
Abstract
Backgroud
Evidence about the relationship between prenatal maternal depression and the development of childhood asthma and allergies in early life is scarce. We aimed to examine this relationship by using data set of EDEN mother-child cohort study. A total of 1139 children were followed-up until the age of 5 years.
Methods
Prenatal maternal depression was self-reported by using the Centre for Epidemiological Studies-Depression scale (CES-D) questionnaire and was classified into binary variable (maternal depression [CES-D score of≥16] and no maternal depression [CES-D score of <16]). Asthma and allergies in the first 5 years were assessed by using the questionnaire of the International Study of Asthma and Allergies in Childhood (ISAAC). Adjusted odds ratio (aOR) was estimated for the relationship between prenatal maternal depression and early life asthma and allergies by marginal models through the method of generalized estimating equation (GEE) when adjusting for the confounders.
Results
In our study population, 13.67 % of the mothers had clinical significant depression (the total scores for CES-D ≥16) during pregnancy. For children ages 5 years, the prevalence of wheezing, physician-diagnosed asthma, physician-diagnosed eczema and allergic rhinoconjunctivitis were 46.78, 20.99, 29.17, and 22.54%, respectively. Prenatal maternal depression was associated with ever allergic rhinoconjunctivitis (aOR 1.87 [95% confidence interval {CI}, 1.33–2.62]). No significant relationships were found between prenatal maternal depression and wheezing, physician-diagnosed asthma and physician-diagnosed eczema (aOR 1.12 [95% CI, 0.91–1.39], aOR 1.23 [95% CI, 0.81–1.85] and aOR 1.17 [95% CI, 0.86–1.61], respecitvely).
Conclusion
Prenatal maternal depression was related to ever allergic rhinoconjunctivitis in the first 5 years of life in children of EDEN mother-child cohort study.
Recently, de Marco et al. 5 reported the impact of fetal exposure to maternal stressful life events during pregnancy on asthma and atopic diseases. An analysis of the results showed that children of mothers who had experienced stressful life events during pregnancy had a moderate risk of developing wheezing, asthma, eczema, and allergic rhinitis during their childhood. Cookson et al. 6 found that maternal anxiety during pregnancy (measured by anxiety scale of the Crown-Crisp Experiential Index) was related to asthma in children ages 7 1 /2 years. Recently, Guxens et al. 7 found that maternal psychological distress during pregnancy is associated with an increased risk of wheezing in children during the first 6 years of life, independent of paternal psychological distress during pregnancy and of maternal and paternal psychological distress after delivery. The purpose of our study was to explore the potential relationship between prenatal maternal depression and the risk of developing asthma and allergies in the first 5 years of life.
Methods
Study Population and Data Collection
In the EDEN (Étude sur les Déterminants pré et postnatals du développement de la santé l'ENfant) mother-child cohort study, we recruited 2002 pregnant women (at <24 weeks of amenorrhea) in two study centers of Nancy and Poitiers in 2003. A total of 1139 mother-child pairs were followed up until the age of 5 years (the sample size of our study). The criteria of noninclusion were the following: (1) twin pregnancy, (2) known diabetes before pregnancy, (3) planned to move outside of the region in the next 3 years, (4) not being able to speak or read French. Author contributions included the following: I. Annesi-Maesano and C. Zhou designed the study; C. Zhou, G. Ibanez, N. Baiz, and I. Annesi-Maesano collected and analyzed the data, and drafted the manuscript; and S. Banerjee, J. Just, V. Miramont, M. Steinecker, J. Chastang, and I. Annesi-Maesano read and approved the final manuscript.
Measurement of Prenatal Maternal Depression
To measure prenatal maternal depression, we used the self-reported Centre for Epidemiologic Studies-Depression scale (CES-D) questionnaire, which was completed by mothers between 24 and 28 weeks of amenorrhea. The CES-D had commonly been used for measuring depression during pregnancy.8,9 This self-administered questionnaire included 20 items, of which, each was scored from 0 (never) to 3 for (all the time). The score of each item was then added up into a total score, which ranged from 0 to 60. In the statistical models, maternal depression was classified into binary variable according to the total scores (maternal depression, CES-D scores of ≥16; and no maternal depression, CES-D scores of <16) by using the typically cutoff point of 16. 10
Measurement of Health Outcomes
Health outcomes were assessed by using International Study of Asthma and Allergies in Childhood questionnaires filled out by the parents for the period after the child's birth: 0–4 months, 4–8 months, 8–12 months, between 1 and 2 years, between 2 and 3 years, between 3 and 4 years, and between 4 and 5 years. For the analyses, the following health outcomes were considered: wheezing, physician-diagnosed asthma, physician-diagnosed eczema and allergic rhinoconjunctivitis at 1, 2, 3, 4, and 5 years. One health outcome was considered as present in the first year of life if it was reported at least once in one of the four questionnaire distributed in the first year of life.
