
Abstract
Objective
Immunoglobulin G4 (IgG4) related sclerosing disease (RSD) of the paranasal sinuses is a rare lesion of dense lymphoplasmacytic tissue, with a high proportion of IgG4+ plasma cells. We presented a rare case of IgG4-RSD with isolated involvement of the paranasal sinuses in the absence of multiorgan involvement.
Methods
A case report and comprehensive literature review.
Results
To our knowledge, only 11 cases of IgG4-RSD with paranasal sinus involvement have been reported. Patients with IgG4-RSD commonly present with epistaxis and symptoms that mimic chronic rhinosinusitis, e.g., rhinorrhea, nasal obstruction, and facial pressure. On imaging, an expansive and erosive process is described. Surgery provides tissue for immunohistologic evaluation; however, there is a paucity of evidence about the direct extent of surgical resection or medical therapies. Postoperative steroids were typically started, although the regimen was not standardized.
Conclusion
Few cases of paranasal sinus IgG4-RSD have been reported in the literature. Evidence-based recommendations regarding treatment and surveillance of paranasal sinus IgG4-RSD are lacking; however, most reports describe systemic steroids as the mainstay of treatment. This single subject analysis, with a review of previously reported cases adds to the expanding body of data related to this rare disorder.
Quantitative cutoff values for the diagnosis of systemic IgG4-RSD*
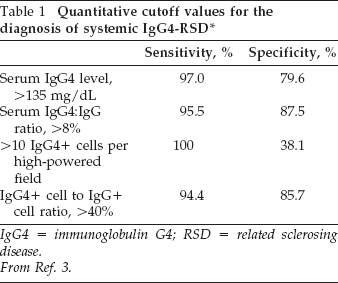
IgG4 = immunoglobulin G4; RSD = related sclerosing disease.
From Ref. 3.
Case Study
A 46-year-old man presented to the otolaryngology clinic with recurrent right-sided epistaxis, facial pain, nasal congestion, rhinorrhea, and nasal crusting for 1 year. Review of systems and results of basic laboratory investigations (i.e., complete blood count and comprehensive metabolic panel) were unremarkable, and, therefore, there was low suspicion for systemic disease. No serum IgG4 measurements were collected. High-resolution computerized tomography (CT) of the sinuses revealed a well demarcated but expansive mass of the right ethmoid sinus with erosion of the lamina papyracea (Figs. 1 and 2). There was no evidence of infiltration within the surrounding structures (i.e., periorbita or skull base). Intraoperative endoscopic visualization confirmed the presence of a polypoid mass that primarily involved the right ethmoid sinus with extension into the frontal recess and erosion of the lamina papyracea. The periorbita and skull base were uninvolved. The patient underwent endoscopic sinus surgery with excisional biopsy of the lesion.

Axial view of the soft-tissue lesion with osseous destruction at the anteroinferior right-sided lamina papyracea.

Coronal view, demonstrating erosion of the right lamina papyracea with maxillary outflow obstruction.
Results of a histologic analysis of the sinus lesion demonstrated dense infiltrates of plasma cells and fibrosis deep within the tissue. Immunostain for CD138, a generic plasma cell marker, labeled >50% of the visible cells (Fig. 3) and anti-IgG4 stains of the sinus lesion demonstrated >50% of the IgG4 subclass (Fig. 4). Postoperative management included oral antibiotics for 7 days, saline solution irrigations, and prednisone 30 mg per day for 4 weeks tapered by 5 mg per week until completed. Routine postoperative debridement in the office was performed. At 1-year of follow-up, there had been no endoscopic evidence of persistent or recurrent disease. All of the patient's symptoms had resolved, without the need for continued therapy.

CD138 immunostain, demonstrating plasma cell population within inflammatory infiltrate (anti-CD138 immunostain, original magnification ×200).

Immunostain for immunoglobulin G4 (IgG4) shows many plasma cells that contain the IgG4 subclass (anti-IgG4 immunostain, original magnification ×150).
Literature Review
A search of the literature located only 11 cases of IgG4-RSD with sinonasal involvement (Table 2). In 2009, Ishida et al. 5 described the first case of sinonasal IgG4-RSD. Including our case, IgG4-RSD of the paranasal sinuses affects men somewhat more often than women (7:5) and afflicts all age groups, with a mean presentation at 55.3 years (standard deviation, 21.6 years; range, 15–79 years). All reported cases describe patients with locally destructive disease, with the most common symptoms being nasal obstruction, epistaxis, and facial pain. The maxillary sinus was involved most commonly, followed by the ethmoid sinus and nasal septum. Alt et al. 6 reported isolated sphenoid sinus involvement with symptoms of constant frontal headaches. Ishida et al. 5 found concomitant parotid gland IgG4-RSD in addition to disease of the right maxillary sinus and nasal septum; however, isolated sinonasal disease was found in the remainder of patients.
Review of sinonasal IgG4-RSD

