
Abstract
Background and Objective
The aim of this study was an evaluation of the dependence between the severity of atopic dermatitis evaluated with the Scoring Atopic Dermatitis (SCORAD) index and the occurrence of other atopic diseases and parameters.
Methods
The complete dermatological and allergological examinations were performed. The statistical evaluation of the dependence between the occurrence of bronchial asthma, rhinitis and duration of the skin lesions, and the severity of atopic dermatitis was performed.
Results and Conclusion
Two hundred and eighty-three patients were examined: 89 men and 194 women (average [standard deviation] age, 26.2 ± 9.5 years). The significant relationship was recorded between the severity of atopic dermatitis and bronchial asthma, the occurrence of rhinitis, and the duration of the skin lesions.
Currently, very little is known about the factors that may increase the risk of a child with AD developing asthma or allergic rhinitis, but the few studies done indicate that immunoglobulin E (IgE) sensitization may be the preceding event. 23 AD starts very early in infancy with chronic skin inflammation after a postnatal preclinical phase (phase 0) but without any evidence for IgE sensitization (phase I). This phase is followed by the emergence of sensitization, usually toward food allergen and other environmental factors that lead to the classic IgE-associated AD phenotype (phase II). The spreading and chronic inflammation of the skin and Staphylococcus aureus colonization play important roles. A substantial proportion of these patients seems to have a high risk of developing allergic rhinitis and asthma, which is further triggered by the chronic skin inflammation and scratching to become sensitized to self-proteins and which ultimately leads to a kind of autoimmune form of AD (phase III).24,25 Eosinophilic inflammation of the bronchial mucosa and bronchial hyperresponsiveness are key pathophysiologic elements in asthma. Patients with AD may have bronchial hyperresponsiveness, even without an actual asthma diagnosis, and it seems that bronchial hyperresponsiveness and mild asthmatic symptoms often remain undetected in patients with AD. The risk factors for the development of bronchial hyperresponsiveness and asthma are not fully characterized, but a positive family history for AD, young age at onset of AD, severe AD symptoms, and multiple sensitization to allergens increase the risk. 23 The aim of this study was the evaluation of the dependence between the severity of AD evaluated with the Scoring Atopic Dermatitis (SCORAD) index and the occurrence of bronchial asthma, the occurrence of allergic rhinitis, and the duration of the skin lesions.
Method
In the period 2008–2013, 283 patients with AD at the age of 14 years and older were examined. The diagnosis of AD was made by using the Hanifin-Rajka criteria. 26 Exclusion criteria were long-term therapy with cyclosporine or systemic corticoids, pregnancy, or breast-feeding. Patients with AD and who had other systemic diseases were excluded from the study as well. Complete dermatologic and allergologic examinations were performed. The following parameters were examined: bronchial asthma, allergic rhinitis, and duration of eczematous lesions. The statistical evaluation of the dependence between the occurrence of bronchial asthma, the occurrence of rhinitis, and the duration of eczematous lesions, and the severity of AD evaluated with SCORAD index was performed. This study was approved by ethics committee of Faculty Hospital Hradec Králové, Charles University of Prague, Czech Republic.
Severity of AD
The severity of AD was scored in agreement with the SCORAD index,27,28 with the assessment of topography items (affected skin area), intensity criteria, and subjective parameters. This examination was performed during 1 year, every 3 months, and the average SCORAD index was recorded.27,28 The diagnosis of bronchial asthma was made according to the results of spirometry at an allergologic outpatient department and according to the data about wheezing. Asthma was diagnosed as at least three separate episodes of wheezing, each at least 3 days in duration during the past year.
The evaluation of allergic rhinitis (seasonal or perennial) was made according to the anamnestic data, such as recurrent nasal symptoms and/or rhinitis (recurrent nasal discharge or blockage, with attacks of sneezing and itchy eyes), and according to the skin-prick test. The commercial food extracts Alyostal (Stallergens, Antony, France), with common inhalant allergens, such as grass, pollen, trees, dust, mites, animal dander, and bird feather, were used for skin prick test. Skin prick tests were placed on the volar side of the forearm according to the extent of AD and were carried out by a standardized method by using lancets with a 1-mm tip. The results were read after 15 minutes and were assessed by comparison with the wheal induced by histamine (10 mg/mL) and the negative control. A wheal with a diameter of >3 mm in comparison with a negative control was scored as positive. For the evaluation of the duration of AD, the AD lesions were evaluated as persistent or occasional, according to the dermatologic examination during one previous year and according to patient information.
