
Abstract
Background
Vasomotor rhinitis (VMR) and irritable bowel syndrome (IBS) are two of the most widespread pathologies in industrialized countries, and they have a substantial impact on health-related quality of life.
Objective
To investigate the relationship between VMR and IBS to provide evidence to classify VMR and IBS as a sole disorder.
Methods
The study included 150 patients from San Salvatore Hospital, L'Aquila: 50 with VMR, 50 with IBS, and 50 healthy volunteers.
Results
With regard to a probable link between VMR and IBS, 62 patients of the whole population, 150 patients (413%) were affected by both VMR and IBS, 33 subjects (22%) were not affected by VMR or IBS, 25 patients (16.67%) only had VMR, and 30 patients (20%) only had IBS. When considering the 87 subjects affected by VMR, 62 of them also had IBS (71.26%). In turn, when considering all 92 subjects with IBS, 62 (67.39%) had VMR. We found a significant association among IBS and nasal obstruction, rhinorrhea, and turbinates, and among VMR and a change in stool consistency and abdominal pain. Among the patients affected by nonallergic rhinitis (NAR), we found a prevalence of NAR with eosinophils (31%) compared with the other cytologic types.
Conclusion
This study expanded the knowledge of the link between VMR and IBS, also the correlation between typical VMR symptoms and IBS, and about the correlation between typical IBS symptoms and VMR. For future implications, the diagnosis of NAR indicated the need to check for the presence of IBS, by using the Rome III criteria, and a diagnosis of IBS indicated the need to check for the presence of VMR. More studies are needed to find the pathogenetic mechanisms to explain the clinical correlation between VMR and IBS as seen in the present study.
Both conditions are characterized by a common autonomic dysfunction of nociceptive nerve sensors and by a neurogenic inflammation,5–33 but, because alterations of an autonomic system may occur in several organs, we wanted to study a relationship between VMR and IBS. Baraniuk indicated that non-allergic rhinitis (NAR) is only one part of a large pattern of autonomic and other mucosal organ dysfunction syndromes, e.g., gastroesophageal reflux, asthma, and IBS. 28 The aims of our study were to point out the link between VMR and IBS, and also the correlations between typical VMR symptoms (e.g., rhinorrhea and nasal obstruction) and IBS, and, moreover, the correlations between typical IBS symptoms (e.g., diarrhea and constipation and VMR). A further objective was to make a diagnosis of NAR subtypes by nasal cytology. With the aim of explaining the significant association between VMR and IBS, we hypothesize a multiple mucosal hyperresponsiveness to several stimuli.
Methods
A total of 150 subjects were recruited consecutively for this study, from April 2013 to September 2014, after obtaining informed consent: 50 patients with VMR (male-to-female ratio, 1:1) from the Ear Nose and Throat department of San Salvatore Hospital, L'Aquila; 50 patients with IBS (male-to-female ratio, 1:1) from the gastroenterology department of San Salvatore Hospital, L'Aquila; and 50 otherwise healthy volunteers (male-to-female ratio, 1:1) (Table 1). The inclusion criteria were diagnosis of VMR or IBS, and negative responses to skin-prick tests. The exclusion criteria were smoking and any other acute or chronic nasal and/or gastroenteric disease. All the subjects had to answer an examiner-guided questionnaire about their clinical history and nasal symptoms. They then had nasal fibroscopy and nasal cytology. We classified NAR subtypes by nasal cytology. Furthermore, all the subjects had to answer an examiner-guided questionnaire about the IBS, validated by the Roma III criteria. 34
Characteristics of patients

ENT = Ear Nose and Throat; GD = Gastroenterology Department; SD = standard deviation; BMI = body mass index.
Statistical Analysis
Descriptive analyses were conducted for all variables: habit characteristics, IBS symptom duration, the presence of mucus in the stool, nasal obstruction, rhinorrhea, and hyperemic and/or hypertrophic turbinates. The Shapiro-Wilk normality test was used for continuous variables to decide parametric or nonparametric tests in data analysis. For comparison of continuous variables in the three independent groups, the mean comparison test, analysis of variance, was used when the variables had normal Gaussian distribution, and the Kruskal-Wallis test for median comparison was used when the variables did not reach Gaussian distribution. A logistic regression univariate model was performed when VMR disease, IBS, and both were independently associated with symptoms. The variables nasal obstruction, rhinorrhea, and turbinates were dichotomized. The presence of obstruction included the persistence, periodicity, and presence or absence of sintomatology. The variable rhinorrhea included periodic or persistent symptoms. Turbinates were considered positive if they were hypertrophic and/or hyperemic (Table 2). Estimated associations were expressed by using odds ratio (OR) with 95% confidence intervals (CI), and a value of p < 0.05 was considered. Statistical analysis was performed by using the statistical package Stata/IC 12.1 (StataCorp LP, College Station, TX) (Table 3).
Synthesized descriptive analysis

