
Abstract
Introduction
Inverted papillomas (IP) are benign sinonasal neoplasms, which account for 0.5–4% of all nasal tumors. IPs have been known to transform into squamous cell carcinoma in 5–15% of cases. Rarely, transformations to other malignancies have been reported. Here we report a unique case of malignant transformation of an IP into sinonasal undifferentiated carcinoma (SNUC).
Methods
A case report with a literature review; institutional review board exempted. The clinical presentation, radiographic features, surgical intervention, histopathologic analysis, treatment, and outcome of the case were examined.
Results
A 62-year-old man presented with a 3-month history of nasal airway obstruction, rhinorrhea, and postnasal drip refractory to medical therapy. He had a long history of exposure to fumes, chemicals, dusts, and solvents as a professional painter as well as a 45 pack-year history of smoking and alcohol abuse. The patient was ultimately found to have a left ethmoidal IP with a focus of malignant transformation into SNUC. Endoscopic resection was performed, followed by concurrent chemoradiation and adjuvant chemotherapy. After surgery, he had no evidence of recurrent disease after 9 years of follow-up.
Conclusions
IP is known to transform into squamous cell carcinoma. Here we report a rare case of malignant transformation into SNUC, a much more uncommon and aggressive lesion. Although traditionally associated with a poorer prognosis, the positive outcome for SNUC observed in this patient may potentially be attributed to early detection and timely therapeutic intervention.
Case Report
A 62-year-old man initially presented to his primary care physician with a 3-month history of bilateral nasal airway obstruction (left greater than right), intermittent facial pressure, rhinorrhea, and postnasal drip. The patient was subsequently treated with multiple courses of antibiotics and topical and systemic steroids as well as saline solution irrigations, with only temporary relief. The patient was then referred to the rhinology service in January 2007 for further management of presumed chronic rhinosinusitis. Although the patient continued to have persistent sinonasal symptoms, he did not have any headache, facial pain, epistaxis, numbness, visual changes, or anosmia. However, his occupational history was significant for long-standing exposure to fumes, chemicals, resins, dusts, and solvents as a professional painter. He also had a 45 pack-year history of smoking and admitted to drinking 4–5 highballs daily for the past 40 years.
On nasal endoscopy, the patient was found to have a large polypoid mass that occluded the entire left nasal cavity from the roof to the floor of the nasal vestibule. On the right, an inferior septal spur was seen, along with polypoid changes of the mucosa of the lateral nasal wall. Polyps were seen in the middle meatus but were not as extensive as the contralateral side. A biopsy of the left nasal mass was performed in the clinic, which showed hyperplastic surface epithelium associated with acute and chronic inflammation and reactive atypia. There was no evidence of malignancy on histopathologic examination. A sinus computed tomography also was obtained, which showed partial opacification of the ethmoid sinuses bilaterally, complete opacification of the left maxillary sinus, and mucosal thickening of the right maxillary and bilateral sphenoid sinuses. The Lund-McKay score was 11 of 24 (Fig. 1).

A preoperative computed tomography was obtained, which showed partial opacification of the ethmoid sinuses bilaterally, complete opacification of the left maxillary sinus, and mucosal thickening of the right maxillary and bilateral sphenoid sinuses (Lund-McKay score of 11/24).
In February 2007, the patient was taken to the operating room for bilateral endoscopic sinus surgery. Specifically, maxillary antrostomies and total sphenoethmoidectomies were performed bilaterally, including complete resection of the left sinonasal lesion. During surgery, polypoid tissue was not only seen filling the nasal vestibule on the left but also extending into the anterior and posterior ethmoid cavities as well as the sphenoethmoidal recess. The left maxillary sinus was also filled with polyps and mucopurulent material, all of which were removed with curved instrumentation. No polypoid tissue was seen in the left sphenoid sinus, and no discrete attachment site was appreciated at the time of surgery. In addition, no frontal sinusotomy was performed because the frontal recess and sinus were clear of any polypoid inflammation both on nasal endoscopy and imaging. Interestingly, on the right side, the patient was also found to have copious polyps within the maxillary sinus as well as the anterior and posterior ethmoid cavities. However, the polyps did not fill the nasal vestibule and were not as extensive as the contralateral side. Specimens from both sinonasal cavities were then sent to pathology.
