
Abstract
Background
Ragweed allergy represents a challenge for allergists due to its increase in some geographic areas, mainly northern Italy.
Objectives
To compare two allergy centers in northern Italy by analyzing both the pollen count and the patient characteristics (sensitization and allergy prevalence) over a 10-year period.
Methods
Pollen counts for 10 years (2004 –2013) were evaluated and compared in the two centers. Characteristics of patients who were sensitized and allergic to ragweed were analyzed.
Results
There was a significantly higher pollen count in Busto Arsizio than in Novi Ligure (p < 0.001). The patients who were seen in the Busto Arsizio center showed more frequent sensitization (p < 0.01) and allergy (p < 0.05) to ragweed than patients who were seen in the Novi Ligure center. The pollen count was significantly (p < 0.01) associated with sensitization and allergy difference. Allergic asthma was more frequent (p < 0.05) in Busto Arsizio.
Conclusions
The pattern of sensitization and allergy prevalence seemed to be associated with ragweed pollen pressure, such as quantity. The knowledge of the pollen count is relevant in clinical practice, mainly for the management of patients with allergy.
The prevalence of ragweed sensitization depends on the country: the mean sensitization prevalence in Europe is 14%, with wide variation from the top in Hungary (54%) to 3.5% in Italy. 3 However, also in Italy, there is a relevant difference among regions, with the peak in Lombardy, with 8–10% sensitization prevalence. 4 The presence of A. artemisiifolia in the northwest of the Milan province has been well known by botanists since 1940. 5 The first report of ragweed allergy in the Milan hinterland occurred in the Busto Arsizio district, located in the south of the province of Varese, at the end of the 1980s and in the Milan hinterland in 1990. 4 From then on, ragweed allergy prevalence has constantly increased both in Lombardy and in other northern Italy regions. At present, ragweed allergy is the second most common cause of pollinosis in Lombardy, after grass allergy. Other than causing severe symptoms in some patients, ragweed pollen is characterized by a peculiarity: it may also affect people >70 years old who never had any allergy until then. In this regard, it has been reported that the mean age at onset of ragweed allergy is 35 years: an age older than for other allergy types, e.g., mites, grasses. 6 Moreover, a further study presented evidence that the mean age at onset did not change after 5 years, even though the percentage of young people (<20 years old) was constantly increasing. 7 Thus, it is conceivable that the mean age at onset will be progressively diminishing as well as for other pollens over time. However, the onset in older people allowed to demonstrate an interesting issue: that AIT is effective also in aged subjects with ragweed allergy. 8 In these patients, there was an antigenic difference between A. artemisiifolia and Ambrosia trifida pollens. In fact, in the Lombardy area, only A. artemisiifolia (short ragweed) extracts are effective. 9
Also, in Piemonte, A. artemisiifolia is spreading because it is a highly infesting weed. The provinces with the highest ragweed pollen count are mainly Novara and Alessandria. 10 The percentage of patients sensitized to ragweed is also increasing, from 11% in 2000 to 16% in 2007. 10 From a clinical point of view, symptoms usually occur beginning in mid-August (the period with a concentration peak) to October.
Based on these considerations, this retrospective study aimed to (i) investigate the trend of the ragweed pollen count and the percentage of ragweed sensitized, and the patients with allergy in two allergy centers (Busto Arsizio in Lombardy and Novi Ligure in Piemonte) over a 10-year period; and (ii) compare the findings.
Methods
Places
Two allergy centers were considered: one placed in Busto Arsizio and the other one in Novi Ligure. The two cities are 124 km apart but are placed in geographically different areas. Busto Arsizio is a Lombardy city in the province of Varese (45°36′43.0′′N 8°51′06.48′′W) with an altitude of 226 m above sea level, and area of 30,66 km2). Its district is at the northern boundary of the Po valley, in the alluvial plain in the south of Varesine PreAlps. The ground is constituted of materials torn off the Alps during glaciation, e.g., pebble, gravel, sand, and clay, which is important because the rain is abundant and the ground has poor drainage. Novi Ligure is a Piemonte city in the province of Alessandria (44°45′33′′ N 8°47′08′ W) with an altitude 197 m above sea level; it is located in the “Basso Piemonte,” which is the southern area of Piemonte at the foot of the Ligurian Apennine. This geographic area is characterized by undulating hills. The climate is typically continental.