ENT = Ear Nose and Throat Department; GD = Gastroenterology Department; IBS-D = irritable bowel syndrome with diarrhea; IBS-C = irritable bowel syndrome with constipation; IBS-M = irritable bowel syndrome-mixed.
Estimated associations expressed with OR (95% CI), and a value p < 0.05 was considered
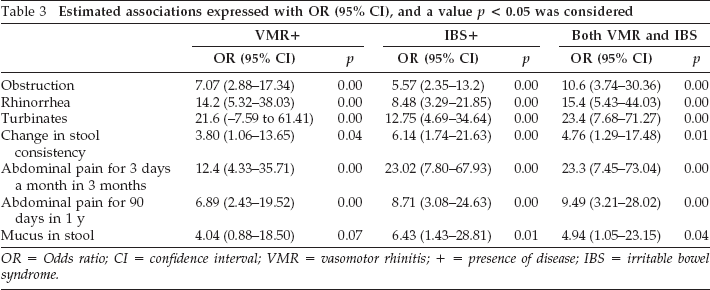
OR = Odds ratio; CI = confidence interval; VMR = vasomotor rhinitis; + = presence of disease; IBS = irritable bowel syndrome.
Informed Consent
The participants were given a consent form and were informed about the study and the standard of anonymization. The University of L'Aquila certified that the project study, to the best of its knowledge, qualified as an exempt study limited to the collection of clinical data and that the study had no more than minimal risk.
Results
No significant differences were recorded among the study groups with regard to age and body mass index. With regard to a probable link between VMR and IBS, 62 patients of the whole population, 150 patients (41.3%) had both VMR and IBS, 33 subjects (22%) did not have VMR or IBS, 25 patients (16.67%) had only VMR, and 30 patients (20%) had only IBS. When considering the 87 subjects with VMR, 62 also had IBS (71.26%). When considering all the 92 subjects with IBS, 62 (67.39%) of these patients had VMR. We found a significant association between VMR and IBS (OR 2.73 [95% CI, 1.38–5.37]; p = 0.004) (Table 4).
Patients with VMR, IBS, and both

VMR = Vasomotor rhinitis; IBS = irritable bowel syndrome; + = with VMR; - = without VMR.
Nasal Obstruction
We confirmed a significant association between VMR and nasal obstruction (OR 7.07 [95% CI, 2.88–17.34]; p = 0.001). Furthermore, nasal obstruction was significantly associated with IBS (OR 5.57 [95% CI, 2.35–13.2]; p = 0.001) and to both diseases (OR 10.6 [95% CI, 3.74–30.36]; p = 0.001) (Fig. 1).

Association of vasomotor rhinitis (VMR) and irritable bowel syndrome (IBS), and of both diseases with nasal obstruction.
Rhinorrhea
A significant association between VMR and rhinorrhea was confirmed (OR 14.2 [95% CI, 5.32–38.03]; p = 0.001). Moreover, a significant association between IBS and rhinorrhea (OR 8.48 [95% CI, 3.29–21.85]; p = 0.001) and this symptom and both diseases (OR 15.47 [95% CI, 5.43–44.03]; p = 0.001) was demonstrated (Fig. 2).

Association of vasomotor rhinitis (VMR) and irritable bowel syndrome (IBS), and of both diseases with rhinorrhea.
Turbinates
Hyperemic and/or hypertrophic turbinates were significantly associated with VMR (OR 21.6 [95% CI, 7.59–61.41]; p = 0.001), IBS (OR 12.75 [95% CI, 4.69–34.64]; p = 0.001), and both diseases (OR 23.4 [95% CI 7.68–71.27]; p = 0.001).
Change of Stool Consistency
A change in stool consistency was significantly associated with IBS (OR 6.14 [95% CI, 1.74–21.63]; p = 0.004), the present study has demonstrated that this symptom was significantly associated with VMR (OR 3.80 [95% CI, 1.06–13.65]; p = 0.04) and both diseases (OR 4.76 [95% CI, 1.29–17.48]; p = 0.01).
Mucus in the Stool
A significant association was confirmed between IBS and mucus in the stool (OR 6.43 [95% CI, 1.43–28.81]; p = 0.01) as well as with IBS and VMR (OR 4.94 [95% CI, 1.05–23.15]; p = 0.04) (Fig. 3).

