
Abstract
Background
Malar augmentation is a common cosmetic procedure utilizing silastic materials. We describe an uncommon complication of a silastic implant eroding into the anterior maxillary sinus wall resulting in chronic rhinosinusitis (CRS).
Methods
A literature review is presented describing the presentation, surgical management and outcome of this uncommon adverse event.
Results
An 80 year old female with a history of bilateral cosmetic malar implants placed approximately 25 years ago presented to our office with a 4–5 month history of left-sided symptoms consistent with chronic sinusitis, and was found to have intrasinus penetration of her left malar implant. Only one other case series of 5 cases in 4 patients is reported in the literature.
Conclusions
Intrasinus malar implant migration is a rare complication of malar augmentation. The present experience suggests that removal of the offending foreign body often results in successful symptom resolution.
Case Report
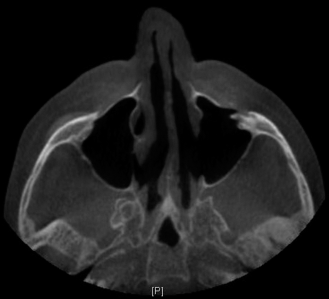
An 80-year-old woman with a history of bilateral cosmetic malar implants placed ~25 years ago presented to our office with a 4–5 month history of left-sided symptoms consistent with chronic sinusitis (nasal obstruction, postnasal drip, and purulent rhinorrhea). The patient's symptoms were refractory to multiple medical therapeutic modalities, including multiple courses of broad-spectrum antibiotics and oral and intranasal corticosteroids. Nasal endoscopy was noncontributory, with no evidence of pathology noted. Computed tomography (CT) imaging revealed intrasinus migration of the left malar implant with associated left maxillary sinus opacification (Fig. 1, A and B). The patient was taken to the operating room for left-sided endoscopic sinus surgery, including complete sphenoethmoidectomy, frontal sinusotomy, and a modified endoscopic medial maxillectomy, which permitted adequate visualization and instrumentation necessary for complete foreign body removal. The immediate postoperative course was uneventful, with both marked symptomatic and endoscopic improvement noted. At the 6-month postoperative time point, the patient was noted to have an ipsilateral, left-sided epiphora, which subsequently resolved after an endoscopic dacryocystorhinostomy procedure. A follow-up at 3 years after surgery demonstrated a well-healed sinonasal cavity, with complete symptom resolution. A postoperative CT (Fig. 2) demonstrated mucosal normalization of the maxillary sinus, with a patent outflow drainage pathway.

(A) Axial cut, bone window, noninfused computed tomography of the paranasal sinuses, demonstrating penetration of a malar implant through the left anterior maxillary sinus wall; there is evidence of mucosal thickening of the maxillary sinus, consistent with chronic sinusitis. (B) Magnified view of (A); note the hyperdense appearance of the malar implant relative to the sinonasal mucosa.
Axial cut, bone window, noninfused computed tomography of the paranasal sinuses acquired after surgery, demonstrating mucosal normalization of the left maxillary sinus; a patent sinus outflow tract is observed when following the endoscopic sinus surgery as described.
Discussion
Sinonasal complications that arise from silastic malar augmentation is an infrequently reported phenomenon. To our knowledge, there is a sole case series published at present, by Ginat and Schatz, 3 who describe five cases in four patients. Much like the clinical course described in this case series, our patient, likewise, presented with a delayed onset of symptoms 25 years after implantation. This was likely due to the relatively inert biologic reaction elicited by implanted silastic materials. Intrasinus implant migration is most likely a product of gradual erosion of the anterior maxillary wall secondary to pressure exerted by the implant. This would seem to explain why such a complication presents in such a delayed fashion relative to the time of implantation. Malar implants can have other various complications, more commonly, mal-positioning and, more rarely, infection. 4 Studies report an incidence of 2% and 1.2%, respectively. 5 Other complications include bleeding, hematoma, and seroma. Infraorbital nerve injury is also a potential risk.
Clinical workup of a suspected intrasinus migrated implant should include a high-resolution CT. Silastic implants have a hyperdense appearance on a CT with respect to soft tissue, although they appear less dense in relation to bone. 6 Given the foreign body reaction that arises from implant migration and subsequent mucociliary disruption, medical therapies are believed to be of limited benefit. Although the previous case series did not address the management of migrated implants, definitive management entails foreign body removal, which, in the context of the present case, may often be accomplished via an endoscopic approach. Extended intranasal approaches, e.g., an endoscopic modified medial maxillectomy, often provides sufficient visualization and surgical access, which permits complete foreign body removal. In the setting of a severely inflamed sinus and foreign body presence, all the sinuses were cleared of disease on the affected side to ensure removal of inflammatory burden as well as to allow improved placement of topical therapies for a prolonged postoperative time.
Conclusion
Intrasinus malar implant migration is a rare complication of malar augmentation, which typically presents in a delayed fashion, as in the current case, >2 decades after the original procedure. Correct diagnosis requires a comprehensive history-taking that elicits previous facial restorative procedures, in addition to an appropriate radiologic workup. The present experience, in agreement with previously reported cases, indicated that removal of the offending foreign body often results in successful symptom resolution.