Patients
The data of two distinct groups of patients who were seen between 2004 and 2013 and tested for ragweed allergy were retrospectively evaluated. The patients were different because they were the ones who presented annually to their respective allergy clinics in Busto Arsizio and Novi Ligure for suspected allergic symptoms. Skin-prick testing was performed according to the European Academy of Allergy and Clinical Immunology position paper on prick test. 11 The allergen panel consisted of house-dust mites (Dermatophagoides farinae and Dermatophagoides pteronyssinus), cat, dog, grasses mix, Compositae mix, ragweed, Parietaria officinalis, birch, hazel, olive tree, Alternaria tenuis, Cladosporium, aspergilli mix (Stallergenes, Milan, Italy). The study procedure was performed according the rules approved by the internal ethical board of two institutions, Hospital of Busto Arsizio and Azienda Sanitaria Locale of Alessandria. Informed written consent was collected from each patient.
Sensitization to ragweed was defined by a positive skin-prick test with a wheal diameter of ≥3 mm. Monosensitization to ragweed was defined by a single sensitization to ragweed alone and the absence of allergic symptoms during ragweed pollen season. Polysensitization was defined by a positive skin-prick test to both ragweed and other tested allergens. Ragweed allergy was diagnosed on the concordance between a typical history of allergic seasonal symptoms and a positive skin-prick test result to ragweed. Monoallergy to ragweed was defined when patients sensitized to ragweed reported allergic symptoms only during ragweed pollen season. Polyallergy was defined by the presence of ragweed allergy plus another allergy. Allergic rhinitis (AR) and allergic asthma (AA) were diagnosed according to international guidelines.12,13
Pollen Counts
The pollen counts were recorded by a Hirst pollen trap (VPPS 2000; Lanzoni S.r.l., Bologna, Italy). The Hirst pollen trap was specifically designed for sampling pollen and fungus spores. Flow rate is fixed and provided by an external vacuum pump. The orifice of the spore trap (2–14 mm) was set at 0.5 mm from the trapping surface (sticky tape). The airflow was 10 L/min, and the speed of the trapping surface was 2 mm/hour. The apparatus always remained in the same place, 20 m above ground level and far from any pollution source, and it was permanently exposed to wind by means of a rotating air vane. The Hirst-type sample provides daily pollen trappings on sticky tape, which are transferred to microscope slides. Each slide is stained with fuchsin and is read by using an optical microscope at ×250 magnification.
The reading of the slide took place in a qualitative manner, which defined the individual particles, and quantitative, by reading five longitudinal bands by using a statistical method. Data are expressed as the average daily concentration from 0 to 24 hours (n/m3). The pollen count values, relative to the scanned surface, were extrapolated to the entire surface of the sampling. The pollen data were expressed as the mean of 10 consecutive years, from 2004 to 2013, considering the two allergy centers separately.
Data analysis was performed with the GraphPad software package (GraphPad Prism Software Inc, San Diego, CA). Data were expressed as absolute number, mean (standard deviation, and percentage. Statistical analysis of the results was performed by using the χ 2 test for inter- and intragroup analysis. We included in the analysis only subjects with a positive result to a skin-prick test for ragweed allergen because the aim of the present retrospective study was limited to assess sensitization and allergy to ragweed.
Results
Pollen Counts
The pollen counts in Busto Arsizio and Novi Ligure are shown in Fig. 1, the data are expressed as a mean during the 10-year period. Ragweed pollen quantity was significantly higher in Busto Arsizio than in Novi Ligure (p < 0.001). In fact, the annual mean pollen quantity was usually 3–8 times higher in Busto Arsizio than in Novi Ligure. The annual quantity in Busto Arsizio was variable, with wide variations within years, as reported in Fig. 2. On the contrary, the mean pollen count in Novi Ligure was more constant over time. However, there was no significant difference over time for both places.