Statistical Analysis
We evaluated whether there was some dependence between patients with AD at the age of 14 years or older, who had (1) bronchial asthma, (2) allergic rhinitis, or (3) persistent eczematous lesions, and the occurrence of a mild, moderate, or severe form of AD. The data were evaluated to determine whether the occurrence of bronchial asthma and rhinitis, and the duration of eczematous lesions were associated with the occurrence of a mild, moderate, or severe form of AD. Pairs of these categories were entered in the contingency tables, and the χ 2 test for independence of these categories was performed with the level of significance set to 5%.
Results
Patients and Tested Parameters
A total of 283 patients were examined: 89 men and 194 women, with the average (standard deviation [SD]) age, 26.2 ± 9.5 years) and with the average (SD) SCORAD of 32.9 ± 14.1. According to the SCORAD index, the mild form of AD was recorded in 89 patients (31%), the moderate form in 169 patients (60%), and severe form in 25 patients (9%). Bronchial asthma was recorded in 124 patients, allergic rhinitis in 210 patients, and persistent lesion in 175 patients. The survey of patients with the tested parameters is shown in Table 1.
The occurrence of monitored parameters in patients with AD

AD = atopic dermatitis; SD = standard deviation; SCORAD = Scoring Atopic Dermatitis.
Bronchial Asthma
Of 124 patients (44%) with bronchial asthma, the mild form of AD was recorded in 31 patients (11%), moderate form in 77 patients (27%), and severe form in 16 patients (6%). Of 159 patients without bronchial asthma (56%), the mild form of AD was recorded in 58 patients (20%), the moderate form in 92 patients (33%), and severe form in 9 patients (3%). The dependence was significant, at p = 0.026 (Table 2). The significantly rising occurrence of bronchial asthma in mild, moderate, and severe forms of AD is shown in Table 3.
Patients with BA and patients without BA, and the severity of AD according to the SCORAD index
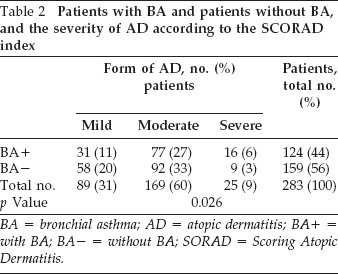
BA = bronchial asthma; AD = atopic dermatitis; BA+ = with BA; BA- = without BA; SORAD = Scoring Atopic Dermatitis.
Patients with BA and patients without BA calculated for mild, moderate, and severe forms of AD

BA = bronchial asthma; AD = atopic dermatitis; BA+ = with BA; BA- = without BA.
Allergic Rhinitis
Of 210 patients with allergic rhinitis, the mild form of AD was recorded in 58 patients (20%), moderate form in 128 patients (45%), and severe form in 24 patients (8.7%). Of 73 patients without allergic rhinitis (26%), the mild form of AD was recorded in 31 patients (11%), the moderate form in 41 patients (15%), and the severe form in 1 patient (0.3%). The dependence was significant, at p = 0.006 (Table 4). The significantly rising occurrence of allergic rhinitis in the mild, moderate, and severe forms of AD is shown in Table 5.
Patients with RC and patients without RC, and the severity of AD according to the SCORAD index

RC = allergic rhinitis; AD = atopic dermatitis; SCORAD = Scoring Atopic Dermatitis; RC+ = with RC; RC- = without RC.
Patients with RC and patients without RC calculated for mild, moderate, and severe forms of AD

RC = allergic rhinitis; AD = atopic dermatitis; RC+ = with RC; RC- = without RC.