Association of vasomotor rhinitis (VMR) and irritable bowel syndrome (IBS), and of both diseases with change in stool consistency and mucus in stool.
Abdominal Pain for at least 3 Days a Month in 3 Months
Results of the present study confirmed a significant association between abdominal pain at least 3 days a month in 3 months and IBS (OR 23.02 [95% CI, 7.80–67.93]; p = 0.001). Moreover, a significant association was also demonstrated between abdominal pain at least 3 days a month in 3 months and VMR (OR 12.44 [95% CI, 4.33–35.71]; p = 0.002) as well as with VMR and IBS (OR 23.33 [95% CI, 7.45–73.04]; p = 0.004).
Abdominal Pain for at Least 90 Days in 1 Year
A significant association between IBS and abdominal pain for at least 90 days in 1 year was confirmed (OR 8.71 [95% CI, 3.08–24.63]; p = 0.003). Furthermore, we have demonstrated a significant association between this IBS characteristic with VMR (OR 6.89 [95% CI, 2.43–19.52]; p = 0.01) with and with both diseases (OR 9.49 [95% CI 3.21–28.02]; p = 0.003) (Fig. 4). When considering all 150 subjects, 87 (58%) had NAR. All patients had a cell-mediated NAR, which was assigned to the type infiltrated by neutrophils (NAR with neutrophils, 27%), by eosinophils (NAR infiltrated by eosinophils [NARES], 31%), by mast cells (NAR with mast cells, 19%), and by both eosinophils and mast cells (NAR with eosinophils and mast cells [NARESMA], 23%) (Table 5).

Association of vasomotor rhinitis (VMR) and irritable bowel syndrome (IBS), and of both diseases with abdominal pain.
NAR subtypes for each group