IgG4 = immunoglobulin G4; RSD = related sclerosing disease; hpf = high-powered field.
To establish the diagnosis, a tissue biopsy rather than primary resection was performed in the majority of patients. After surgery, a systemic steroid was immediately started in several patients; although the dosage and duration was not consistent. Alt et al. 6 noted recurrent and/or recidivistic disease 2 months after surgery of primary debulking; thus, fluticasone was initiated with no reported progression. Lindau et al. 7 and Prabhu et al. 8 described the use of rituximab in patients with poor response to oral steroids after biopsy.
Discussion
The prototype of IgG4-RSD has become IgG4-related sclerosing pancreatitis, also known as autoimmune pancreatitis. 9 Extrapancreatic pathology has been reported in many organ systems, including regions within the head and neck.10,11 Although most cases of IgG4-RSD are systemic, clinicians should be aware of possible isolated sinonasal disease. As in our case, most cases of paranasal IgG4-RSD report locally destructive disease. Many of the presenting symptoms mimic other forms of rhinitis or rhinosinusitis with rhinorrhea, nasal obstruction, facial pressure, and epistaxis being the most common. Based on symptomatology, this could prompt the clinician to initiate intranasal steroid sprays that possibly aid in the treatment of both rhinosinusitis and paranasal IgG4-RSD, thus potentially delaying the diagnosis.
Endoscopic biopsy for immunohistochemistry may be the primary role of surgery. A characteristic histologic appearance with marked plasma cell IgG4 expression supports a diagnosis of IgG4-RSD. Serum IgG4 levels are potentially misleading because IgG subtypes can be elevated in other inflammatory conditions.4,12 In the cases reviewed, most surgeons performed a tissue biopsy rather than complete excision of the lesion. In our case, a complete excision was performed. There does not seem to be a correlation between the extent of biopsy and disease recurrence (i.e., biopsy versus excisional biopsy). Therefore, it is unclear whether an at-tempt at surgical excision needs to be or should be performed.
Due to limited evidence, the management of sclerosing diseases that affect the sinuses is largely based on extrapolations from other organ systems. Currently, the suggested treatment for systemic IgG4-RSD is an oral corticosteroid taper over several weeks, the dose and duration of which is poorly defined. Except for two patients, in the cases reviewed, there were no recurrences or progression of disease reported in patients started on oral prednisolone soon after a tissue diagnosis. However, the follow-up time documented was not consistent or standardized, the sample size was small, and, therefore, an evidence-base recommendation was lacking. One case noted recidivistic disease 2 months after surgery, and fluticasone intranasal spray was started with no progression reported. 6 In cases isolated to the paranasal sinuses, a nasal steroid irrigation, e.g., budesonide 0.5 mg in 240 mL normal saline solution, could target nasal symptoms; although, this has never been studied or reported.
Disease surveillance should be directed by clinical examination and symptomatology, including endoscopic examination and, possibly, imaging. Periodic serology studies (i.e., IgG4 levels) may be indicated with suspicion of systemic involvement. 13 Further, there is no standard for treating recurrence; re-treatment with high-dose corticosteroid is an option, alternatively, immunomodulating medications (i.e., rituximab) may be beneficial in refractory cases.13–15 In our case, there had been no recurrence of disease after 12 months of observation.
Conclusion
Only several cases of IgG4-RSD isolated to the paranasal sinuses have been described in the literature. The disease typically presents as a nasal lesion with obstructive symptoms. Imaging is nonspecific and demonstrates an expansive and erosive process, usually without infiltrative characteristics. Surgery at minimum provides tissue for histologic analysis but may provide relief of symptomatic nasal obstruction or may alleviate mucociliary obstruction and restore effective paranasal sinus ventilation when more extensive excisional procedures are performed. There is a paucity of evidence to guide management strategies. Local and systemic medical therapies are unproven and poorly studied; however, most reports describe symptom control and improved endoscopic appearance, with systemic steroid use. It is unclear whether IgG4-RSD lesions of the sinuses recur and, if so, when. Therefore, evidence-based recommendations for follow-up are lacking. It seems prudent that endoscopic surveillance continues yearly or as directed by symptomatology. Imaging may be best reserved for those with clinical evidence of recurrence.
Footnotes
Acknowledgments
We thank Aaron Prussin, M.D., and Mark R. Wick, M.D. for their support in the workup and management of the patient.
The authors have no conflicts of interest to declare pertaining to this article