Duration of Lesions
Of 175 patients with persistent lesions, the mild form of AD was recorded in 34 patients (12%), moderate form in 117 patients (42%), and severe form in 24 patients (8.7%). Of 108 patients (38%) with occasional lesions, the mild form of AD was recorded in 55 patients (19%), moderate form in 52 patients (18%), and severe form in 1 patient (0.3%). The dependence was significant, at p = 0.0000 (Table 6). The significantly rising occurrence of persistent lesions in mild, moderate, and severe forms of AD is shown in Table 7.
Patients with and patients without persistent lesions, and the severity of AD according to the SCORAD index

AD = atopic dermatitis; SCORAD = Scoring Atopic Dermatitis.
The occurrence of persistent lesions in mild, moderate, and severe forms of AD

AD = atopic dermatitis.
Discussion
There is a lack of reports that focus on long-term studies of the clinical evaluations observed during the course of AD with respect to its evolution and association with other allergic diseases in patients who are affected. Many studies demonstrate the prevalence of allergic diseases; however, most studies analyzed a limited period from infancy to later childhood and/or to early adolescence. Early childhood is thought to be a key period for the prevention of allergic march, and adolescence is another key period for the prevention of recurrence. Further prospective studies that use large cohorts are necessary to assess this issue. 29 Atopic march can occur at any age 30 ; there is recent evidence that atopic march does not always follow the classic sequence. 31 Environmental and genetic studies provide evidence that a defect in epithelial barrier integrity may contribute to the onset of AD and progression of atopic march. Studies in animal models demonstrate that epidermal barrier dysfunction can be caused by repeated sensitization to allergens to the skin, which leads to phenotypes of AD and systemic sensitization and increased risk of allergic rhinitis, lung inflammation, and airway hyperresponsiveness.32,33 Our study evaluated the relationship between the occurrence of bronchial asthma, the occurrence of allergic rhinitis, and the duration of the skin lesions, and the severity of AD evaluated with the SCORAD index. The significant relationship was confirmed between the occurrence of bronchial asthma, the occurrence of rhinitis, and the duration of the skin lesions, and the severity of AD.
We demonstrated atopic march in patients with AD because the occurrence of bronchial asthma, allergic rhinitis, and persistent eczematous lesions is significantly higher in moderate and severe forms of AD evaluated with the SCORAD index. The significantly rising occurrence of bronchial asthma in mild, moderate, and severe forms of AD was 35%, 45%, and 64%, respectively. The significantly rising occurrence of allergic rhinitis in mild, moderate, and severe forms of AD was 65%, 76%, and 96%, respectively. The significantly rising occurrence of persistent eczematous lesions in mild, moderate, and severe forms of AD was 38%, 69%, and 96%, respectively. According to our previous study, the occurrence of bronchial asthma, allergic rhinitis, and persistent eczematous lesions are recorded more often in adolescent and adults patients with AD who have food allergy to basic foods such as wheat, soy, peanuts, egg, and milk. 34 Patients with food hypersensitivity reactions, in general, significantly more often experience allergic rhinitis and persistent eczematous lesions; the dependence was confirmed in patients with hypersensitivity reactions to nuts, kiwi, fish, and apple. 35 Regarding the inhalant allergens, IgE sensitization to animal dander, dust, and mites may increase the risk of developing asthma or allergic rhinitis. Persistent lesions of AD occur more often in patients with sensitization to animal dander, mites, and dust. 36
In a prospective multicenter study, Ekbäck 37 followed up children with AD from infancy to the age of 10 years and focused on sensitization to allergens, severity of AD, and development of allergic airway symptoms at 4.5 and 10 years of age. According to the results, infant AD with high SCORAD index points was associated with an increased risk of asthma at 10 years of age. 34 According to Ricci et al., 38 AD is often the prelude to allergic diseases. This study included 176 children affected by AD and who were previously evaluated, between 1993 and 2002 at the age of 9–16 months, who underwent a telephone interview by means of a semistructured, preformed questionnaire after a mean follow-up of 8 years. According to the SCORAD index at the first evaluation, the children had mild AD in 23% of cases, moderate in 62%, and severe in 15%. AD disappeared in 92 cases (52%), asthma appeared in 30 (17%), and rhinoconjunctivitis in 48 (27%). The factors significantly related to the appearance of asthma were the following: sensitization to food allergens with specific IgE of >2 kU/L (cow's milk and hen's egg, p < 0.05), and to inhalant allergens with specific IgE of >0.35 kU/L (p < 0.05). The conclusion of this study 38 was that integrated management of AD does not seem to influence its natural course. Nevertheless, there was a decrease in the percentage of children that evolved toward respiratory allergic disease, which stresses the importance of early diagnosis and improvement management carried out by specialist centers.