NAR = Nonallergic rhinitis; ENT = Ear Nose and Throat Department; GD = gastroenterology department; NARES = NAR infiltrated by eosinophils; NARNE = NAR with neutrophils; NARESMA = NAR with eosinophils and mast cells; NARMA = NAR with mast cells.
Discussion
VMR comprises ~71% of NAR. VMR represents a global health problem that affects between 10 and 25% of the world population. The impact of the disease is often underappreciated with patients with VMR and results in significantly impaired health-related quality of life. Furthermore, this disease has a profound socioeconomic impact with direct medical costs and considerable indirect costs that relate both to absence from work and school, and reduced productivity. 1 Also, IBS has a high prevalence that ranges, for example, in North America, from 5 to 10%. 4 Patients with IBS have lower work productivity and higher absenteeism; they take more medications; and require more physician visits, diagnostic tests, and hospitalizations compared with patients of the same age and without IBS. 2
In the present study, a clinical relationship between VMR and IBS was demonstrated. The primary objective of our study was to investigate the link between VMR and IBS. We identified the presence of IBS symptoms in patients with VMR. In our study, the results indicated a significant association between VMR and abdominal pain for at least 3 days a month in 3 months as well as between VMR and abdominal pain for at least 90 days in 1 year. Furthermore, a significant association between VMR and a change in stool consistency was observed. Interestingly, we identified the presence of nasal symptoms in patients with IBS: a significant association between IBS and nasal obstruction, between IBS and rhinorrhea, and between IBS and hyperemic and/or hypertrophic turbinates was observed. A significant association with nasal obstruction, rhinorrhea, hyperemic and/or hypertrophic turbinates, a change in stool consistency, pain for at least 3 days a month in 3 months, and pain for at least 90 days in 1 year was detected in patients with both diseases.
The clinical association between VMR and IBS found in the present study, according to Baraniuk, 28 were shown by different studies with physiologic and pathologic correlations; there are studies that report neurogenic inflammation and autonomic dysfunction in both VMR 5 and IBS.6,7 Increased nociceptive C-fiber activity may lead to nasal dysfunction in idiopathic rhinitis 8 : neuropeptides (i.e., substance P and neurokinin A, calcitonin gene–related peptide, and gastrin-releasing peptide) are released from C-fibers by anti-dromic stimulation, which produces a localized increase in vascular permeability and nasal secretion.9,10 Central nervous system communication with the gut is mediated through the sympathetic and parasympathetic pathways of the autonomic nervous system by modulation of the enteric nervous system as well as via the hypothalamic-pituitary-adrenal axis. Activation of the axis takes place in response to both physical and psychological stressors, 11 both of which have been implicated in the genesis of IBS. 12
The high prevalence of IBS in NAR is important because of correlations of IBS subtypes with specific abnormalities in the enteric serotonin (5-HT) and dopamine systems as well as central pain, sympathetic autonomic, and parasympathetic autonomic nervous system. 30 The molecular defects of these syndromes may provide insight into potential subsets of NAR.31,32 Potentiation of 5-HT release and activation of 5-HT1P or 5-HT3 receptors have been linked to diarrhea-predominant IBS. Conversely, reduced release of 5-HT, desensitization of 5-HT4 prokinetic receptors, and reduced dopaminergic function have been implicated in constipation-predominant IBS.
The expression of transient receptor potential vanilloid 1 (TRPV1) has been found enhanced in upper airway hyperresponsiveness.15–18 Van Rijswijk et al. 19 note that repeated nasal provocation with capsaicin could significantly reduce nasal symptoms in patients with idiopathic rhinitis, which indicates either C-fiber desensitization, degeneration, or TRPV1 inactivation. Increased expression of the TRPV1 protein was demonstrated in mucosal nerve fibers of patients with IBS, which correlate with their pain symptom severity. 20 Keszthelyi et al. 21 postulated that postinflammatory upregulation of the TRPV1 receptor through increased biosynthesis in the nerve terminals of mucosal afferents, which resulted in increased nociceptive sensitivity, represented a mechanism potentially responsible for such sustained effect.
When studying chronic pain, Dray et al. 22 noticed that cytokines, including interleukin (IL) 1, IL-6, IL-8, IL-11, and tumor necrosis factor α, may induce hyperalgesia by acting via a common final pathway mediated by the induction of nerve growth factor from fibroblasts, keratinocytes, and neural Schwann cells, which may increase neural sensitivity to inhaled irritant factors. Administration of substance P to human nasal mucosa in vitro can increase cytokine expression. 23 Significantly increased levels of some proinflammatory cytokines, such as tumor necrosis factor α, IL-1β, and IL-6, were reported in patients with IBS. 24 Dinan et al. 25 reported that the serum concentrations of the proinflammatory cytokines IL-6 and IL-8 were elevated in all IBS subgroups (diarrhea predominant, constipated, and alternated periods wih diarrhea and constipation).
The discrimination between saprophytes- and foreign pathogens is mainly mediated by a family of receptors, termed pattern recognition receptors, which interact with specific ligands of the invading hosts (pathogen-associated molecular proteins). 26 Pattern recognition receptors are mainly expressed by epithelial cells, antigen-presenting cells, regulatory T cells, and other cells involved in the interaction between the immune system and the environment.27–29 Toll-like receptors (TLR) represent the major family of pattern recognition receptors. TLR activation triggers a cascade of reactions, which lead to increased expression of proinflammatory genes. 30 Lauriello et al. 25 pointed out that, in VMR, both TLR4 and TLR9 seemed to be significantly downregulated.8–31 Results of biopsy study 26 indicate that the expression of the TLR family is altered in IBS. TLR4 was increased in colonic mucosal biopsy specimens from patients with IBS compared with healthy controls.32,33
Also, we studied nasal cytology to make a diagnosis of NAR subtypes. All 87 patients with VMR were subdivided into NAR with neutrophils (27%), NARES (31%), NAR with mast cells (19%), and NARESMA (23%), and we found a predominance of NARES compared with the other cytologic types. The increased incidence of NAR with neutrophils was linked to physical and chemical aggression of the mucosa because the individuals most affected are factory workers, inhabitants of industrialized centers, and heavy smokers. The persistence of neutrophils and the release of chemical mediators (neutrophil elastase) are the main cause of formation of free radicals and consequent suffering mucosal epithelium. Patients with NARESMA and NARES had the worst quality of life. 35 Patients with NARESMA had a more-intense impairment of dry nose, snoring, and sore throat, whereas patients with NARES showed more-severe postnasal drip.
Conclusion
This study demonstrated the link between VMR and IBS. In particular, it showed a significant presence of typical VMR symptoms (e.g., rhinorrhea and nasal obstruction) in patients with IBS as well as typical IBS symptoms (e.g., diarrhea and constipation) in patients with VMR. This strong association can be explained when considering a common pathophysiologic pathway such as a chronic neurogenic inflammation. As future implications, the diagnosis of NAR suggests a need to check for the presence of IBS (by using the Rome III criteria 2 ), and the diagnosis of IBS indicates the need for evaluation of nasal symptoms and to perform nasal cytology with the aim of classifying the type of NAR. More studies are mandatory to find out the pathogenetic mechanisms to explain the strong clinical correlation between VMR and IBS as indicated in the present study.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article