0 in).
Surgical seat measurements
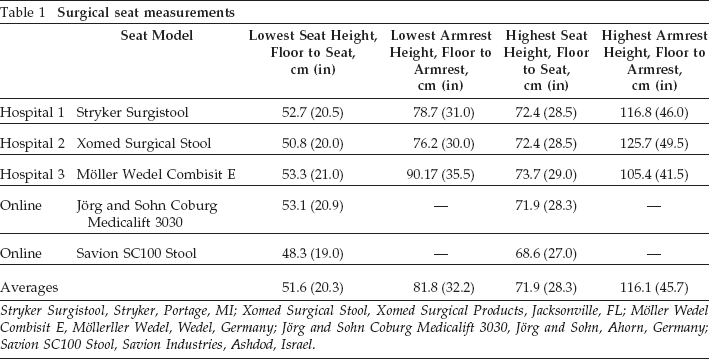
Stryker Surgistool, Stryker, Portage, MI; Xomed Surgical Stool, Xomed Surgical Products, Jacksonville, FL; Möller Wedel Combisit E, Möllerller Wedel, Wedel, Germany; Jörg and Sohn Coburg Medicalift 3030, Jörg and Sohn, Ahorn, Germany; Savion SC100 Stool, Savion Industries, Ashdod, Israel.
Surgical Tables
The results of five models of surgical tables used in otolaryngology are summarized in Table 2. Minimum table heights ranged from 59.9 cm (23.6 in) to a maximum elevation of 124.5 cm (49.0 in). Reverse Trendelenburg angles ranged from 0° to a maximum of 35°.
Surgical table measurements

Berchtold Operon D760, Berchotold Tuttlingen, Germany; Steris Amsco 3085 SP, STERIS, Mentor, OH; Berchtold Operon D850, Berchtold, Tuttlingen, Germany; Medifa-hesse GmbH and Co. KG 601700, Medifa-hesse GmbH and Co., Finnentrop, Germany; Merivaara Prometrix B3, Merivaara, Lahti, Finland.
Discussion
To date, to our knowledge, there are no universal guidelines on constructing operating tables or seats. Individual manufacturers use data from their own investigations to create operating room equipment. 14 This study attempted to develop ergonomic table and seat recommendations based on well-documented ergonomic guidelines for industrial workstation design and laparoscopic literature, and apply them to the otolaryngology setting. Integrating good ergonomic practices from industry and laparoscopic medicine should provide strong ergonomic standards for otolaryngology studies.
Diverse Surgeon Population
When designing a workplace, it is important to remember to accommodate the full range of body types. The optimal surgical environment for a woman in the 5th percentile of the population is different from a man in the 95th percentile. This study incorporated anthropometric measurements typically used in the industry (Table 3) to serve as a reference for operating table and seat design. These measurements help determine whether there is enough clearance for a surgeon to be seated and perform procedures comfortably on the operating table surface. Further, the armrest heights provide ranges for the surgeon to rest his or her arms comfortably during the surgery.
Summary statistics of the American population
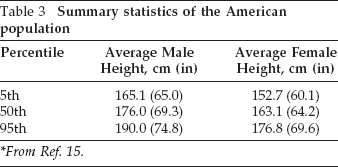
*From Ref. 15.
Operating Table Height
When considering an optimal ergonomic setting, certain elements of the operating room environment must be examined, such as monitor height and bed height.2,15,16 In contrast to open surgeries, minimally invasive surgeries direct the surgeon's vision away from the active site of surgery to the monitor, which contributes to visual strain in prolonged cases. Laparoscopic studies have shown that the optimal monitor position for reducing fatigue is ~1 m from the surgeon's eyes, at an angle that ranges from 0 to 15° downward from neutral.17,18 In a comparison of different visual displays, Kelts et al. 18 found that ceiling-mounted booms provided optimal heights to best accommodate the various gaze angles of surgeons of different heights.
In minimally invasive head and neck surgery, there is limited information on operating table and the surgical stool placement. However, the surgeon's position relative to the patient is critical. The working surface height relative to the height of the surgeon plays a major role in the potential for musculoskeletal injury. 2 Although the effects of table height on surgical outcome have not been formally studied, the surgeon may be forced to adapt physically to suboptimal conditions through adverse postural changes. Ramakrishnan and Montero 2 noted that a lower table height results in trunk flexion, whereas a higher one leads to effort and fatigue of the neck and upper extremities. Excess muscle loading correlates with work-related musculoskeletal injury. Thus, the ideal working height is a balance between spine position and arm position.2,19
According to literature published on industrial workstation design, the recommended working height ranges between 12.5 cm below and 2.5 cm above elbow height (–5 to 1 in). 20 As a result, the laparoscopic literature recommends a work surface height between 0 and 10 cm (0 and 4 in) below elbow height, with an upper arm elevation of 15–20°. 19 Although there were no data regarding the average physical features of surgeons or otolaryngologists, anthropometric measurements of the general population provided guidance on recommended table height for surgical procedures. The average male height at the 5th percentile is 165.1 cm (65 in), whereas the average female height is 152.7 cm (60.1 in). 21 At the 95th percentile, male and female average heights are 190.0 cm (74.8 in) and 176.8 cm (69.6 in), respectively. 21 Integrating the average population data with working height guidelines from laparoscopic studies implies that the operating table height should range from 64 to 77 cm (25 to 30 in) above the floor. 19 Thus operating tables at minimum should have the capability to reach 63.5 cm (25 in) from floor to the table so that surgeons can be seated and maintain a reasonable working height to perform procedures.
