
Abstract
Background
Inflammatory injury of nasal respiratory mucosa is a common feature of multisystem autoimmune disease. Certain autoimmune disorders are associated with nasal septum perforation (NSP). We performed a systematic review of the literature to better understand the association of NSP with specific autoimmune disorders. This is a case report of a 29-year-old woman with a history of arthralgia, autoreactive antibody titers, platelet dysfunction, and NSP. The constellation of symptoms and potential familial involvement indicated that the NSP in this patient was an early sign of an autoimmune disorder, an unknown autoimmune disorder, or a known disease with incomplete penetrance.
Methods
A systematic review of the literature was performed by two independent reviewers. Relevant articles were reviewed, and data that pertained to autoimmune-related NSP were extracted and analyzed.
Results
Overall, 140 cases of autoimmune-associated NSPs were reported. Granulomatosis with polyangiitis (48%), relapsing polychondritis (26%), and cocaine-induced midline lesions (15%) constituted 89.3% of the reported cases.
Conclusion
NSP is a potential sign of systemic disease. The identification of an NSP, especially in the context of other unexplained symptoms or workup suggestive of an autoimmune disorder, should prompt clinical evaluation for multisystem autoimmune disease with consideration of granulomatosis with polyangiitis, relapsing polychondritis, or cocaine-induced midline lesions.
Case Report
A 29-year-old woman with a history of beta thalassemia intermedia, Gilbert syndrome, asthma, fatigue, arthralgia, lower extremity numbness, alopecia, and high titer antinuclear antibody was referred to the otolaryngology clinic for daily nasal congestion and epistaxis. Her family history was significant for a paternal NSP. Nasal congestion was associated with itchy eyes and runny nose, which worsened in the fall and spring. Epistaxis after nose blowing occurred nearly daily since age 16 years. The patient also reported nasal crusting and whistling but denied intranasal trauma, nasal spray use, nasal surgery, intranasal drug use, or insufflation of other substances. A urine toxicant screen tested negative.
Visualization of the right and left nasal cavities by rigid nasal endoscopy revealed a 2-cm-diameter anterior septal perforation circumscribed with bloody crusting. The left inferior turbinate showed an anterior ulceration and dried blood. No polyps or purulence were observed. Results of a histopathologic examination of a nasal septal biopsy specimen demonstrated diffuse squamous metaplasia with moderate acute and chronic inflammation that extended into the adjacent cartilage. No evidence of vasculitis was observed. The patient also had a mild but consistent platelet aggregation defect over 3 years that could not be attributed to other causes. Platelet count, size, and granularity were within normal ranges, but platelet function assay results showed increased closure time and decreased aggregation with multiple agonists. No family history or other bleeding symptoms were recorded, and testing on two occasions showed no evidence of von Willebrand disease.
Inflammatory marker assays for C-reactive protein and erythrocyte sedimentation rate were within normal limits in at least two independent measurements. The patient tested negative for Treponema pallidum with independent modalities (rapid plasma reagin and fluorescent treponemal antibody absorption). Serum levels of thyroid stimulating hormone, free thyroxine, vitamin B12, and folate were within normal ranges. Antibodies against double stranded DNA, Smith antigen, ribonucleoprotein, anti-Sjögren syndrome antibodies A and B, perinuclear antineutrophil cytoplasmic antibody, centrally accentuated antineutrophil cytoplasmic antibody, myeloperoxidase 3, and proteinase 3 were negative.
Evaluations for rheumatologic diseases and testing for autoreactive antibodies remained inconclusive for an autoimmune disorder with a clear etiology. Despite being negative for standard perinuclear antineutrophil cytoplasmic antibody and/or centrally accentuated antineutrophil cytoplasmic antibody, the patient exhibited waxing and waning of autoreactive antibody titers, notably antinuclear antibody and atypical perinuclear antineutrophil cytoplasmic antibody. The constellation of arthralgia, autoreactive antibodies, and platelet dysfunction with potential familial involvement may indicate that NSP in this patient was an early sign of an impending autoimmune disorder, an unknown autoimmune disorder, or a known disease with incomplete penetrance.
Methods
To investigate the association between NSP and autoimmunity, two independent researchers (L.G. and K.P.) searched PubMed, Ovid (Wolters Kluwer, New York, NY), BioMed Central (Springer Nature, London, UK), Scopus (Elsevier B.V., London, UK), and U.S. National Library of Medicine (Bethesda, MD) by using a combination of “autoimmune*,” “autoimmunity,” “nasal sept*,” “septum,” “septal,” “septal perf*,” “nose,” “nasal,” “saddle nose,” and “rheumat*“ through November 23, 2015, without publication date restrictions. Duplicates were discarded, and abstracts that met search criteria were reviewed for relevance (Fig. 1). Inclusion criteria were human case series or case reports in English. Cases that only related to NSPs with no relationship to autoimmune disease or vice versa were excluded. Full text of reports that met search criteria were subsequently reviewed to extract the number of autoimmune-related NSP cases based on the specific autoimmune disorder. Sex and age data for included cases were also extracted. L. Guntupalli and K. Patel contributed equally.

Flow chart explanation of the systematic review of the literature.
Results
The initial data base search yielded 416 articles after excluding 76 duplicates and 56 withdrawn articles (49 from PubMed, 33 from Scopus, 323 from BioMed Central, and 2 from Medline Plus). A review of article abstracts yielded 106 remaining articles, and subsequent full text and reference analysis led to selection of 28 articles (Fig. 1). All articles except four were case reports or case series. Relapsing polychondritis,15–20 GPA,4,21–27 cocaine-induced midline destructive lesions (CIMDL),26,28–32 vasculitis,33,34 SLE,35,36 IgG4 related, 37 pyoderma gangrenosum, 38 STING-associated vasculopathy with onset in infancy, 39 chronic rhinosinusitis, 40 and Takayasu arteritis 41 were the reported NSP-associated autoimmune diseases (Fig. 2).