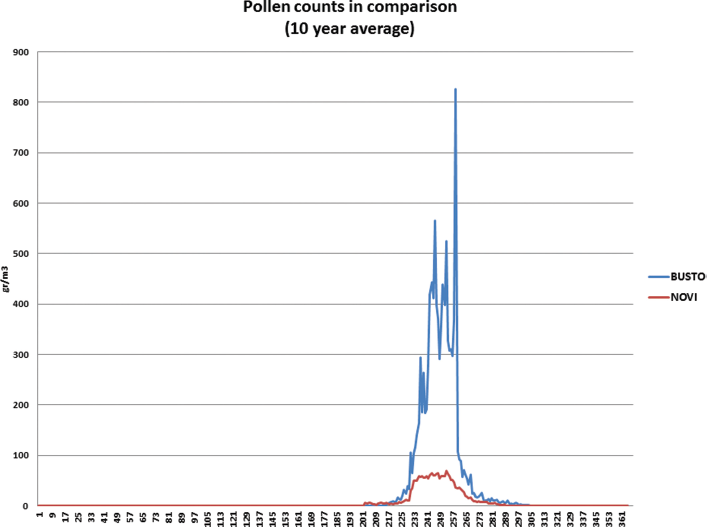
Ragweed pollen counts in Busto Arsizio and Novi Ligure: data are expressed as the mean of 10 years.

Ragweed pollen counts in Busto Arsizio and Novi Ligure: data are expressed as the annual mean of ragweed pollen count during each year.
Patients
The demographic characteristics of the patients who had a positive skin-prick test result to ragweed are shown in Table 1. There are no significant differences concerning both intra- and intergroup analyses. The distribution of the patients who were ragweed sensitized and those with allergy who were seen in both places between 2004 and 2013 are shown in Table 2.
Demographic characteristics of the patient population with ragweed sensitization

SD = standard deviation.
Clinical characteristics of patients with ragweed positivity to skin-prick test in the two centers

AR = allergic rhinitis; AA = allergic asthma
With regard to Novi Ligure, the percentage of patients who were ragweed sensitized is ~20% of globally tested patients, without significant variation over time. The percentage of patients who were monosensitized was ~10% of all the patients who were ragweed sensitized, without significant variation over time. Consequently, the percentage of the patients polysensitized was ~90% of all patients who were ragweed sensitized, without significant variation over time. The percentage of the patients with allergy to ragweed was ~40% of all the patients who were ragweed sensitized, without significant variation over time. The percentage of patients with monoallergy was ~15% of all the patients with ragweed allergy, without significant variation over time. Consequently, the percentage of patients with polyallergy was ~85% of all the patients with ragweed allergy, without significant variation over time.
With regard to Busto Arsizio, the percentage of the patients who were ragweed sensitized was ~50% of the globally tested patients, without significant variation over time. The percentage of patients who were monosensitized was ~10% of all the patients who were ragweed sensitized, without significant variation over time. Consequently, the percentage of patients who were polysensitized was ~90% of all the patients who were ragweed sensitized, without significant variation over time. The percentage of patients with allergy to ragweed was ~65% of all the patients who were ragweed sensitized, without significant variation over time. The percentage of patients with monoallergy was ~10% of all the patients with ragweed allergy, without significant variation over time. Consequently, the percentage of patents with polyallergy was ~90% of all the patients with ragweed allergy, without significant variation over time.
When considering the comparison between allergy centers, there were significant differences with the percentages of both patients who were sensitized and patients with allergy, whereas the distribution between mono- and polysensitization as well as between mono- and polyallergy was not significant. With regard to ragweed sensitization, the patients who were seen in Busto Arsizio were significantly (p < 0.01) more frequently (~2.5 times) sensitized to ragweed than were patients who were seen in Novi Ligure. With regard to ragweed allergy, the patients seen in the Busto Arsizio center were significantly (p < 0.05) more frequently (~1.5 times) allergic to ragweed than patients seen in the Novi Ligure center. Also, there was a significant association between ragweed pollen exposure and both ragweed sensitization (p < 0.01) and ragweed allergy (p < 0.01) when comparing the two centers.
With regard to AR and AA diagnoses, AR was more frequent than AA; AA was often associated with AR. AA was significantly (p < 0.05) more common in patients in the Busto Arsizio than in patients in Novi Ligure. There was no significant difference over time.
