
Abstract
Background
Endoscopic extended maxillary mega-antrostomy (EMMA) is a mucosal sparing technique that allows maxillary drainage by gravity, with a reported symptomatic nasolacrimal duct injury incidence of 0–4%, based on history alone. Injury to the nasolacrimal duct is known to cause epiphora, a complication that is rare but more often seen in this revision surgery.
Objective
The goal of this study was to determine the incidence of nasolacrimal system penetration during EMMA. We, in addition, sought to determine the minimal safe distance from the midpoint of the maxillary line (the “M” point) to the nasolacrimal system to avoid this injury.
Methods
Six cadaveric heads underwent bilateral Jones II test followed by EMMA. Measurements from the M point to the antrostomy were recorded. The Jones II test was then repeated to assess for penetration and/or injury of the nasolacrimal system. If no penetration occurred at the surgical limit of EMMA, then dissection was continued incrementally until penetration occurred. This measurement was recorded.
Results
Lacrimal duct violation was identified in 5 of 12 procedures (42%). Lacrimal duct penetration occurred at an average of 3.7 mm (range, 2–7 mm) posterior to the M point.
Conclusion
Subclinical lacrimal system injury is likely to occur during EMMA. These findings would indicate that maintaining a distance of >7 mm from the maxillary line could avoid this injury.
With anterior dissection, intraoperative injury to the nasolacrimal duct (NLD) can occur, most commonly with back-biting nasal forceps. The nasolacrimal sac originates ~8 mm above the insertion of the middle turbinate and extends ~11 mm posteroinferiorly and becomes the NLD. 4 It is closest to the maxillary os at the midpoint of the maxillary line (the M point) (Fig. 1). Chastain et al. 5 describe the maxillary line as follows, “The maxillary line corresponded intranasally to the junction of the uncinate and maxilla and extranasally to the suture line between the lacrimal bone and maxilla within the lacrimal fossa. This suture was approximately half way between the anterior and posterior crests. Axially, the plane of the M point corresponded to the superior margin of the maxillary sinus ostium posteriorly (average, 10 mm) and was just inferior to the lacrimal sac-duct junction anteriorly.”
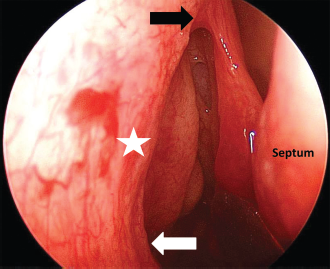
An endoscopic view of the right nasal cavity. The maxillary line extends from the axilla of the middle turbinate (black arrow) to the root of the inferior turbinate (white arrow). The M point (star) represents the midpoint along the maxillary line where the nasolacrimal system is closest to the dissection during endoscopic extended maxillary mega-antrostomy.
Published literature on EMMA reports a symptomatic NLD injury complication rate of 0–4%.1,5,6 However, all reports have been based on subjective symptomatic history alone. The true incidence of injury as determined by an in vivo visualization of the NLD has not been described. Because this is an aggressive technique that is more widely indicated than when first introduced, we sought to determine the true incidence of lacrimal duct injury. Our secondary goal was to determine the minimal distance from the M point to the lacrimal duct to provide the surgeon clinical guidance to promote effective, yet safe, maximal widening of the mega antrostomy.
Methods
An internal exempt institutional review board protocol was submitted and accepted for this study. Six cadaver heads were dissected, which resulted in 12 sides and procedures. A power analysis based on pilot data (mean [standard deviation] difference, 1.5 ± 0.8 mm, alpha 0.05, and power at 0.80) dictated a minimum sample size of five specimens in each arm. This was increased to six for the purposes of this study.
First, A type II Jones test was accomplished with cannulation of the inferior punctum and canaliculus, and flushing with fluorescein-stained saline solution. This ensured patency of the nasolacrimal system and ruled out anatomic abnormalities or previous injury. All the procedures were performed by the same senior resident (K. M. S.) and supervised by the senior author (E. K. W.). Maxillary antrostomy was performed as described by Wormald and McDonogh 7 and EMMA was then completed as described by Coleman and Duncavage. 1 Briefly, after the maxillary antrostomy was widened by removing the anterior and posterior lamella, a subtotal inferior turbinectomy was performed by using Foman scissors to incise between the anterior one-third and the posterior two-thirds, just behind the valve of Hasner. Another incision was made with the scissors at the plane of the posterior maxillary wall. A curved suction was used to fracture the turbinate into the nasal cavity. An osteotome was then used to take the medial wall down to the level of the nasal floor. At this point, the anterior-to-posterior diameter of the EMMA was measured at the level of the M point (Fig. 2). The Jones type II test was repeated by observing for leakage of fluorescein from the nasolacrimal system. If the nasolacrimal system was uninjured during EMMA, then the dissection was carried anteriorly with back-biting forceps, sequentially removing bone in 1-mm increments until the lacrimal system was disrupted, as evident by leakage during the Jones test. The distance from the point of penetration to the M point was measured.