Of the five surgical tables studied, the Berchtold Operon D850 (Berchtold, Tuttlingen, Germany) (63.5 cm [25 in]) and the Merivaara Promerix B3 (Merivaara, Lahti, Finland) (61.0 cm [24 in]) have the capacity to lower the table height to 63.5 cm. The other surgical tables in this study may prove to be too high for the seated surgeon, even at their lowest height. In addition, the head of bed elevation with reverse Trendelenburg positioning is recommended in endoscopic sinus surgery for hemostatic benefit, which further challenges shorter surgeons when the table is unable to be closer to the ground.22,23
Surgical Stool
Many endoscopic and microscopic procedures in otolaryngology occur while the surgeon is seated, but there is a paucity of literature regarding surgeon ergonomics. Workplace design studies have shown that seated workers require less muscular activity to maintain posture, remain stable while performing precise maneuvers, have easier access to foot controls, and are subject to lower intravascular pressures. 20 In considering surgical stools, adjustment of seat height provides the surgeon the greatest vertical motion. Seat height should lower enough to allow the user's feet to be comfortably supported by the floor or a proper footrest while also raise sufficiently to permit perched hybrid sit-stand positions for the full range of male and female surgeons. BIFMA (Business + Institutional Furniture Manufacturers Association, Grand Rapids, MI) provides guidelines that suggest seat heights range from 39.4 to 50.5 cm (15.5 to 19.9 in). 21 None of the commercially available surgical stools evaluated in this study cover the entire recommended seating range. Further, BIFMA guidelines indicates armrest height ranges of 17.5–27.7 cm (6.9–10.9 in). 21 None of the surgical stools were able to fulfill this recommendation, and the minimum armrest height measured at the hospitals was 25.4 cm (10 in) with the Xomed Surgical Stool (Xomed Surgical Products, Jacksonville, FL).
The base of the surgical table may also be taken into consideration. Surgeons face limited range of motion as they attempt to maneuver their chairs near the midpoint of the operating table, where the base of the table is located. This is especially challenging for shorter surgeons operating on an obese patient in Trendelenburg or reverse Trendelenburg position. The base of the operating table may not allow the seated surgeon to reach the surgical field without poor postural compensation. Although some tables have the capability to swing 180° around, it still may not improve the surgeon's access near the table's midpoint, which is fixed by the base. Although not measured for in this study, awareness of this limitation may prove useful. Although none of the tables in this study had this feature, designing operating tables to move laterally to bring the surgical field closer to the surgeon may ameliorate this concern. However, this could introduce additional risk if the fulcrum created fails to accommodate weight imbalances.
Perched Position
The perched position is accomplished by raising the stool so that the surgeon has a 135° angle between his or her back and thighs. 24 This position is thought to decrease strain and thus improve body posture. Specifically, it preserved the natural anterior pelvic tilt and lumbar lordosis. 25 However, a contradictory study, conducted by Hamaoui et al., 26 reported the need for greater muscle activity of knee and ankle extensors when in the perched position. Although there are some conflicting data on the perched position, the combination of surgical stool and surgical table height should be able to accommodate for those surgeons who choose this position until clearer data evolves.
Optimal Combination for Surgical Table and Seat
Currently, no ideal combination exists for surgical tables and seats in ergonomics for otolaryngologists. In an effort to provide practical application, we defined the optimal combination for surgical table and seat as the greatest range of vertical maneuverability that can accommodate surgeons from the 5th to 95th percentile in height to perform seated surgery. The results of this study demonstrated the Berchtold Operon D850, along with the Xomed Surgical Stool, to have the greatest range of heights and positions. The surgical table goes as low as 63.5 cm (25 in), which is the minimum recommended working height for an operating table, and as high as 124.5 cm (49 in), well above the maximum suggested working height of 76.2 cm (30 in). The seat goes as low as 50.8 cm (20 in) to a maximum of 72.4 cm (28.5 in). This combination is optimal to accommodate a wide range of surgeons who plan to be seated and have enough clearance for the knees. With this range of vertical movement, the surgeon has the opportunity to be seated, perched, or standing while performing surgical procedures. The table can also be positioned flat and in reverse Trendelenburg angles as needed.
Limitations
The results of this study were subject to some limitations. First, this study did not represent an exhaustive review of every product available in each market segment. Three operating tables and surgical stools were measured at the hospitals. The remaining data were obtained from available specification sheets, and not all parameters were available from the manufacturers. Additional chairs and tables that meet the needs of the seated surgeon may be available. Second, it is possible that the ergonomic requirements for surgical stools differ from the office chairs. There are no ergonomic recommendations available on surgical stools. A formal study of the unique needs of operating surgeons would strengthen these findings. Third, this study emphasized the role of minimally invasive procedures in otolaryngology. Thus, not all procedures will be conducted while seated or while using armrests for support. Further studies are needed to elucidate optimal ergonomic positions for the diverse practices encountered in otolaryngology—head and neck surgery and for all seated surgeons.
Conclusion
Many otolaryngologists experience musculoskeletal pain and discomfort due to their surgical practice. Ergonomics in a surgical setting has become increasingly important with the advent of minimally invasive surgical techniques for otolaryngology procedures. Of the available tables and stools measured, the combination of a surgical table with a range of 63.5–125.7 cm (25–49.5 in) and a surgical stool with a range of 50.8–72.4 cm (20–28.5 in) provided the greatest versatility for diverse physician heights. In ergonomic terms, this combination may reduce physical fatigue and create a potentially safer working environment for seated surgeons.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article