
Abstract
Introduction
Septoplasty, or surgical correction of the deviated septum, is an elective, routinely performed rhinologic procedure to address nasal airway obstruction. In many cases, resected septal cartilage and bone fragments are sent for pathologic review, although there is no consensus on this practice. We reported two cases of incidentally diagnosed lymphoma after elective septoplasty and discussed clinical presentation, diagnosis, and management.
Methods
Retrospective chart review of two patients who underwent septoplasty at a tertiary academic medical center and found to have incidental lymphoma based on histopathology.
Results
Two patients who underwent septoplasty had an incidental diagnosis of lymphoma on pathologic analysis. One patient was noted to have an S-shaped septal deviation that produced bilateral nasal obstruction. She underwent a difficult septoplasty, in which the mucoperichondrial flap was firmly adherent to the underlying septum and bone. Final pathology demonstrated diffuse large B-cell lymphoma. She was treated with chemoradiation and remained free of disease at 59 months. The other patient had a history of nasal trauma, which produced left septal deviation. He underwent an uncomplicated septoplasty, with pathology that demonstrated low-grade B-cell lymphoma. Because there was no evidence of active disease, the decision was made to not treat and to observe the patient clinically.
Conclusions
This is the first reported series of septal lymphoma incidentally diagnosed on routine septoplasty. Although histopathologic review of specimens from routine nasal and sinus surgery is not routinely performed, this report highlighted the importance of this process, on a case-by-case basis, in detecting unexpected malignancies that otherwise were clinically silent.
Although there has been some interest in histopathologic detection of occult malignancies in sinonasal surgery, no previous reports identified incidental malignancies during septal surgery. In this study, we reported two cases of incidentally diagnosed lymphoma after elective septoplasty, both of which were clinically silent, and we discussed clinical presentation, diagnosis, management, and treatment outcomes.
Methods
This study was approved by the institutional review board of the University of California, Los Angeles. A comprehensive review of the institutional pathology data base at a tertiary academic medical center was conducted and identified, between January 1, 2001, and December 31, 2014, 329 septoplasty specimens that were sent for histopathologic review. During the same time period, a larger, indeterminate number of septoplasties were performed, although it was estimated to be 150–200 cases/y. The choice of submitting for histopathologic review was based on the primary surgeon's preference. We retrospectively reviewed the records of two patients who underwent elective septoplasty and who were both later found to have an incidental diagnosis of septal lymphoma. Analysis was limited to only septal contents (cartilage and bone) because mucosa was preserved during each procedure.
For both cases, endoscopic septoplasty was the technique used. A hemitransfixion incision is made, and an ipsilateral mucoperichondrial flap is elevated. After leaving an adequate caudal and dorsal strut, the quadrangular cartilage is transected and the contralateral mucoperichondrial flap is elevated. Deviated cartilage and bone is resected and sent for histopathologic analysis. Correction of deviation is confirmed via endonasal examination. Absorbable sutures are then used to loosely close the hemitransfixion incision, and a quilting stitch is occasionally used to reappose the bilateral mucoperichondrial flaps.
Results
The clinical history, presentation, management, and postoperative course of each patient are presented below.
Case 1
A 46-year-old female patient presented to the head and neck surgery clinic for bilateral nasal airway obstruction and congestion. She also reported occasional facial pressure and headache, which was worse on the left side. She had undergone computed tomography of the sinuses, which demonstrated an “S”-shaped nasal septum, without evidence of inflammatory sinus disease. Her medical and surgical histories were significant for Hashimoto thyroiditis for which she had undergone thyroidectomy 6 years earlier. She also had chronic microcytic hypochromic anemia for which no source of occult hemorrhage was found on workup (i.e., endoscopy). Preoperative laboratory studies demonstrated anemia (hemoglobin level, 10.5 g/dL) and a mildly elevated erythrocyte sedimentation rate (48 mm/hour) but were otherwise within normal limits. Physical examination confirmed the septal deviation, and the patient elected to undergo septoplasty. There were no septal mucosal abnormalities seen on nasal endoscopy. During the septoplasty, despite having had no previous nasal surgery or inflammatory disease and having normal-appearing mucosa, the submucosal tissue was extremely adherent to the underlying cartilage and bone, which made elevation of the bilateral mucoperichondrial flaps difficult. Nevertheless, the deviated cartilage and bone were successfully resected, and the patient tolerated the procedure well, without complications.
The final pathologic analysis of the septal specimen at 1 week after surgery showed a diffuse infiltrate of atypical, moderate-to-large lymphoid cells within the septal bone. Immunohistochemistry stains were positive for CD20, CD10, and BCL6 and negative for MUM-1 and BCL2. These findings were consistent with a diagnosis of diffuse large B-cell lymphoma (Fig. 1). The patient was referred to the hematology/oncology and radiation oncology services for further workup. She underwent a bone marrow biopsy; results were normocellular and did not demonstrate disseminated disease. A whole-body positron emission tomography–computed tomography confirmed the absence of distant metastases. Chromosomal analysis was normal (46, XX). These findings were consistent with stage IE disease, and the patient was subsequently treated with chemotherapy 1 month after surgery, followed by consolidative radiation therapy (3600 cGy). She tolerated the treatment well and had no clinical or radiographic evidence of recurrent disease at 59 months after surgery.