At each period of follow-up, detailed questions were as follows: wheezing was defined by a “yes” response to the question of “Did your child ever have wheezing or whistling in the chest?” Ever physician-diagnosed asthma was defined by a “yes” response to the question of “Did your child have a diagnosed asthma by a physician?” Physician-diagnosed eczema was identified by “yes” responses to all of the questions of “Did you child ever have a physician-diagnosed eczema by a physician?” Allergic rhinoconjunctivitis was identified by positive answers to the following questions of “Did your child have a problem with sneezing or a runny or blocked nose when she or he did not have a respiratory infection (without a cold or nasopharyngitis or a flu)?” and “If yes, were those problems accompanied with lacrimation (tears) or itching (scratchiness) eyes?” 11
Statistical Analysis
The population characteristics are presented as means and percentages. Morbidity associated with asthma phenotypes was defined in terms of prevalence and incidence. Marginal models were used to measure the relationships between prenatal maternal depression and childhood asthma when adjusting for the covariates of the study center; maternal educational attainment; maternal smoking during pregnancy; maternal age at recruitment; maternal pre-pregnancy body mass index; siblings; gender of the newborn; and family history of asthma, eczema, allergic rhinitis, or food allergy. The marginal model was estimated by the generalized estimating equation approach by using exchangeable working correlation matrices. All the statistical tests were performed by using SAS statistical software version 9.2 (SAS Institute Inc., Cary, NC). All p values were two-tailed; p < 0.05 was considered statistically significant.
Statement of Ethics
This study was approved by the ethical committee (Comité Consultatif pour la Protection des Personnesdans la RechercheBiomédicale) of Kremlin Bicêtre and by the data protection authority (Commission Nationale de l'Informatique et des Libertés).
Results
Characteristics of the Study Population
The characteristics of all individuals in the recruited sample at the beginning of the study and the sample used in our study are described in Table 1. We followed up 607 boys (53.29%) and 532 girls (46.71%) until the age of 5 years. Among the sample of our study, 21.81% of the mothers smoked during pregnancy, and 13.67% of the mothers had clinical significant depression (the total scores for CES-D of ≥16) during pregnancy. Compared with the characteristics of all those in the recruited sample, the children followed up to ages of 5 years (the study sample of our study) had significantly different characteristics of the study center, maternal education attainment, maternal smoking during pregnancy, and prenatal maternal depression (p < 0.01), except for the characteristics of maternal age at recruitment; maternal pre-pregnancy body mass index; siblings; gender; and family history of asthma, eczema, allergic rhinitis, or food allergy.
Characteristics of all individuals in the recruited sample and individuals in the sample of our study
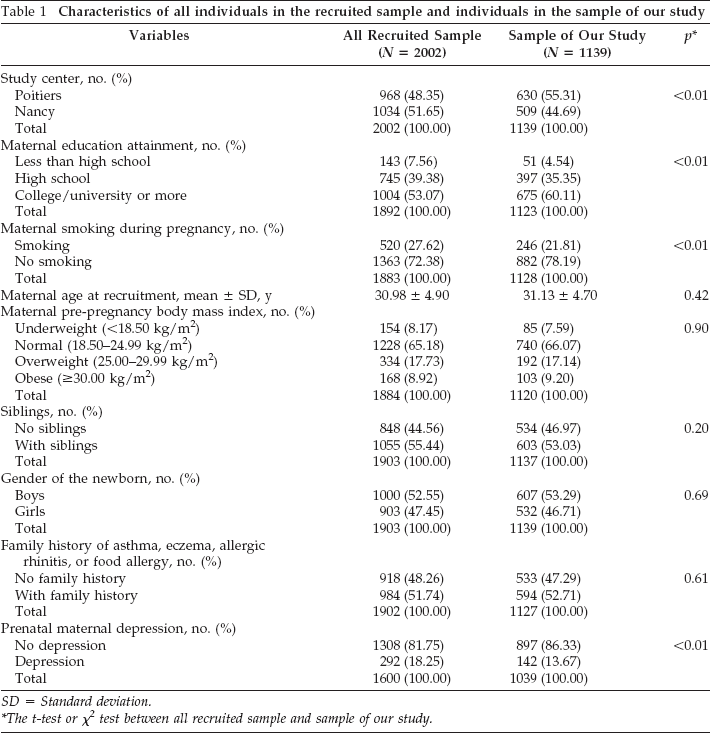
SD = Standard deviation.
