
Abstract
Background
The issue of heat shock protein (HSP) 70 and anti-HSP70 antibodies in chronic rhinosinusitis (CRS) has never been explored.
Objective
To determine the nasal secretion (NS) levels of HSP70 and anti-HSP70 antibodies in patients with CRS with nasal polyps (CRSwNP) and patients with CRS without nasal polyps (CRSsNP), and to evaluate their associations with CRS clinical severity and correlation with NS interleukin (IL), IL-5 and interferon λ.
Methods
CRS severity was determined by Lund-Mackay scores. Levels of immunoglobulin E (IgE), IL-4, IL-5, interferon A, HSP70, and anti-HSP70 antibody levels in NS were measured by enzyme-linked immunosorbent assay.
Results
Forty-six patients with CRSsNP (25 women [543%] and 21 men [45.7%], mean [standard deviation {SD}]) age, 34.1 ± 123 years; 54 patients with CRSwNP (24 women [44.4%] and 30 men [55.6%], mean [SD] age, 37.9 ± 17.5 years). A group of 40 healthy subjects served as controls. Compared with the controls (with a mean [SD] NS HSP70 level of 0.05 ± 0.03 μg/mL), mean [SD]NS HSP70 levels in both the CRSsNP group (0.16 ± 0.07 ixg/mL) and CRSwNP group (0.21 ± 0.10 μg/mL) were increased (p < 0.001). Similarly, the mean (SD) NS anti-HSP70 antibody levels were significantly higher in patients with CRSwNP (0.25 ± 0.09 optical density value [ODV]) compared with CRSsNP (0.13 ± 0.04 ODV) (p < 0.001) and healthy controls (0.14 ± 0.02 ODV) (p < 0.001). NS HSP70 in subjects with CRSwNP showed a significant positive correlation with the Lund-Mackay score (r = 0.31; p < 0.05). NS levels of either HSP70 or anti-HSP70 antibodies were strongly correlated with NS IL-4 in the CRSwNP group (r = 0.62, p < 0.001; and r = 0.69, p < 0.001, respectively).
Conclusion
NS concentrations of HSP70 and secretory IgA anti HSP70 antibodies are increased in CRSwNP (but not in CRSsNP) and correlate positively with the Lund-Mackay score, NS IL-4, and NS IL-5.
CRS is characterized by increases in local production of several immunoglobulin isotypes, especially IgA and IgE. 12 The locally produced immunoglobulins from nasal polyp tissues of patients with CRSwNP include self-antigens, which indicate autoimmunity in its pathogenesis. 13 However, to our knowledge, the concentrations of HSP70 and anti-HSP70 antibodies in nasal secretions (NS) have not been evaluated in patients with CRS. In the present study, we determined the NS levels of HSP70 and anti-HSP70 antibodies in subjects with CRS and in healthy controls, evaluated their associations with CRS clinical severity, and their correlation with NS IL-4, IL-5, and interferon (IFN) λ.
Methods
Patients
Consecutive subjects with CRS were recruited during the period of 2011 to 2014 from the tertiary care allergy-immunology clinic and the otolaryngology clinic at the Chita Medical Academy (Chita, Russian Federation). All subjects met the criteria for CRS as defined by the American Academy of Otolaryngology—Head and Neck Surgery Chronic Rhinosinusitis Task Force. Patients with established acute respiratory tract infections, immunodeficiency, malignancy, pregnancy, Churg-Strauss syndrome, a diagnosis of aspirin intolerance, allergic fungal sinusitis, or cystic fibrosis as well as smokers or those taking anticoagulants or oral corticosteroids were excluded from the study. Aspirin provocation tests were carried out in all patients with CRSwNP and with a history of hypersensitivity reaction to aspirin and/or other nonsteroidal anti-inflammatory drugs by using oral, single-blind, placebo-controlled diagnostic challenge tests with aspirin according to European Academy of Allergy and Clinical Immunology/Global Allergy and Asthma European Network (EAACI/GA 2 LEN) guidelines. 14 All the subjects with a diagnosis of human immunodeficiency virus-acquired immunodeficiency syndrome and International Classification of Diseases, Ninth Revision codes for immunodeficiency diseases (range, 279.00–279.10) were excluded.
None of the patients enrolled in this study had a history of autoimmune disease as determined by a comprehensive review of patient electronic medical records. The subjects were not allowed to take intranasal steroids or systemic antibiotics during the 3 weeks before the study enrollment. Each patient underwent computerized tomography of the paranasal sinuses and diagnostic nasal endoscopy as part of routine clinical care; disease severity was determined by Lund-Mackay scores.
