
Abstract
Background
Sinus computed tomography (CT) is performed for the diagnosis of paranasal sinus disease and to assess response to medical therapy. In addition, sinus CT is used for intraoperative imaging guidance. Multiple CTs increase cost and radiation exposure.
Objective
To determine potential cost savings and radiation dose reduction that result from the use of a single universal sinus CT protocol for diagnostic imaging and intraoperative navigation.
Materials and Methods
For sinus CT at the authors' institution, a single imaging protocol was begun and deemed acceptable by neuroradiologists and surgeons for diagnostic imaging and intraoperative guidance. The electronic medical record was queried over a 4-year period to determine the number of sinus CTs performed, dose-length products, referring providers' specialties, percentage of CTs used for intraoperative navigation, and the elapsed time between CT and surgery.
Results
A total of 6187 sinus CTs were performed by using a 64-detector scanner during the study period (2759 women and 3428 men; 53.6 ± 16.7 years [mean ± SD]), and 596 endoscopic sinus surgery cases used imaging guidance, for which all the CTs were deemed technically adequate. The mean dose-length product for the CTs was 338.4 ± 31.9 mGy-cm (mean ± SD). Of the 3702 sinus CTs ordered by nonotolaryngology providers, 167 surgeries with intraoperative navigation (4.5%) were performed. A higher percentage of CT referrals from sinus surgeons (23.9%) and other otolaryngology providers (11.4%) was used for imaging guidance (p < 0.0001). The time interval between sinus CT and surgery was greatest for nonotolaryngology providers (63.1 days, p < 0.01). Based on Medicare reimbursement, the total estimated saving was $147,628.
Conclusions
Adopting a single universal sinus CT protocol for diagnostic imaging and intraoperative navigation can be an effective means of decreasing cost and radiation exposure. However, successful implementation must take into account multiple practice-based considerations.
Public awareness has increased in recent years regarding the potential long-term cancer risks associated with iatrogenic radiation exposure from the rising use of CT. 9 For sinus CT, radiation dose reduction strategies have included adjusting scanner parameters,10–12 using bismuth eye lens shielding, 13 using iterative reconstruction techniques,14–16 and adopting cone-beam technology. 17 However, the most-effective way to decrease the radiation dose related to sinus CT is to eliminate unnecessary examinations.
The American Academy of Otolaryngology—Head and Neck Surgery recognizes the important role of computer-aided endoscopic sinus surgery (ESS) in delineating cases with complex anatomy. 18 One nuance in using surgical navigation systems is that they have specific technical requirements for CT to permit accurate image coregistration as well as to satisfactorily delineate bony anatomy. If an initial diagnostic CT was not performed with the appropriate parameters, then an additional CT would be necessary for intraoperative imaging guidance, which thereby leads to added expense and radiation exposure.
At our tertiary care multispecialty institution, >500 health care providers have access to ordering sinus CTs. Before 2010, two different sinus CT protocols were available, depending on whether the imaging was intended for diagnosis or for intraoperative imaging guidance for ESS. “Screening” sinus CT by using either a very low radiation dose or limited anatomic coverage was not in use because of local practice preferences. In an attempt to decrease sinus CT utilization, we synthesized and implemented a single sinus CT protocol that was universally acceptable for diagnostic imaging and intraoperative navigation, regardless of whether ESS was anticipated at the point of order entry. The objectives of this retrospective study included validating the universal sinus CT protocol, characterizing the reduction in sinus CTs that resulted, and estimating cost savings to the health care system.
Materials and Methods
This study was approved by the institutional review board (Mayo Clinic Institutional Review Board protocol 14–002262), and the need for informed consent was waived. Historically, sinus CT at our institution (a multispecialty academic medical center) was performed in the radiology department by using one of two imaging protocols, based on whether the CT was intended for diagnostic purposes or intraoperative navigation, neither of which would be considered a low-radiation dose “screening” sinus CT. In 2010, the two techniques were integrated such that all sinus CT began by using a single imaging protocol that was constructed and deemed mutually acceptable by neuroradiologists and sinus surgeons for both diagnostic imaging and intraoperative navigation (Fusion ENT Navigation System; Medtronic Inc, Minneapolis, MN). As such, all patients referred for sinus CT regardless of clinical indication were imaged under this universal protocol by using a 64-detector CT scanner (Lightspeed VCT or Discovery CT750HD; General Electric, Waukesha, WI), with the following imaging parameters: 120 kV, 180 mA, 0.5-second rotation time, 0.531 pitch, and 0.625-mm section collimation. An axial Fusion-compliant data set (standard reconstruction algorithm, 22-cm field of view, 0.625-mm slice thickness, no fiducial markers or headset required) was created and archived for all patients, regardless of whether or not ESS was planned at the time of imaging. Consequently, the subset of patients that ultimately needed ESS would not require repetitive imaging.