The t-test or χ2 test between all recruited sample and sample of our study.
Health Outcomes in the First 5 Years of Life
The health outcomes in the first 5 years of life are presented in Table 2. For children at ages 5 years, the prevalences of wheezing, physician-diagnosed asthma, physician-diagnosed eczema, and allergic rhinoconjunctivitis were 46.78, 20.99, 29.17, and 22.54%, respectively; the incidences of wheezing, physician-diagnosed asthma, physician-diagnosed eczema, and allergic rhinoconjunctivitis were 2.13, 1.52, 1.42, and 2.94%, respectively. The relationships between prenatal maternal depression and health outcomes are presented in Table 3. There were significant relationships between prenatal maternal depression and the development of allergic rhinoconjunctivitis in the first 5 years of life of the children in the EDEN mother-child cohort study, whereas no significant relationships were found between prenatal maternal depression and the development of wheezing, physician-diagnosed asthma, and physician-diagnosed eczema.
Incidences and prevalences of health outcomes in the first 5 years of life

Relationships between prenatal maternal depression and health outcomes in the first 5 years of life

aOR = Adjusted odds ratio; CI = confidence interval.
The odds ratios were adjusted by potential confounders of the study center; maternal educational attainment; maternal smoking during pregnancy; maternal age at recruitment; maternal pre-pregnancy body mass index; siblings; gender of the newborn; and family history of asthma, eczema, allergic rhinitis, or food allergy.
Value in bold represent significant relationship was found for the prenatal depression during pregnancy and the corresponding health outcome.
Discussion
In our study population, 13.67% of the women had clinical significant depression during pregnancy and prenatal maternal depression was related to ever allergic rhinoconjunctivitis in the first 5 years of life.
Strengths and Limitations
The strengths of our investigation were that the sample was drawn from the general population and that our study was a longitudinal study, which allowed us to determine the potential causality between exposures and health outcomes. The limitation of our study was that both exposure and health outcomes were assessed by questionnaires and that reporting bias may have existed in the investigation. Another limitation could be that our study sample had fewer mothers with depression during pregnancy then the general French population. Therefore, the health effect of prenatal maternal depression on the development of childhood asthma and allergies may be underestimated. There also was a limitation in the different characteristics between all individuals in the recruited sample (which included those mother-child pairs who dropped out) and the individuals in the sample of this study (which excluded those mother-child pairs who dropped out) in study center, maternal education attainment, and maternal smoking during pregnancy; but the actual differences were not large, and not all of these three factors were found to be correlated to the health outcomes (only the study center associated with physician-diagnosed asthma, and smoking during pregnancy related to wheezing).
Prevalence of Prenatal Maternal Depression
Prenatal maternal depression is an important risk factor for the health of both mothers and infants, thus it has been considered a major public health concern. 12 Results of one study, 13 which recruited 579 women (average age, 29.37 years) in Bordeaux, France, indicated that 24% of the women presented with a highly intense depressive symptoms during pregnancy (assessed by CES-D). Results of another French population-based study showed that the prevalence rate of prenatal maternal depression (assessed by the Edinburgh Postnatal Depression Scale [EPDS]) was 18.3%. 14 Tandon et al. compared the sensitivity, specificity, and positive predictive value of the three tools of measuring prenatal maternal depression, viz. the CES-D, the EPDS, and the Beck Depression Inventory II. Analysis of the results showed that the three tools were accurate and reliable in detecting major and minor depression among low-income African American prenatal women. 15 The prevalence rates of prenatal maternal depression were 18.25 and 13.67% in all recruited women and in mothers whose children were followed up until the age of 5 years, respectively. This difference may be explained in that mother-child pairs with prenatal maternal depression in our study sample had more dropouts in the 5-year follow-up. The prevalence of prenatal maternal depression in our study was relatively lower compared with the reports (21.9%) by Tandon et al., 15 probably because of the difference of the characteristics of the study population. Our study recruited pregnant women from a general French population and with a relatively large sample size (n = 1136), whereas the study by Tandon et al. 15 focused on low-income African American women and had a small sample size (n = 32).