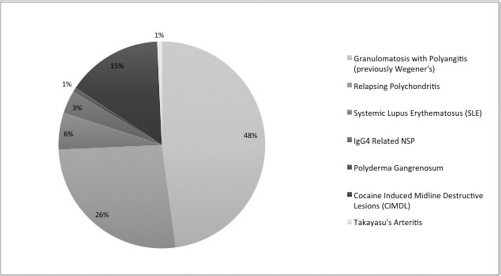
Percentage of reported cases of each autoimmune disease associated with a nasal septum perforation.
The 28 articles that met the search criteria described 140 cases of autoimmune-associated NSP (Table 1). The cases were divided based on the specific autoimmune disorder associated with the NSP. Eight articles described NSP associated with GPA, and six articles described relapsing polychondritis-associated NSP. Six articles reported NSP associated with CIMDL, and two described cases of unspecified vasculitis-associated NSP. NSP associated with immunoglobulin G4 (IgG4)-related autoimmunity, pyoderma gangrenosum, STING-associated vasculopathy with onset in infancy, Takayasu arteritis, SLE, and chronic rhinosinusitits each had one reported case. NSP was most commonly associated with GPA (67/140 [48%]), relapsing polychondritis (37/140 [26%]), and CIMDL (21/140 [15%]). SLE-associated NSP constituted 8 of 140 of the total cases (5.7%), and 5 of 140 cases (3.6%) reported IgG4-related NSP. A single case each described NSP associated with Takayasu arteritis (0.7%) or pyoderma gangrenous (0.7%) (Fig. 2). Twenty-one cases specified the sex of the patient. Ten were male (47.6%) and 11 were female (52.3%) patients. The most frequent age of presentation was between 30 and 40 years (n = 8 [42.1%]).
Demographic data and autoimmune disease composition in patients with NSP (N = 140)
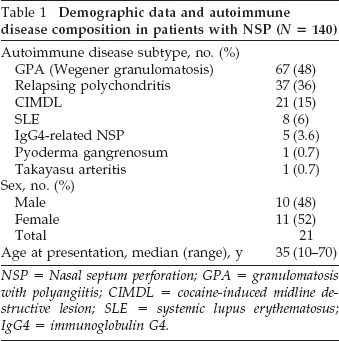
NSP = Nasal septum perforation; GPA = granulomatosis with polyangiitis; CIMDL = cocaine-induced midline destructive lesion; SLE = systemic lupus erythematosus; IgG4 = immunoglobulin G4.
Discussion
Our systematic review of the existing literature found that GPA, CIMDL, and relapsing polychondritis were the autoimmune disorders most frequently reported to be associated with NSP and to comprise 89.3% of reported cases of autoimmune-related NSP in the literature. This may indicate that, absent a clear diagnosis, preferential consideration can be given to GPA, relapsing polychondritis, or CIMDL during diagnostic evaluation if autoimmune-associated NSP is suspected. The small sample size of this study rendered age and sex data difficult to interpret. Available evidence, however, indicated a typically presenting patient may be 30 to 40 years old, with a slight female bias. Limitations inherent t this systematic review included reliance on case reports with a small sample size and a lack of prospective studies. Reporting cases of autoimmune-associated NSP within larger series that also included non-NSP cases reduced the amount of usable patient demographic data.
The patient in the presented case met 3 of 11 American College of Rheumatology SLE criteria: nasopha-ryngeal ulceration, arthritis, and antinuclear antibody positivity. 42 Interestingly, atypical perinuclear antineutrophil cytoplasmic antibody tested positive but did not replicate 20 weeks later. Anticardiolipin or lupus anticoagulant antibodies remain as the only untested SLE-associated antibodies listed in the American College of Rheumatology criteria. Positivity of either untested antibody would achieve 4 of 11 criteria, which is 85% sensitive and 96% specific for SLE. Cutaneous disease, a particularly well-recognized feature of SLE, was not observed in our patient; 41% of SLE cases, however, do not display cutaneous involvement. 43 Based on the literature review, relapsing polychondritis also remains a diagnostic possibility and should be considered given further cartilaginous involvement. 44 A negative urine toxicant screen, negative personal history of intranasal drug use, and positive family history of NSP reduces clinical suspicion of a CIMDL-associated NSP.
The possibility of false-negative results and laboratory error should also be given consideration in the diagnostic evaluation of autoimmune disease. Several cases of autoimmune diagnoses were initially found to be negative for disease-related antibodies only to test positive on repeated testing. A currently undiscovered autoimmune disease also remains a diagnostic possibility. As more specific and sensitive tests arise, it will be important to consider periodic re-testing for patients who are serologically negative and who fit the clinical picture for autoimmune disease. Conversely, autoreactive antibodies are found in only a subset of individuals who are asymptomatic, 45 and arthralgia is a common, nonspecific finding. A nonautoimmune cause of NSP, therefore, remains in the differential diagnosis for such patients.
Conclusion
The identification of an NSP, especially in the context of other unexplained symptoms or workup suggestive of an autoimmune disorder, should prompt clinical evaluation for multisystem autoimmune disease. GPA, relapsing polychondritis, and CIMDL should be preferentially considered in the differential diagnosis due to the higher reported frequency of NSP with these diseases. Our case presentation and systematic review highlighted the role of the vigilant otolaryngologist in the early detection of autoimmune disease and initiation of disease-modifying therapy.