Histopathologic analysis of the tissue from the right sinonasal cavity showed findings consistent with benign inflammatory polyps. However, the specimen from the left side demonstrated two concurrent processes, inverted schneiderian papilloma with a focus of malignant transformation into SNUC (Fig. 2 A–D). The focus of undifferentiated carcinoma was found deep in the stroma of the IP, with the contour of the IP preserved. The focus also showed a syncytial-type grown pattern, with a high nuclear-to-cytoplasmic ratio. The cells were dark blue in appearance, with round-to-oval nuclei that contained vesicular nuclear chromatin and small nucleoli. Mitoses were markedly increased within the focus of SNUC. There was no squamous or glandular differentiation. Immunohistochemistry was performed. The neoplastic cells showed a strong pan-cytokeratin reaction and a positive result for cluster of differentiation 56 but negative results for S100 protein, Human Melanoma Black 45, chromogranin, synaptophysin, tumor protein 63, cytokeratin 5/6, CD45RB, desmin, and smooth muscle actin consistent with SNUC. HPV testing results were negative.
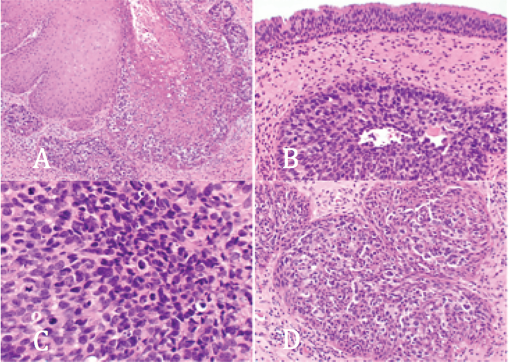
(A) A sinonasal papilloma (inverted type) is partially overtaken by a neoplastic population of undifferentiated cells; these have a dark blue appearance, with clearing around the nuclei; the neoplastic cells expand in a pagetoid fashion. (B) The surface respiratory epithelium is uninvolved; deep within the stroma, a neoplastic island of undifferentiated cells within the contour of an inverted sinonasal papilloma can be seen. (C) The sinonasal undifferentiated carcinoma component shows a syncytial-type growth, a high nuclear-to-cytoplasmic ratio, with nuclei that are round to oval with open-to-vesicular nuclear chromatin and small nucleoli; mitoses, including atypical forms, are greatly increased. (D) Islands of immature and undifferentiated-appearing cells that have a high nuclear-to-cytoplasmic ratio and open, delicate nuclear chromatin.
The patient was then seen by a head and neck oncologist, and his case was presented to a multidisciplinary tumor board. Concurrent chemoradiation therapy was recommended. A postoperative positron emission tomography (PET) and computed tomography (CT) was performed before radiation and chemotherapy, which showed no evidence of distant metastasis. The patient was then treated with 70.29 Gy of radiation with concurrent cisplatin therapy. Combined treatment began on April 2, 2007, and concluded May 16, 2007. Cisplatin was administered over 1 hour once a week for 7 weeks throughout the treatment. Radiation treatment was completed over the same length of time 5 days each week for a total of 33 treatments. The patient did not require a break-in treatment at any time. He then underwent adjuvant chemotherapy after this initial treatment with four courses of cisplatin, docetaxel, and 5-fluorouracil, which concluded in September 2007. The patient was subsequently followed up by his rhinologist and his head and neck surgeon with serial nasal endoscopy examinations and imaging. Specifically, posttreatment magnetic resonance images were obtained in October 2007, April 2008, December 2008, April 2009, and June 2010, with no evidence of recurrent disease (Fig. 3). Postoperative PET/CT was also obtained in June 2008 and April 2009, without evidence of local or distant disease. There has been no evidence of recurrent disease after 9 years of follow-up on imaging or examination.

Postoperative magnetic resonance image 3 years after treatment with wide local resection, concomitant chemoradiation, and adjuvant chemotherapy; this scan shows no evidence of recurrence or sinonasal disease.
Discussion
SNUC has been reported in the literature as arising once from an OP but, to our knowledge, never before from an IP. 3 An IP is known to transform into SCC in a small subset of patients; however, transformation into other malignancies has also been identified on histopathology, including verrucous carcinoma and mucoepidermoid carcinoma,2,4 which both originated in the right maxillary sinus. The patient with verrucous carcinoma was treated with medial maxillectomy via a lateral rhinotomy approach. The patient reportedly did well, albeit with only 5 months of reported follow-up. Postoperative chemotherapy and radiation therapy were not performed in this case. In the case of mucoepidermoid carcinoma, the mass was excised with wide local excision surgically in a combined approach with Caldwell-Luc, followed by radiation with 6000 cGy. The patient had a recurrence at the skull base 2.4 years after treatment, which was treated surgically at that time. Surgical excision of IP is recommended with complete resection of the lesion, along with its site of attachment to prevent recurrence and malignant transformation as well as close monitoring after surgery for surveillance.5,6 It has also been advocated to drill the bone at the site of attachment to ensure complete resection. 5 The risk of recurrence and potential malignant transformation is thought to be greater if the lesion is incompletely resected.