The presence of allergic sensitization at 1 year of age might predict the development of respiratory allergy. 38 According to Hon et al., 39 many patients with AD would “march” to develop allergic rhinitis or asthma. The aim of the study was to evaluate the prevalence and severity of airway atopies in patients with AD. Allergic rhinitis and asthma severity were assessed in consecutive patients with AD seen at a pediatric dermatology clinic by using the allergic rhinitis score and the asthma control test. AD severity (SCORAD index and Nottingham Eczema Severity score) was recorded. A total of 110 patients with AD and 42 patients without AD were recruited. Allergic rhinitis and asthma were significantly more prevalent in patients with AD. When comparing mild with moderate-to-severe AD, there essentially was no difference between the prevalence of allergic rhinitis and asthma, or severity of symptoms by allergic rhinitis score and the asthma control test, but women reported more severe symptoms of sneezing and nose itching. The researchers conclude that allergic disorders of airways are common among patients with AD, independent of the AD severity. Most of the patients had mild-to-moderate allergic rhinitis and asthma. 39 The average (SD) age of patients in the study by Hon et al. 39 was 11.47 ± 4.67 years; however, in our study, the average (SD) age of patients was 26.2 ± 9.5 years.
In the study by Stelmach et al., 40 a global assessment of allergic diseases and pre- and postnatal exposure to various environmental risk factors was evaluated to enable early prevention of allergic diseases. This study was designed to evaluate an inner-city urban birth cohort to identify early environmental factors associated with AD and food allergy as well as the incidence of wheezing during the first year of life. 40 The risk factor profile of AD and/or food allergy in early childhood that was defined in this study support the following recommendations: (1) longer breast-feeding, (2) avoid pets during gestation, (3) avoid too frequent house cleaning, and (4) live in an area with decreased traffic density. 40 The study by Hong et al. 41 is an investigation of the effect of breast-feeding on current AD among Korean children. There was no significant association between breast-feeding and AD among children >5 years of age. Regardless of parental history of atopic diseases, breast-feeding for >12 months was a significant risk factor for AD. The effect of breast-feeding differed by age group. Prolonged breast-feeding increased the risk of AD in children who were <5 years of age, regardless of parental history of atopic diseases. 41
The study by Leonardi et al. 42 evaluated interleukin (IL) 17, IL-23, and IL-10 levels in children with AD and in healthy controls, in atopic and nonatopic subtypes, and their relationship with disease severity. A total of 181 children with atopic eczema-dermatitis syndrome and 93 healthy children were evaluated. Serum IL-17 and IL-23 levels were significantly higher, and serum IL-10 levels were significantly lower in children with atopic eczema-dermatitis syndrome than in the healthy group (p < 0.001). Moreover, serum IL-17 and IL-23 levels were significantly higher in patients with atopy than in nonatopic subtypes (p < 0.001). There was a correlation between the SCORAD index and both IL-17 and IL-23, and an inverse correlation between the SCORAD index and IL-10 in atopic and nonatopic types. This study confirmed the role of IL-17, IL-23, and IL-10, and their relationship with the severity of AD, which indicates their role as markers of “atopic march” and disease severity. 42
Conclusion
A significant relationship was confirmed between the occurrence of bronchial asthma, the occurrence of allergic rhinitis, the duration of the skin lesions, and the severity of AD evaluated with SCORAD index. The occurrence of bronchial asthma, allergic rhinitis, and persistent eczematous lesions was significantly higher in moderate and severe forms of AD evaluated by using the SCORAD index.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article