Relationships between Prenatal Maternal Depression and Childhood Asthma Prevalence
In our study, we focused on the influence of prenatal maternal depression on the offspring's development of asthma and allergies, disorders with complex etiologies. In previous studies, analysis of data indicated that maternal depression was associated with the development of asthma and allergy in children in Western countries.16,17 Wood et al. found that prenatal maternal depression (assessed by the EPDS) was positively associated with wheezing (two or more episodes) in children ages 12 months in the Urban Environment and Childhood Asthma birth cohort study. 16 Lefevre et al. assessed the relationship between maternal depression (investigated by using the Beck Depression Inventory Short Form Questionnaire) in early life and wheezing in children ages ≤3 years by using a case-control study design. Analysis of the results showed that there was a statistical link between maternal depression at the time of the survey (at age of 2 years) and infant wheezing but not for the relationship between prenatal maternal depression and wheezing (OR 1.55 [95% CI,0.12–19.8]). 17
In our study population, we found that prenatal maternal depression was the risk factor for ever allergic rhinoconjunctivitis in the children's first 5 years, which was consistent with results of recent studies.18,19 In the current literature, most studies report on the relationship between maternal depression and asthma in the offspring. Only a few studies considered rhinoconjunctivitis, as indicated in the unique systematic review of observational human studies on the topic. 20 In the two studies that dealt with allergic rhinitis discussed in this review,21,22 three of four analyses found positive associations, one significant. The adjusted odds ratios were between 0.96 and 2.38. More recently, in the GUSTO (Growing Up in Singapore Towards Healthy Outcomes) birth cohort, only prenatal anxiety was associated with child's rhinitis. 23 To sum up, our study provided new data about a birth cohort and maternal depression instead of anxiety. In addition, the existing studies are of diverse quality with wide definitions of often self-reported maternal events.
Of note, prenatal maternal depression was not found to be related to other phenotypes of asthma (wheezing, physician-diagnosed asthma, and physician-diagnosed eczema, with lower incidences compared with allergic rhinoconjunctivitis, as showed in Table 2), which is resistant with the findings by Lefevre et al. 17 The reason could be that our study population had a relatively lower prevalence of prenatal maternal depression because of dropouts of mother-child pairs with depressive problems, which probably underestimated the possible links and resulted in the nonsignificant relationships.
One potential explanation of the relationship between prenatal maternal depression and the development of allergic rhinoconjunctivitis could be that psychological factors may influence the immune system24–26 and favor the development of asthma and allergies. Another explanation could be that psychological factors may have a detrimental effect on the lung structure and function. 27 In addition, as presented in existing data, in utero life exposures were identified as important factors for the development of the structure and functions of the immune and respiratory systems28,29 and favor the further development of asthma and allergies. In utero exposures to psychological disorders as important exposures that influence the development of asthma and allergies of the children have been well documented in the literature.5,17,30,31 Recently, Khashan et al. 30 found that prenatal exposure to severe life events increases the risk of hospitalization for asthma in the offspring. The “fetal programming” theory, which indicates that in utero life exposures may alter expression of the fetal genome and may have lifelong consequences, has been used to further explain potential mechanism of the risk of in utero life exposures to asthma and allergies. This theory also considers that in utero life is a critical period and may have permanent effects on structure, physiology, and metabolism of the offspring.32,33
Conclusion
In the longitudinal study, prenatal maternal depression was associated with the development of childhood allergic rhinoconjunctivitis in the first 5 years of life, while the links were not found between prenatal maternal depression and wheezing, physician-diagnosed asthma, physician-diagnosed eczema. Those associations should be interpreted with caution as they may be underestimated for the dropouts of mother-child pairs with depressive problems. Further studies are needed to explain the magnitudes of these links according to different prevalence rates of prenatal maternal depression.
Footnotes
Acknowledgments
We thank the participating families, and the midwife research assistants (L. Douhaud, S. Bedel, B. Lortholary, S. Gabriel, M. Rogeon, M. Malinbaum) for data collection and P. Lavoine for checking, coding and data entry. We acknowledge all the funding sources for the EDEN study: Fondation pour la Recherche Médicale, French Ministry of Research: Institut Fédératif de Recherche program, Institut National de la Santé Et de la Recherche Médicale Nutrition Research Program, French Ministry of Health Perinatality Program, French Agency for Environment Security, French National Institute for Population Health Surveillance, Paris–Sud University, French National Institute for Health Education, Nestlé, Mutuelle Générale de l'Education Nationale, French Speaking Association for the Study of Diabetes and Metabolism (Alfediam) and National Agency for Research, and the Institute of Research in Public Health (Cohort program).
The authors have no conflicts of interest to declare pertaining to this article