The electronic medical records for all outpatients undergoing sinus CT between October 1, 2010, and September 30, 2014, were queried. During this period, only the new universal sinus CT protocol was available for use regardless of the specialty of the ordering provider. The number of sinus CTs performed, the specialty of the referring provider, the percentage of CTs used for intraoperative navigation during ESS, the dose-length product reported for each sinus CT, and the amount of time that elapsed between CT and ESS were determined. In instances in which a patient had multiple sinus CTs, the date of the most recent CT before surgery was used. Patients with an age <18 years were specifically excluded. The referring providers were categorized into three groups: sinus surgeons, other members of the otolaryngology—head and neck surgery (ENT) department exclusive of sinus surgeons, and all other non-ENT health care providers. Referrals from trainees and physician assistants were attributed to the specialty of their supervising physician.
To provide an estimate of costs, the combined technical and professional fees for sinus CT (CT maxillofacial without dye; Level I Health Care Common Procedural Coding System—Current Procedural Terminology Code 70486) was obtained for 2010–2014 by using the Physician Fee Schedule search tool from the Centers for Medicare & Medicaid Services Web site (carrier locality, 310200). 19 The total cost was adjusted for inflation by using Consumer Price Index data to determine the present value for June 2015. 20
Statistical analysis was performed by using JMP 10.0.0 (SAS Institute Inc, Cary, NC). The χ 2 test was used to compare the proportion of patients in each group who underwent surgery after sinus CT. Differences in the mean time between sinus CT and ESS among the three groups were assessed by using oneway analysis of variance with the Dunn Multiple Comparison Test.
Results
A total of 6187 sinus CTs performed during the study period met inclusion criteria and had a mean dose-length product of 338.4 ± 31.9 mGy-cm (mean ± SD). The cohort consisted of 2759 women (44.6%) and 3428 men (55.4%), with an average age of 53.6 years ± 16.7 years (mean ± SD). During the study period, 876 ESS cases were performed, and 596 used imaging guidance (68.0%). Of all the patients who had a sinus CT, the proportion that ultimately underwent ESS with imaging guidance differed based on the specialty of the referring provider (p < 0.0001). As illustrated in Fig. 1, 23.9% of patients (278/1162) referred for sinus CT by sinus surgeons underwent ESS with imaging guidance, whereas this percentage was 11.4% (151/1323) for the remainder of the ENT department. Of the 3702 sinus CTs ordered by non-ENT providers, 167 ESS with imaging guidance (4.5%) were ultimately performed and did not require a new CT for intraoperative navigation because of the use of the universal CT protocol. The mean time interval between sinus CT and ESS was longer (p < 0.01) for non-ENT (63.1 ± 58.3 days [SD]) compared with sinus surgeons (42.5 ± 50.9 days [SD]) or the remaining ENT providers (45.1 ± 51.2 days [SD]). In all the cases used for intraoperative navigation, the sinus surgeons deemed the sinus CTs acquired with the universal protocol to be technically adequate.
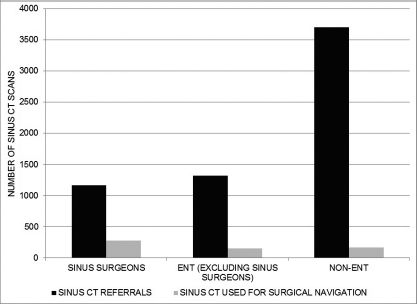
Bar graph, demonstrating the relative proportions of patients who underwent sinus CT compared with those who subsequently had ESS with imaging guidance based on referring provider specialty; the difference in proportions across the three referring groups was found to be statistically significant (p < 0.0001).
In chronological order, Medicare prices for the combined technical and professional fees for sinus CT from 2010 to 2014 were $247.48, $259.36, $246.27, $227.20, and $206.91. In applying these prices to the 596 ESS cases that did not require a repeated preoperative sinus CT because of the universal sinus CT protocol, total saving was estimated as $142,162, which translated to $147,628 when adjusted for inflation.
