
Abstract
Objective
In this report, we presented a rare case of bilateral silent sinus syndrome (SSS) in an otherwise healthy 57-year-old man treated with functional endoscopic sinus surgery (FESS). A systematic review of the literature regarding bilateral SSS was performed.
Case Report
A 57-year-old man with well-controlled allergic rhinitis in the absence of previous surgery or trauma presented with bilateral SSS, which was successfully managed with bilateral FESS.
Methods
A medical literature data base search of the terms “silent sinus syndrome” “maxillary atelectasis,” “imploding antrum syndrome,” and “bilateral silent sinus syndrome” was performed. The results were then narrowed to include only relevant articles.
Results
Relevant articles included three case reports and two articles that describe or mention bilateral SSS. Of the three case reports found, two patients presented with bilateral SSS, whereas the third patient presented metachronously, with the contralateral SSS manifesting 4 months after presentation of the initial ipsilateral SSS.
Conclusion
The present literature regarding bilateral SSS is likely incomplete, and further investigation is required to provide greater insight into the prevalence of this disease. In this report, bilateral FESS was successful in resolving symptoms and preventing disease progression.
Case Presentation
A 57-year-old man with a history of well-controlled environmental allergies presented to our office with an incidental diagnosis of bilateral SSS on computed tomography (CT). The patient's symptoms, which consisted of postnasal drip and nasal obstruction, had been adequately managed with oral antihistamines and a combined intranasal antihistamine-corticosteroid spray. The CT had been requested by his primary care provider after a seasonal exacerbation of his environmental allergies. He did not have any previous facial trauma or facial and/or sinus surgery. A review of his medical history was noncontributory, and the patient was otherwise asymptomatic from a sinonasal standpoint. A noninfused CT of the paranasal sinuses was notable for marked displacement of the walls of both maxillary sinuses, with bilateral maxillary sinus opacification (Fig. 1). Nasal endoscopy was significant for bilateral laterally displaced uncinate processes and medial maxillary walls. Results of an external examination were remarkable for a left-sided hypothalamus. Extraocular movements were intact bilaterally. The patient did not have limitations in visual acuity or diplopia. The patient underwent bilateral maxillary antrostomy, total ethmoidectomy, and dissection of all cells to the level of the frontal recess to establish an adequate drainage pathway at the level of the frontal sinus, without complication. The patient was administered our standard postoperative medical regimen of oral antibiotics, oral steroid taper, and budesonide sinus rinse. The patient's postoperative course was uneventful.

Preoperative computed tomography (CT) of the paranasal sinuses. Axial (A) and coronal (B) cuts of a noninfused preoperative CT of the patient's paranasal sinuses. (B) The scan is significant for bilateral maxillary sinus opacification, with marked displacement of the medial maxillary wall and uncinate processes best appreciated on the coronal view. The orbital floor is likewise inferiorly displaced bilaterally. (A) There also is marked displacement of the left posterior and lateral maxillary walls with significant attenuation of the bone. The left pterygopalatine fossa (PPF) is notably enlarged as a result of the inward displacement of the posterior maxillary wall. (A) Preservation of the fat plane within the PPF distinguishes this disease entity from tumors arising from this space.
Methods
A search of the PubMed and OVID (Wolters Kluwer group, New York, NY) data bases for studies on bilateral SSS was performed (Fig. 2). Key terms searched included “silent sinus syndrome,” “bilateral silent sinus syndrome,” “imploding antrum syndrome,” and “maxillary atelectasis.” Because SSS is a rare entity, no restrictions on year of publication were applied. All articles not dealing with primary or bilateral SSS were excluded. As this study maintained patient anonymity and did not alter the nature of the patient's management, the need for ethical approval was waived.
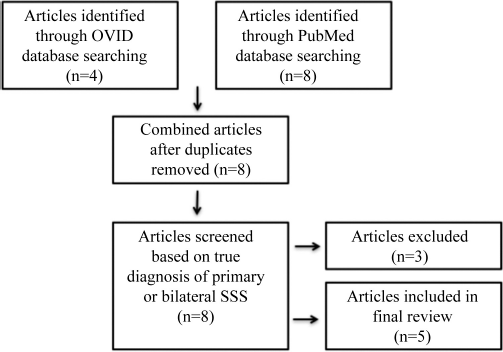
Flowchart of literature review.
Results
Our literature search revealed seven articles related to the subject of bilateral SSS.3–9 An article by Liss et al. 8 was excluded because SSS in this context occurred subsequent to surgery and chemoradiotherapy for a sinonasal malignancy. The case did not therefore meet criteria for primary SSS. 11 A second article was excluded because it comprised a letter to the editor that addresses the secondary nature of SSS described in the case report by Liss et al. 8 Five articles were included in our search, the first being a case by Suh et al. 3 in which a diagnosis of bilateral SSS was made incidentally on CT. In this report, a 29-year-old male patient had a history of allergic rhinitis and recovered well after FESS, without complications. 3 A second case, by Ferri et al., 4 describes a 27-year-old woman with radiographic evidence of contralateral SSS discovered 4 months after a maxillary antrostomy for an initial unilateral SSS. A third case, by Gunaratne et al., 9 describes an acute onset of symptomatic SSS after an upper respiratory infection. The fourth article, by Kass et al. 5 lists two instances of bilateral SSS without providing further clinical details regarding presentation and/or disease management. The last article describes balloon sinus dilation as a treatment modality for chronic maxillary atelectasis. 6 Imaging of one case in which bilateral SSS was present was provided but no further clinical details were provided. 6
Discussion
SSS was conceived as a unilateral phenomenon since its initial description in 1964.3,10,11 Our case and a review of the literature highlighted the potential for SSS to manifest as a bilateral phenomenon, be it is rare, nonetheless.7,9 Criteria for SSS include (1) a spontaneous change in the appearance of the eye; (2) the presence of ipsilateral enophthalmos and hypoglobus; and (3) radiographic findings, including maxillary sinus atelectasis with complete or partial opacification of the affected maxillary sinus. 3 Maxillary sinus atelectasis results in a potentially irreversible increase in orbital volume with eventual enophthalmos and hypoglobus. 12 It is likely that bilateral SSS is underreported because bilateral enophthalmos and hypoglobus may be more difficult to appreciate clinically in the absence of obvious asymmetry.
Ultimately, the rarity of this disease limited our understanding of the development of bilateral SSS. Our case, however, shared similarities with that of Suh et al., 3 in which a patient with chronic rhinosinusitis developed bilateral SSS and recovered well from FESS. The difference in presentation of our case to that of Ferri et al., 4 of the patient's metachronous disease evolution raised the interesting question of a potential temporal relationship of bilateral SSS. It is conceivable that all cases of bilateral SSS occur in a staggered fashion, yet our patient and the patient of Suh et al. 3 underwent imaging after the period of time required for the disease to manifest bilaterally. If this is the case, then more research is necessary to determine the temporality of bilateral SSS because this could be paramount in identifying bilateral cases on follow up of unilateral SSS. Further efforts should be directed at increasing the awareness of bilateral SSS in addition to determining its exact prevalence.
Conclusion
The present literature regarding bilateral SSS is likely incomplete, and further investigation is required to provide greater insight into the prevalence of the disease. In this report, bilateral FESS was successful in resolving symptoms and preventing disease progression.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article