
Abstract
Intracranial epidermoid cysts are rare. We report a case of a 55-year-old man who presented with trigeminal neuralgia and was found, on imaging, to have an epidermoid cyst located in the right middle fossa. He was managed via an entirely endoscopic endonasal approach. Postoperative magnetic resonance imaging confirmed complete removal of the mass, and the patient continued to have complete resolution of symptoms at a 1-year follow-up.
A previously healthy 55-year-old male patient presented to the emergency department after failed medical management of presumed trigeminal neuralgia. He had a 4–6–week history of intermittent, progressive right-sided headache and facial pain, which involved his right temple, jaw, and ear. Results of a physical examination were unremarkable. Noncontrast computed tomography showed a 4-cm, hypoattenuated, well-circumscribed mass in the right temporal lobe, with infiltration into the pterygopalatine fossa, posterolateral sphenoid sinus wall, and both foramen ovale and rotundum (Fig. 1). Magnetic resonance imaging (MRI) delineated a cystic mass with a central solid component, hypointense on T1- and hyperintense on T2-weighted images, with rim-like enhancement after contrast injection (Fig. 2).

(A) Preoperative coronal and (B) axial noncontrast computed tomographies, showing an expansile lesion in the right middle fossa.

Preoperative T2-weighted MRI of well-circumscribed mass in the right temporal lobe.
Because of the erosion of the lesion into the sphenoid sinus, endonasal endoscopic biopsy was recommended for diagnostic purposes. The lesion was approached via a transmaxillary-transpterygoid and transsphenoid approach, with the dissection staying anterior and inferior to the cavernous carotid artery and orbital apex. During the procedure, a large mass that infiltrated the pterygopalatine fossa as well as the floor of the sphenoid sinus was found, and incision of the capsule released an outflow of thick yellow debris, which was collected for pathology. The remaining debris was removed by using suction forceps and saline solution irrigation, with angled endoscopes that subsequently showed complete evacuation of the debris and the overlying dura of the temporal lobe. The thin capsule of the lesion was dissected circumferentially with a small cuff left in the far lateral recess of the resection cavity. The entire dissection remained extradural, and no cerebrospinal fluid leak was encountered during the procedure. Results of the final pathologic examination of the specimen and contents revealed squamous epithelium and abundant keratinous debris consistent with an epidermoid lesion. Postoperative MRI showed complete removal of the mass (Fig. 3). The patient was discharged 2 days later without complications. At 1 year, he continued to have complete resolution of headaches and trigeminal neuralgia.
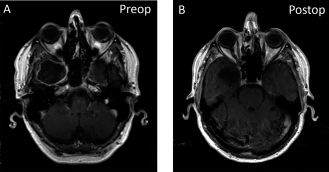
(A) Preoperative and (B) postoperative T1-weighted postcontrast MRIs, showing resection of the lesion.
Discussion
Epidermoid cysts are circumscribed lesions with irregular lobulated surfaces that can grow to encase vessels and nerves. Intracranial epidermoid cysts are commonly located in the cerebellopontine angle cistern (40–50%), the fourth ventricle (17%), the parasellar regions (10–15%), and, less commonly, in the cerebral hemispheres and brainstem. 1
On computed tomography, these lesions generally appear as well-defined hypodense masses. 1 On MRI, most epidermoid cysts are isointense to cerebrospinal fluid on both T1- and T2- weighted MRIs, although hyperintense epidermoid cysts on T1-weighted images have been reported secondary to high protein or lipid content. 2 Most cysts do not enhance after injection of contrast agents, although minimal rim enhancement can occur in ~25% of patients. 1 This enhancement is generally attributed to peritumoral granulation secondary to leakage of irritant cyst contents. 2
Our patient presented with the unusual feature of an epidermoid cyst located in the right middle fossa. The radiologic differential diagnosis for this location also included arachnoid cysts and schwannomas. Arachnoid cysts are also isointense to cerebrospinal fluid on T1- and T2-weighted MRIs; however, arachnoid cysts typically have complete suppression of signals on fluidattenuated inversion recovery imaging. 1 Schwannomas are expected to have intense enhancement on T1 with contrast. This was inconsistent with the minimal rim enhancement seen on imaging in this case.
Trigeminal neuralgia is a common symptom associated with epidermoid cysts. Many investigators have proposed possible mechanisms, including direct compressive effect of the mass, local irritation from cholesterol seeping through the cyst wall, or dense adhesions between the tumor and nerve. 5 We speculated that nerve compression by mass involvement of the foramen ovale and rotundum caused secondary trigeminal neuralgia in our patient. Surgical resection, traditionally by a transcranial approach, is typically necessary to relieve the neuralgia. 5 However, open transcranial approaches can be associated with parenchymal and neurovascular injury as well as postoperative epilepsy due to prolonged retraction of the brain. 6 Some surgeons have incorporated endoscopic-assisted open approaches, either to improve visualization of the resection cavity or to access the tumor for resection that may not otherwise be visualized microscopically.7,8 More recently, a number of case reports demonstrated successful resection of epidermoid cysts in the ventral skull base by a purely endoscopic endonasal approach.9–11
Our case report indicated that epidermoid cysts in the middle cranial fossa can be successfully resected by an endoscopic endonasal approach as well by providing direct surgical access to these lesions and minimizing the risks associated with brain manipulation. The limited postoperative follow-up period in this case is worth emphasizing because epidermoid lesions can often recur years after surgical resection.12–14 However, the comparatively noninvasive endoscopic approach may potentially offer similar postoperative outcomes with the added ability to address any recurrence with minimal morbidity.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article