Discussion
Ragweed allergy represents a worldwide challenge for allergists 14 and seems to be increasing in some geographic areas, mainly in northern Italy. The present study aimed to compare two allergy centers in northern Italy by analyzing both the ragweed pollen count and patients' clinical characteristics, such as ragweed sensitization as well as ragweed allergy, over a 10-year period. First, ragweed pollen season is a typical seasonal pollination because the presence of ragweed pollens is limited to ~2 months in late summer in both areas. There is evidence that pollen concentration was significantly higher in Busto Arsizio than in Novi Ligure, by ~6 to 8 times. This outcome was constant over time. An annual variation in pollen count was evident in Busto Arsizio over time, even though not significant. These dips might depend on typical interannual climatic changes that affect pollen seasons; indeed, this finding was consistent with a previous study of a 30-year period that showed wide fluctuations over time related to climatic oscillations. 15
The frequency of patients sensitized to ragweed was significantly higher in the Busto Arsizio center than in the Novi Ligure center. This finding was associated with the different ragweed concentration in the two places. In the same way, the frequency of patients allergic to ragweed was significantly higher in the Busto Arsizio center than in the Novi Ligure center. Also, this outcome was associated with the different ragweed concentrations in the two places. Interestingly, AA was more frequent in the Busto Arsizio center than in the Novi Ligure center.
These facts could confirm the relevance of environmental factors, e.g., pollen quantity, which concerns the sensitization and allergy prevalence pattern. In other words, this study demonstrated that, the higher the pollen count, the higher the frequency of both sensitization and allergy. This finding was consistent with previous recent studies that had evidence of an association between pollen count quantity and an increase in sensitization and allergy.15–19 However, there are other conflicting studies that contradict our findings.20,21 Generally speaking, the concept regarding the link between allergen exposure and symptom occurrence is a cornerstone in allergy, thus it is intuitive to associate pollen exposure quantity with sensitization rate as well as symptom severity. 22
In this regard, the present study confirmed a large series of studies that showed a relationship between pollen exposure and sensitization and/or allergy pattern. However, conflicting findings might depend on the characteristics of the single allergen, the age of subjects, the climate, the pollution, and the lifestyle as recently reviewed. 23 In this regard, the model of mite allergy was enlightening, as recently underlined. 24 It is well known that the prevalence of a mite allergy is closely linked to mite exposure: there is evidence that there is a cumulative increase in the development of allergy, depending on increasing exposure, with a peak level >10 μg/g of Der p1 and Der f 1. 25 However, there are studies that showed a bell-shaped dose-response slope for mite exposure in comparison with sensitization.26,27 To explain this “protective” effect exerted by high exposure levels, it has been proposed as a tolerogenic effect, but related studies were inconsistent.
Thus, the question is still open, so further studies should be conducted to better define this aspect. The present outcomes are clinically relevant as it underlines the importance of potentially reducing allergen exposure quantity to prevent sensitization. The present study also highlighted the close association between ragweed pollen quantity and the rate of both sensitization and allergy. However, there is no association with both monosensitization and monoallergy. This fact seems to indicate that other immunologic factors may be involved in the polysensitization and polyallergy phenomena that transcend the allergen exposure. In addition, pollen counts substantially did not significantly change over time in the two areas as well as the sensitization and allergy prevalence over time.
However, this study has some relevant limitations. It was performed as a retrospective study, the patients were not reevaluated in a follow-up, there were no data about the diagnosis of rhinitis and asthma, there was a lack of pulmonary function, and data on other sensitization and clinical parameters were missing because we included in the analysis only the subjects with positive results to skin-prick test for ragweed allergen. For these reasons, further studies should be designed to address these issues. However, the main message of the present study is that the pattern of sensitization and allergy prevalence is associated with ragweed pollen pressure. This point reinforces the utility of locally assessing the pollen count because a relevant difference may exist between places even relatively close.
Conclusion
Ragweed allergy represents an important issue in northern Italy, with geographic differences. The knowledge of the pollen count is important in the clinical practice that mainly concerns the management of patients with allergy.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article