An artist's rendition of the endoscopic view of the middle meatus after mega-antrostomy. The horizontal dotted red line with a surrounding box represents the distance that was measured from the M point to the anterior-most aspect of the antrostomy.
Statistical Analysis
Data were analyzed by using SPSS 19.0.0 (IBM Inc., Armonk, NY). All numerical data were considered continuous and normally distributed. Nominal data was categorized as yes or no.
Results
Lacrimal Duct Penetration Frequency
In the unoperated state, no case (0/12) showed evidence of anomalous routes of lacrimal drainage. After mega antrostomy was performed, lacrimal duct or inferior sac violation was identified in 5 of 12 sides (42%).
Mega-Antrostomy Measurements
Measurement of 12 mega-antrostomies determined a mean average anteroposterior distance of 29.8 mm (range, 23–37 mm) and a mean distance posterior to the maxillary line of 5.5 mm (range, 3–7 mm).
Lacrimal Penetration Measurement
In specimens with uninjured lacrimal apparatus, the maxillary ostium was expanded in an anterior dimension until lacrimal system penetration occurred. This was performed to determine the maximal amount of allowable dissection when approaching the maxillary line. Lacrimal system violation occurred at a mean distance of 3.7 mm (range, 2–7 mm) posterior to the M point along the maxillary line.
Lacrimal Penetration and Dissection
The unpaired Welch t test was performed to determine if the limit of anterior dissection was associated with lacrimal system penetration. When equal variances were not assumed, greater anterior dissection was significantly associated with lacrimal system penetration (6.3 mm in specimens without lacrimal penetration to 4.6 mm in specimens with penetration; p = 0.0249) (Fig. 3). However, the overall anteroposterior diameter was not significantly related to penetration (p = 0.511).

The mean distance between the anterior limit of dissection and the M point on the maxillary line during endoscopic extended maxillary mega-antrostomy. Column 1 represents the five sides where the nasolacrimal sac was violated (4.6 mm). Column 2 represents the seven sides where the nasolacrimal duct was not violated (6.14 mm). Error bars represent the standard deviation. This was found to be statistically significant, p = 0.029.
Discussion
Unfavorable outcomes with lacrimal duct penetration include epiphora and dacryocystitis. Previously, the region posterior to the anterior maxillary line has been described as a safe area to resect during medial maxillectomy, 2 which is especially important information when performing wide antrostomies, e.g., EMMA. Analysis of the data presented here indicated that the risk of penetration rises significantly in this “safe area.” Lacrimal penetration occurred at a mean distance of 3.7 mm posterior to the maxillary line at the M point but did not occur <6 mm posterior to the maxillary line. As a result, in our study, assuring at least 7 mm between the M point and the anterior limit of dissection avoided injury to the NLD.
Analysis of the data presented here indicated that the incidence of NLD penetration in this region due to endoscopic extended maxillary mega-antrostomy was likely higher than what has previously been reported in the literature clinically as “epiphora.” The present findings are consistent with the findings of Unlu et al., 8 who reported a 53.2% radiologic lacrimal bone dehiscence rate in their study of the NLD system after functional endoscopic sinus surgery. Taken together, analysis of these data indicated that subclinical injury to the lacrimal system may occur far more commonly than is clinically appreciated when performing EMMA.
There were several limitations to this study. With any cadaveric study, dehydration and tissue conformational changes may distort tissue. However, using a cadaveric model permitted critical study of the functional anatomic limits of this procedure in a way that would not be permissible in vivo. Because the study was not conducted in vivo, clinical correlation data are not available. This study demonstrated a high rate of injury to the lacrimal apparatus with EMMA but could not address the contribution of wound healing to the eventual function of the lacrimal system, which made a direct clinical correlation difficult.
Conclusion
NLD injury during extended maxillary mega-antrostomy occurred in 47% of procedures. The position of the NLD seems to vary from the M point of the anterior maxillary line. Maintaining a distance of at least 7 mm between the maxillary line and the anterior most extent of the dissection avoided any penetration into the nasolacrimal system in our experiment. Observing this distance may serve as a clinical marker to avoid NLD injury during EMMA. However, further studies on surgical patients are surely warranted.
Footnotes
P.D. O'Connor is a consultant for Cook Medical. The remaining authors have no conflicts of interest pertaining to this article
Acknowledgments
We thank our illustrator, Paul Woodham.