Discussion
The use of a universal sinus CT protocol for both intraoperative navigation and routine diagnostic imaging represents an easily overlooked opportunity for eliminating redundant imaging. This approach can reduce health care expenditures and patient radiation exposure. Although the estimated saving of $147,628 over 4 years in the current study was relatively modest, curtailing wasteful spending in any amount is increasingly necessary in the era of cost containment and accountable care. Likewise, the amount of radiation exposure avoided per patient was not substantial because a mean dose-length product of 338.4 mGy-cm only translates into an effective dose of ~0.8 mSv. 21 Although this effective dose in isolation is unlikely to cause harm to an individual, there is a constant obligation to keep medical radiation exposure as low as reasonably achievable out of concern for potentially deleterious cumulative effects. The annual average per capita effective radiation dose from medical procedures in the United States increased sixfold between 1980 and 2006, from 0.53 to 3.0 mSv compared with background environmental radiation exposure of 2.4 mSv. 22
In the current study, all the CTs used for ESS were graded as technically adequate, so subjective quality for intraoperative navigation was not negatively impacted. This was an expected result because the new universal sinus CT protocol did not lower the radiation dose. Adopting the strategy of making all diagnostic sinus CTs compatible with surgical imaging guidance systems requires the involved surgeons and radiologists to reach a consensus on acceptable image quality, and this is most challenging when decreasing the radiation dose. Whether using cone-beam CT or low-dose multidetector CT, a decreased radiation dose comes at the expense of declining image quality, and this diminished signal-to-noise ratio degrades the assessment of soft tissues more than bones. 23 From an interpretive standpoint, the minimum acceptable image quality is highly subjective, and this is reflected by tremendous variability in radiation dose for sinus CT. A survey of in-office, hospital-based, and outpatient imaging facility CT scanners found a 10-fold difference between the highest and lowest radiation dose for sinus CT, 24 and a separate report identified an 18-fold variation between minimum and maximum dose across 30 institutions when the sinus CT was being specifically performed for guidance during ESS. 25 Although some of this variability can be attributed to the use of different CT scanners, substantial variability can also be found across sites even when using the same CT scanner model. 26 When assuming that agreement can be reached on an acceptable subjective image quality for diagnosis and surgical navigation, a question can be raised as to whether or not a higher image quality is needed to preserve the fidelity of imaging guidance during ESS. Specifically, does a noisier image impair surface registration and thereby decrease navigation accuracy? Although the answer to this question may differ from one platform to the next, two studies assessed the impact of radiation dose reduction for ESS on the BrainLAB system (Feldkirchen, Germany) with phantom and cadaver testing.25,27 They found that the technical accuracy of surface registration was not dose dependent, and surgical landmarks could also be identified even at very low radiation doses. As such, their conclusion was that the primary limiting factor for radiation dose reduction is the surgeon's willingness to accept impaired image quality.
Certain logistical considerations may make it impractical to use a common protocol for diagnostic sinus CT and imaging-guided ESS. First of all, if a navigation system requires a stereotactic headset or fiducial markers to be worn during the CT acquisition, then it would not be cost effective to follow this procedure for a majority of CTs that will never be used for navigation. Second, the CT scanner(s) used must be able to meet the technical requirements set forth by the imaging guidance system, such as the minimum field of view and slice thickness. Third, the time that elapses between the sinus CT and ESS must be taken into account. Depending on the severity of disease and whether significant fluctuation is anticipated based on treatment (or lack thereof), it may still be necessary to repeat a preoperative CT for updated planning purposes. In the current study, the mean duration between CT and ESS ranged from 42.5 days to 63.1 days and, as expected, the longest time interval was for non-ENT providers. Any practice that considers the use of a universal sinus CT protocol would have to take this lag into account based on local referral patterns and wait times. Fourth, this approach would not be beneficial at a facility that is currently using very low radiation dose screening sinus CT for a majority of diagnostic examinations, with a higher radiation dose reserved for preoperative sinus CT. In this scenario, the potential cost savings from eliminating redundant CTs would come at the expense of increased radiation dose to a much broader group of patients.
The current study had multiple limitations. Because reimbursement records were not available to determine exact amounts billed and collected for each CT, Medicare rates were applied. As such, the reported saving represented a conservative estimate because the actual amount would have been higher if the higher reimbursement rates of private insurers were considered. However, given that there is significant variability in payer mix across practices, the use of Medicare rates allowed for a more generalizable result. The presented data were derived from an integrated multispecialty academic practice. Not only did this make it easier to reach a consensus on CT imaging protocols, but it also increased the likelihood that a patient who received a sinus CT and ultimately needed ESS would have this performed at the same institution. The benefit of a common sinus CT protocol would be negated if a patient proceeded with ESS at an external facility that may have required a repeated preoperative CT. Although worth acknowledging, these limitations did not significantly hamper the results. The primary objective was to highlight the potential for cost saving and to raise awareness of radiation dose reduction, with the understanding that the derived estimates were not absolute and would vary from one site to the next based on the unique nature of individual practices.
Conclusions
Adopting a single universal sinus CT protocol for diagnostic imaging and intraoperative navigation can be an effective means of decreasing cost and radiation exposure. However, successful implementation must take multiple considerations into account, including radiologist and surgeon preferences for image quality, technical requirements for imaging guidance systems, and other local practice differences.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article