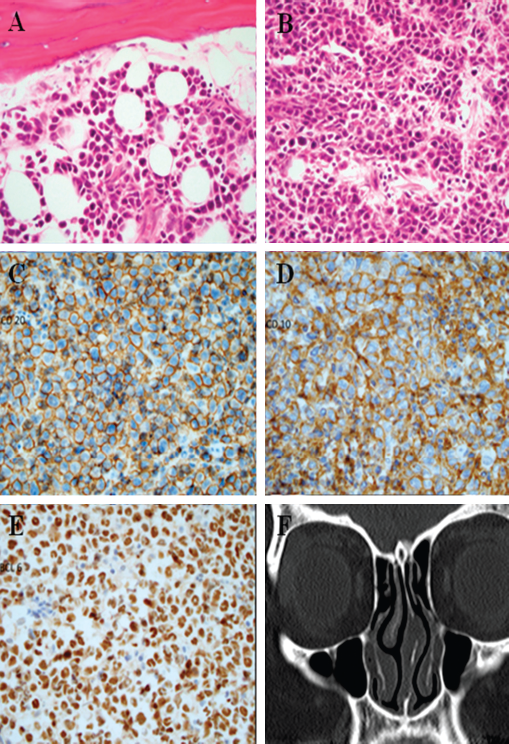
Septal contents from the patient in case 1, demonstrating a diffuse infiltrate of atypical moderate-to-large lymphocytes on hematoxylin and eosin staining (A, B), which further stained positive for CD20 (C), CD10 (D), and BCL6 (E), and confirmed the diagnosis of diffuse large B-cell lymphoma. (F) Computed tomography of sinuses demonstrates left septal deviation with no visible abnormalities seen on the scan. All images are 10 × magnification.
Case 2
A 60-year-old male patient presented to the rhinology clinic with severe left-sided nasal airway obstruction after sustaining nasal trauma years earlier. His medical and surgical histories were otherwise unremarkable. Nasal endoscopy demonstrated a severe left septal deviation with the septum touching the left inferior turbinate; the right nasal cavity contained no anatomic deviation. No mucosal abnormalities were seen. Preoperative laboratory study results were all within normal limits. The patient decided to proceed with elective septoplasty. The septoplasty procedure was unremarkable, and he tolerated the procedure well, without complications.
The final pathologic analysis of the septal bone at 1 week after surgery showed marrow elements, with a sparse, primarily interstitial, atypical lymphocytosis composed of small B cells that stain positive for CD20 and BCL2 and negative for CD5, CD10, BCL1, and CD23 (Fig. 2), which indicated a diagnosis of a low-grade B-cell lymphoproliferative disorder, likely follicular lymphoma. He was referred to the hematology/oncology service for further evaluation. A whole-body positron emission tomography–computed tomography did not identify any distant disease. Due to the patient's lack of symptoms and negative laboratory and radiologic workup, he will be monitored closely with regular visits to determine any changes.

Septal contents from the patient in case 2, demonstrating marrow elements with a sparse, primarily interstitial atypical lymphocytosis composed of small B cells on hematoxylin and eosin staining (A), which further stain positive for CD20 (B) and BCL2 (C), and negative for CD5, CD10, BCL1, and CD23, indicating a diagnosis of a low-grade B-cell lymphoproliferative disorder. All images are 10 × magnification.
Discussion
Septoplasty is the most commonly performed elective nasal procedure. Because the primary indication of the procedure is for the relief of anatomic nasal airway obstruction, many otolaryngologists generally do not send the extracted cartilage and bone fragments for histopathologic analysis. Furthermore, scarring between the tissue planes is not unusual, especially if patients have a history of nasal trauma or previous nasal surgery. Although there is ample evidence that the rate of occult malignancy in nasal and sinus surgery is low, an actual diagnosis of a malignancy is extremely clinically significant.
In light of the current health care socioeconomic climate, there has been a strong push toward the conscious practice of cost-effective, systems-based medicine. The role of routine histopathologic analysis of surgical specimens from elective procedures has been examined frequently across specialties. For instance, there is no consensus on this topic within the general surgery literature, in which some investigators support pathologic review of all specimens5,6; other investigators encourage only analyzing specimens if the macroscopic tissue appearance or clinical history is consistent with more concerning underlying conditions 7 ; whereas other investigators deem the incidence of malignancy to be so low that routine pathologic review is unnecessary or even “useless.”8,9 In addition to the study by Daniero et al., 4 Haffey et al. 10 further examined the clinical and financial value of routine review of septal surgical specimens. Of 516 septoplasties performed, 303 specimens were sent for pathologic analysis, with no unexpected diagnoses. 10
The investigators further found that pathology-related charges, valued at $255 per specimen, accounted for ~2% of the total charges per procedure, which accumulated to >$130,000 over the course of 2 years. 10 Although a considerable sum, the costs associated with treating aggressive non-Hodgkin lymphoma, such as diffuse large B-cell lymphoma, at an advanced stage (i.e., from late or missed presentation) are astronomical in comparison, estimated to be >$9000 per month at the palliation stage. 11 In addition, to a lesser extent, errors in diagnosis, such as missed diagnoses, are the second most common of rhinology-related litigation. 12 This, taken together with the improved outcomes with early intervention and the negative impact on quality of life with a late diagnosis, prompts a reexamination of the true value of histopathologic analysis in elective nasal surgery. Nevertheless, based on the literature and our own institution's experience, routine histopathologic review of all specimens in elective nasal surgery, indeed, is not cost effective and should be considered on a case-by-case basis.