A skin-prick test was performed on all the subjects by using ALK-Abelló allergens (Hørsholm, Denmark) for Dermatophagoides pteronyssinus, Dermatophagoides farinae, dog, cat, mixed feather, alternaria, mixed molds, Aspergillus fumigatus, cockroach, mixed grass, mixed weed pollen, birch pollen, and ragweed pollen. Those with a positive skin-prick test result to molds and/or the presence of fungus in the sinuses were excluded. The patients with CRS were classified into two groups, depending on the presence of polyps: CRSsNP and CRSwNP. A group of age- and sex-matched healthy volunteers served as controls. The study was approved by the ethics committee at the Chita Medical Academy (Chita, Russia), and all the participants gave informed consent.
All the subjects who met inclusion and exclusion criteria underwent baseline assessments, which included assessment by the Russian version of a 22-item Sino-Nasal Outcome Test, blood sampling, and NS collection. Blood samples were obtained from each subject by using disposable vacuum blood collection tubes and then were centrifuged at 3000 rpm for 15 minutes. Supernatants were collected as serum samples. NS were sampled as previously described15–17 by the insertion into the anterior nares of sterile cotton-tipped wooden swabs, premoistened with sterile phosphate-buffered saline solution. The subjects were instructed to lean the head backward to reduce any contamination with tears from the nasolacrimal duct. The cotton swabs were removed after 20 minutes, placed in 2 mL of phosphate-buffered saline solution and vigorously shaken and wrung out. NS samples were stored at −70°C until IgE, cytokines, HSP70, and anti-HSP70 antibodies screening.
Immunoglobulins and Cytokines Assays
Serum and NS samples were analyzed for total IgE levels by using the immunometric assay of the Immulite 2000 system (DPC [Diagnostic Products Corporation]; Global Siemens Health Care, Erlangen, Germany). The levels of IL-4, IL-5, and IFN-λ in serum, and NS were determined by commercial enzyme-linked immunosorbent assay (ELISA) kits (Protein Contour, St. Petersburg, Russia) according to the manufacturer's instructions.
Measurement of HSP70 concentrations and anti-HSP70 antibodies in NS
HSP70 concentrations in NS were measured by the commercial Antihuman HSP70 ELISA kit (Assay-Designs-Stressgen, Ann Arbor, MI) according to the manufacturer's instructions. The sensitivity of the anti-human HSP70 ELISA was determined to be 6.79 ng/mL. The recombinant human HSP70 (StressGen, Victoria, British Columbia, Canada) was used in autoantibody-binding ELISA for detection of HSP70 antibodies in NS. Round-bottom microtiter wells (Dynatech Laboratories, Alexandria, VA) were coated with 4 mg/mL of recombinant human HSP70, 0.1 mL per well, for 2 hours at room temperature (22°C). Antigen solution was removed, and the wells were blocked with 1.0% human serum albumin in phosphate-buffered saline solution for 0.5 hours at 22°C or overnight at 4°C. After blocking, NS were diluted 1:10 and added to coated wells, incubated overnight at 4°C, followed by washing and development. Bound antibodies were detected by using goat antihuman IgA (α chain) peroxidase-conjugated antibodies (A7032; Sigma-Aldrich, St. Louis, MO) and rabbit antihuman secretory component peroxidase conjugated antibodies (P0166; Dako, Carpinteria, CA). The goat antihuman IgA determined the whole pool of IgA antibodies (IgA plus secretory IgA [sIgA]) in NS by detection of α chain. Secretory component peroxidase conjugated antibodies react with secretory component bound to sIgA. Peroxidase reactivity was visualized by using o-phenylenediamine (0.2 mM in 0.1 M citrate buffer pH 5.0) in the presence of hydrogen peroxide (3.5 mm). The reaction was terminated with 2 M sulfuric acid. After adding the stop solution, optical density values (ODV) reading was performed by 450 nm spectrophotometry.
Statistical Analyses
Results are presented as mean (standard deviation [SD]). Differences in cytokines, HSP70, and anti-HSP70 antibody levels in NS between the groups were determined by one-way analysis of variance. Correlations between the variables were analyzed by Pearson correlation and the Spearman rank test, respectively, depending on the distribution of the data. Statistical significance was defined as a two-sided p value of <0.05. All statistical analyses were performed by using the software Statistica 6 (StatSoft, Inc., Tulsa, OK).
Results
Clinical and Demographic Characteristics
The demographic, clinical, and laboratory characteristics of the patients and controls are presented in Table 1. The study included 46 patients with CRSsNP (25 women [54.3%] and 21 men [45.7%], mean [SD] age, 34.1 ± 12.3 years) and 54 patients with CRSwNP (24 women [44.4%] and 30 men [55.6%], mean [SD] age, 37.9 ± 17.5 years. A group of 40 healthy volunteers (19 women [47.5%] and 21 men [52.5%], mean [SD] age, 35.3 ± 14.1 years) served as controls. From the 61 consecutive subjects with CRSwNP, 11 (18.1%) had a history of intolerance to aspirin and/or other nonsteroidal anti-inflammatory drugs. Among these 11 subjects, oral, single-blind, placebo-controlled diagnostic challenge test with aspirin was positive in 7 (63.6%). These seven subjects were excluded from the study. The levels of NS IFN-λ, IL-4, IL-5, serum and NS total IgEs of the patients and healthy controls are also presented in Table 1.