In the case of this patient, he had exposure to both tobacco and organic solvents throughout his adult life as a professional painter. Results of some studies have indicated that exposure to organic solvents significantly increases the risk of developing IP.7,8 The effect has been shown to be dose dependent. 7 Interestingly, smoking as a co-exposure decreased the odds ratio in this particular study. However, the risk of IP in tobacco exposure (both former and current smokers) without exposure to organic solvents was found to be increased but not statistically. Other recent studies found that smoking history was associated with the risk of malignant transformation of IP to SCC as well as the risk of recurrence.9,10
HPV has also been named as a potential etiologic factor for the genesis of IP and also for malignant transformation to SCC. 11 However, in the case of primary SNUC, HPV has not yet been shown to play a role in pathogenesis. In the study by Wadsworth et al., 12 histologic samples of five patients with SNUC were analyzed, but no sample showed evidence of HPV DNA. However, two of the five patients did show p16 staining throughout the samples, which indicated that testing for p16 can be nonspecific and that HPV may not play a large role in the pathogenesis of primary SNUC, at least in this small sample size. 12
Primary SNUC is an uncommon, highly aggressive carcinoma of the sinonasal tract. It typically presents as a rapidly enlarging mass that can involve multiple sites, even with extension beyond the sinonasal tract. 13 Given that some tumors demonstrate small foci of squamous differentiation, it is theorized that these tumors also derive from sinonasal epithelium. 13 Even with aggressive treatment, primary SNUC has a poor prognosis for survival, and the median overall survival is 1.9 years. 14 The 5-year overall survival rate is 30%. The median survival of patients with these tumors that originate in the ethmoid sinus was calculated to be 1.7 years compared with tumors that arise from the nasal cavity, with patients having a median survival of 3.4 years. Survival is thought to be poor due to the tendency for patients to present late with unresectable disease. 14 However, our patient, interestingly, remained disease free even 9 years after therapy. Current practice for the surgical treatment of SNUC involves complete resection with wide exposure for postoperative surveillance.5,6 However, recently, there has been discussion that advocates for minimally invasive endoscopic resection, which showed similar outcomes. 15 Multiple investigators have advocated for multimodal treatment with surgery, chemotherapy, and radiation therapy due to the aggressive nature of the disease.16,17
On review of the literature, we only found one other case report of SNUC that arose from a schneiderian papilloma, in this case, an OP. 3 The patient was a 64-year-old man who presented with epistaxis and nasal obstruction. 3 Physical examination revealed a polypoid mass in the left nasal cavity, and biopsy results showed OP with areas of frank carcinoma in situ. 3 Surgery with left medial maxillectomy and neck dissection was performed, and postoperative radiation was given. The patient was determined to be disease free after surgery, with a follow-up of 14 months. 18 It is unknown the long-term disease status of this patient but, compared with the Surveillance, Epidemiology, and End Results (SEER) Program data, the median survival for SNUC arising from the nasal cavity is 3.4 years. For this reason, no conclusions could be made regarding treatment or behavior of SNUC that arises from OP.
In the case of the patient with SNUC that arose from an IP, his long–term disease-free survival was currently at 9 years, which was much higher than the reported median outcome for patients with primary SNUC, of 1.9 years. 14 Whether this was because of an intrinsic difference in the natural history of SNUC that arises from IP or whether it was due to there being only a small focus of SNUC involvement within a much larger tumor specimen is unknown. It is possible that, in this case, due to the overall large tumor burden because of the IP, this patient presented much more quickly than if he had only a small focus of primary SNUC in the ethmoid sinus. Unfortunately, because this entity is so rare and there are no other reported cases of SNUC arising from IP, no overarching claims regarding tumor biology or treatment can be made at this time. Whether the treatment choice can be de-escalated in cases of SNUC that arise from papilloma requires a much larger sample size.
Conclusion
IP is well known to have a propensity for recurrence and a potential for malignant transformation into SCC. To our knowledge, we report the first case of IP transforming into SNUC. Although organic solvents and tobacco exposure may have played a role in the development of IP and malignant transformation in this patient, much remains to be learned regarding the pathogenesis of this degeneration into SNUC. The prognosis of this case seems to be much better after maximal treatment than with the typical patient with primary SNUC. However, additional research is necessary to determine if the superior clinical outcomes stemmed from early diagnosis or inherent features of the tumor itself in the context of concurrent IP.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article