Diffuse large B-cell (non-Hodgkin) lymphoma is the most common type of sinonasal lymphoma. 13 In the largest review of non-Hodgkin lymphoma of the sinonasal cavity, Abbondanzo and Wenig 14 found that low-grade lesions tend to present with nasal obstruction (the most common overall presentation), whereas high-grade lesions present with nonhealing ulcers, pain, facial swelling, epistaxis, or even cranial nerve palsies. 14 Furthermore, T-cell lymphomas were more likely to be midline (i.e., involving the nasal septum) and to behave aggressively, with significant local tissue destruction. 14 The fact that both cases were B-cell predominant malignancies may explain their relatively more indolent and clinically silent course. Although reported in previous series, in both cases, there were no classic harbingers of lymphoproliferative disorders, such as constitutional symptoms (fevers, chills, weight loss, night sweats) or generalized lymphadenopathy. 15 Also, given the localized nature of each case, it was unlikely for disease to be suspected based on laboratory or imaging studies. However, it is also conceivable that, despite the absence of classic signs and symptoms of lymphoproliferative disorders, the defining clinical manifestation of septal lymphomas is actually anatomic nasal obstruction due to septal deviation, and that this complaint may also prompt early consultation and lead to elective surgery, which possibly facilitates diagnosis.
A well-accepted canon of sinonasal surgery is that a unilateral nasal mass should carry a higher suspicion for neoplasm. Numerous studies have attempted to describe the incidence of occult tumors in routine nasal surgery, with nasal polyposis samples having been the most extensively studied. Yaman et al. 16 found that, although 85 patients with bilateral nasal polyposis had no neoplastic process diagnosed on histology, 6 of 32 patients (19%) with unilateral nasal “polyposis” were found to have neoplasms, which is similar to the results in the study by Arslan et al., 17 in which 7 of 54 patients with unilateral nasal “polyposis” were diagnosed with neoplasms, whereas none of the 197 patients with bilateral polyposis were diagnosed with neoplasms. However, larger series, such as those reported by Garavello and Gaini,18,19 indicate that the incidence of occult neoplasm is actually much less, on the order of <1%. Neither case in this series had any mass or mucosal lesion suspicious for malignancy, with the surgical indication for both cases being anatomic nasal obstruction, and the neoplastic process, in actuality, was embedded with the bony septal tissues.
The mainstay of treatment for sinonasal lymphoma is chemotherapy and/or radiation, with surgery only playing a diagnostic role. For patients with stage 1E disease (defined as involvement of one organ or extra-nodal area), there were reports that overall 5-year survival ranges from 67 to 75%.20–22 Left undiscovered and untreated, the natural progression of B-cell lymphomas of the sinonasal tract is aggressive local extension, with the potential for multiorgan involvement. Based on the findings of the International Non-Hodgkin Lymphoma Prognostic Factors Project, the International Prognostic Index was developed for the prognostication of non-Hodgkin lymphoma, including diffuse large B-cell lymphoma. 23 For the patient in case 1, she would have had an International Prognostic Index of 0 (low risk), and the standard of care for the treatment of limited stage diffuse large B-cell lymphoma is chemoradiation, 24 with observation that demonstrated decreased disease-free survival in one study. 25 For these reasons, the patient in case 1 underwent a more aggressive treatment regimen and did not elect for observation. However, the patient in case 2 had a low-grade B-cell lymphoproliferative disorder, likely a follicular lymphoma, which is associated with a more favorable diagnosis. In fact, limited-stage follicular lymphomas may actually be observed because many such patients do not require additional treatment.26,27
Based on the Lugano guidelines, 28 posttreatment surveillance for patients with low-grade sinonasal lymphoma involves regular clinical visits with their oncologists every 3 months for the first 2 years, followed by every 6 months for the subsequent 3 years, and annually thereafter. Patients should also be counseled on considering follow-up visits with their rhinologist at concurrent intervals to endoscopically evaluate the biopsy site for initial proper healing and local recurrence.
Conclusion
To our knowledge, this is the first reported series of septal lymphoma incidentally diagnosed on septoplasty. Although histopathologic review of surgical specimens from routine nasal and sinus surgery is not always performed (and oftentimes, not encouraged), this report highlighted the importance of this process in detecting unexpected malignancies that otherwise were clinically silent. At this point, given the rarity of such diagnoses in light of increased health care costs, there are no defining clinical or intraoperative characteristics that may prompt the surgeon to elect histopathologic review of septoplasty specimens that contain lymphoproliferative disorders but rather must be considered on a case-by-case basis.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article