Demographic and laboratory data of the study population *
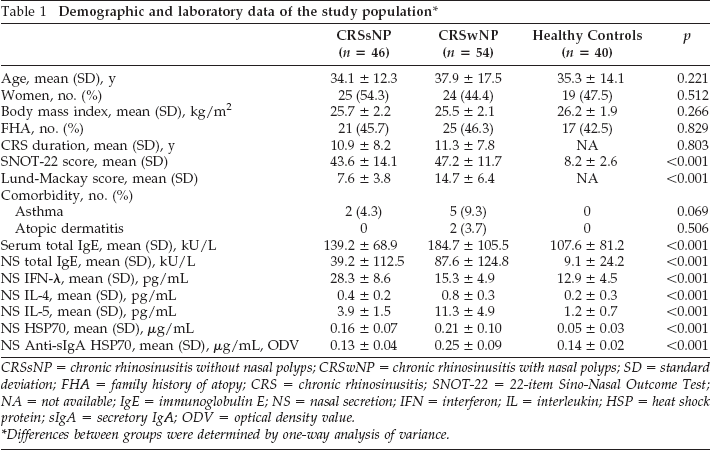
CRSsNP = chronic rhinosinusitis without nasal polyps; CRSwNP = chronic rhinosinusitis with nasal polyps; SD = standard deviation; FHA = family history of atopy; CRS = chronic rhinosinusitis; SNOT-22 = 22-item Sino-Nasal Outcome Test; NA = not available; IgE = immunoglobulin E; NS = nasal secretion; IFN = interferon; IL = interleukin; HSP = heat shock protein; sIgA = secretory IgA; ODV = optical density value.
Differences between groups were determined by one-way analysis of variance.
The Levels of HSP70 and anti-HSP70 Antibodies in NS
Differences in mean (SD) NS HSP70 levels between all CRS subgroups of controls are presented in Table 1. Compared with controls (0.05 ± 0.03 μg/mL), in both CRSsNP (0.16 ± 0.07 μg/mL) and CRSwNP groups (0.21 ± 0.10 μg/mL), mean (SD) NS HSP70 levels were increased (p < 0.001). The NS HSP70 levels were significantly higher in patients with CRSwNP compared with patients with CRSsNP (p < 0.01). Similarly, the mean (SD) NS anti-HSP70 antibody levels were significantly higher in patients with CRSwNP (0.25 ± 0.09 ODV), compared with CRSsNP (0.13 ± 0.04 ODV) (p < 0.001) and healthy controls (0.14 ± 0.02 ODV) (p < 0.001). There was no difference in NS anti-HSP70 antibody levels between patients with NS anti-HSP70 antibody levels and healthy controls. Further analysis showed that NS HSP70 and NS anti-HSP70 antibodies were strongly correlated (r = 0.71; p < .001) in the CRSwNP group, whereas no significant correlations between NS HSP70 and NS anti-HSP70 antibodies were detected in CRSsNP and control groups.
Correlation of NS HSP70 and NS anti-HSP70 Antibody Levels with CRS Clinical Characteristics
HSP70 levels in NS in the subjects with CRSwNP showed a significant positive correlation with the Lund-Mackay score (r = 0.31; p < 0.05). A similar correlation was observed between NS anti-HSP70 antibody levels and the Lund-Mackay score (r = 0.30; p < 0.05) in the CRSwNP group (Fig. 1). On the contrary, no significant correlations between these parameters were observed in the CRSsNP group. No statistically significant correlations were observed between the 22-item Sino-Nasal Outcome Test and the laboratory parameters in the study groups.

Correlation between nasal secretion (NS) heat shock protein (HSP) 70 and NS anti-HSP70 antibodies with NS interleukin (IL) 4 levels in patients with chronic rhinosinusitis with nasal polyps (CRSwNP).
Correlation of NS HSP70 and NS anti-HSP70 Antibodies with NS Cytokines
Results of the study showed that the NS levels of either HSP70 or anti-HSP70 antibodies were strongly correlated with NS IL-4 in the CRSwNP group (r = 0.62, p < 0.001; and r = 0.69, p < 0.001, respectively) (Fig. 2). A weaker positive correlation was observed between NS HSP70 and NS anti-HSP70 antibodies with NS IL-5 (r = 0.30, p < 0.05; and r = 0.36, p < 0.01, respectively) in the CRSwNP group (Fig. 3.).

Correlation between nasal secretion (NS) heat shock protein (HSP) 70 and NS anti-HSP70 antibodies with NS interleukin (IL) 5 levels in patients with chronic rhinosinusitis with nasal polyps (CRSwNP).

Correlation between nasal secretion (NS) heat shock protein (HSP) 70 and NS anti-HSP70 antibodies with the Lund-Mackay score in patients with chronic rhinosinusitis with nasal polyps (CRSwNP).
Discussion
In this study, we found that the NS concentrations of HSP70 and sIgA anti-HSP70 antibodies in CRS were increased, dependent of the Lund-Mackay score in the CRSwNP group (but not in the CRSsNP group). We also found that the NS concentrations of HSP70 and anti-HSP70 antibodies were positively correlated with IL-4 and IL-5 in the CRSwNP group. Because NS reflects the immunopathologic changes that occur during mucosal inflammation in CRS, the present study focused on HSP70 and anti-HSP70 antibody levels in it. In the current study, we demonstrated higher levels of HSP70 and sIgA anti-HSP70 antibodies in both phenotypes of CRS versus healthy controls. CRSwNP was characterized by a T-helper type 2 skewed profile, while CRSsNP was T-helper type 1 dominant. These findings were in agreement with the previous studies.18–21
Theoretically, HSP70 can play a wide range of immunologic effects in CRS. To better define HSP70 as both chaperone and cytokine, Asea22,23 named extracellular HSP70 as chaperokine. After contacting with exogenous HSP70, antigen-presenting cells release several proinflammatory cytokines, including tumor necrosis factor α, IL-1β, IL-6, and IL-12.24,25 Nevertheless, results of other studies showed that HSP70 may also play an anti-inflammatory role in several inflammatory diseases26,27 and this phenomenon was described by Chen et al. 26 as “heat shock paradox.”
In this study, we found significant differences in NS HSP70 levels between CRSsNP and CRSwNP phenotypes of CRS. One reason for this difference may be different cellular sources of HSP70 in CRSsNP and CRSwNP. 28 Although it has not yet been investigated in detail, it is very likely that HSP70 in NS could be a mixture of both constitutively expressed and stress inducible forms of HSP70. Besides nasal epithelial cells, there also are other cellular sources of HSP70 in sinonasal tissues. 29 Many bacterial and fungal homologs of HSP70 proteins were likewise identified in the oral and nasal cavity. 30
Because CRSwNP is a T-helper type 2 biased chronic mucosal eosinophilic inflammatory disorder, Lin et al. 31 investigated an expression and role of Bcl-2-associated athanogene-1 and HSP70 in eosinophilic and noneosinophilic CRSwNP, and found that Bcl-2-associated athanogene-1 and HSP70 were overexpressed in CRSwNP, especially in eosinophilic CRSwNP. Moreover, Bcl-2-associated athanogene-1 messenger RNA was augmented by IL-4, IL-17A, and IL-1β, but suppressed by IFN-γ. 31 In addition to acting as a chaperone during protein folding, HSP70 was found to play a role in inhibiting proinflammatory NF-κB signaling by acting as a bridge between an ubiquitin E3 ligase and the proteasome. 32 NF-κB induces transcription of genes, including IL-8, IL-16, inducible nitric oxide synthase, and eotaxins, which upregulation has implicated in the pathogenesis of CRSwNP. 33 Moreover, NF-κB acts as anti-apoptotic molecule in eosinophils and may be responsible for the recruitment and enhanced survival of these cells in CRSwNP. 34 Our observation that NS HSP70 was positively correlated with IL-4 and IL-5 in CRSwNP was in agreement with the study by Lin et al. 31 The possible mechanisms of interaction among HSP70, IL-4, and IL-5 in CRSwNP have to be elucidated in further studies.
Another interesting observation of our study was the finding of sIgA anti-HSP70 antibodies in NS of patients with CRS. Moreover, NS levels of anti HSP70 antibodies were positively correlated with the Lund-Mackay score in CRSwNP. Such anti-HSP70 antibodies have substantial roles in the pathogenesis and prognosis of other otolaryngologic35,36 and autoimmune diseases.37–40 The presence on sIgA anti-HSP70 antibodies could reflect the failure of immunologic mucosal tolerance toward HSP70 and subsequent development of mucosal autoimmune response.
Conclusion
Several limitations of our study warrant consideration. First, the outcomes of the study at this stage were very preliminary and had only an observational character; therefore, the exact contribution of HSP70 and anti-HSP70 antibodies to the pathophysiology of CRS needs further investigation. Second, we did not examine the molecular events that link HSP70 and anti-HSP70 antibodies to IL-4, IL-5, and IFN-λ. Third, it is unknown whether pharmacologic targeting of HSP70 and anti-HSP70 antibodies can modulate clinical features of the disease. Further studies are needed to better investigate pathophysiologic roles of these biomarkers in several phenotypes of CRS.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article