
Abstract
Cerebrospinal fluid (CSF) leak is one of several complications that can occur after traumatic skull base injury. Although most patients present soon after the injury occurs, some can present years later, with resulting morbidity and the need for additional procedures. We present a case of a patient with a sphenoid sinus CSF leak who presented 12 years after a closed head injury that included a sphenoethmoid skull base fracture. We also reviewed the literature on this topic, with a discussion of previous reports of CSF leaks that occurred months, years, or decades after trauma. A late onset CSF leak appears to be a rare but important complication of traumatic skull base injury. This case highlights the need for clinicians to remain vigilant to the possibility of delayed CSF rhinorrhea, even years after traumatic head injury.
Case Report
A 61-year-old woman presented with a 14-month history of clear rhinorrhea and copious postnasal drip. Her history was significant for a traumatic motor vehicle accident 12 years earlier, with a resulting closed head injury and sphenoethmoid skull base fracture. This resulted in CSF rhinorrhea that was managed conservatively with bedrest and observation, and she was subsequently discharged after 5 days in the hospital. Four years later, she began experiencing severe headaches and vertigo, and a subsequent workup demonstrated a cerebral aneurysm that involved the hypophyseal artery immediately adjacent to her previous skull base fracture (Fig. 1). This was managed via endovascular treatment, with placement of a Neuroform stent (Stryker, Kalamazoo, MI) and coiling of the aneurysm.

Cerebral angiogram, showing a delayed posttraumatic aneurysm that involves the hypophyseal artery (arrow).
She was without symptoms or concerns until 7 years later when she developed intermittent postnasal drip and clear rhinorrhea. Shortly thereafter, she developed left otalgia and hearing loss that persisted for several weeks. Initial otologic and audiometric evaluation showed a middle ear effusion and a mild conductive hearing loss. The effusion did not resolve with conservative measures, and a myringotomy subsequently resulted in the drainage of clear fluid. A temporal bone computed tomography scan showed thinning of the tegmen on the left side (Fig. 2), and she subsequently was taken for a tympanomastoidectomy and exploration due to concern for a possible CSF leak. Several small defects were identified in the tegmen, but no active leak could be found. There were signs of chronic inflammation and infection of the mastoid, which were addressed, and the defects were repaired by using bone pate and temporalis fascia. After surgery, she continued to have clear rhinorrhea but was unable to collect a sufficient amount for β-2-transferrin testing. Imaging at this time showed the patient's previous aneurysm repair and fluid pooling in the sphenoid sinuses (Fig. 3). The patient was taken to the operating room for an elective surgical repair of a suspected CSF leak. Endoscopy revealed a left sphenoid sinus CSF leak, which was repaired with a pedicled nasoseptal flap (Fig. 4). The patient was discharged home on the second postoperative day, with resolution of her symptoms, and no recurrence was evident at her 1-year follow-up visit.
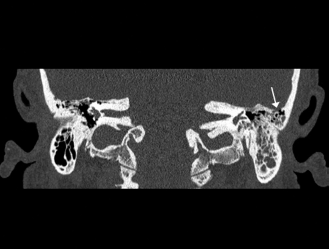
Temporal bone computed tomography scan, demonstrating opacification of the left mastoid cavity with thinning of the tegmen (arrow).

(A) Sinus computed tomography scan, showing airfluid levels in the left sphenoid and posterior ethmoid sinuses. (B) Coronal computed tomography scan, showing a possible dehiscent area that involves the left superolateral sphenoid sinus adjacent to previous endovascular aneurysm repair.

(A) Endoscopic view, showing fracture line along the left superolateral sphenoid wall (solid arrow) with a centrally located area of dehiscence (arrow). (B) The leak site was repaired by using a nasoseptal flap.
Discussion
CSF rhinorrhea is a common complication after traumatic head injuries and can result in meningitis and other intracranial complications if left untreated. Although traumatic CSF rhinorrhea often resolves with observation and conservative measures, leaks that persist beyond a few days are typically managed with surgical repair or placement of a lumbar drain. Management of traumatic CSF rhinorrhea is variable and remains somewhat controversial. Conservative management is commonly advocated because up to 85% of traumatic CSF leaks will close spontaneously. 2 However, some authors have encouraged immediate surgical repair to minimize the risk of infection and to provide reinforcement to the injury site. 3 Fortunately, with advances in endoscopic techniques, the reported success rates for traumatic CSF leaks are now quite high.4,5
Our patient presented with CSF rhinorrhea 12 years after a traumatic head injury. This patient had a small skull base fracture with CSF rhinorrhea that was initially managed conservatively. Unfortunately, she ultimately experienced delayed complications associated with this injury, including an intracranial aneurysm and a recurrent CSF leak. The incidence of traumatic CSF rhinorrhea that occurs years after injury is unknown but may be higher than is generally recognized. A previous retrospective review of 51 patients with traumatic CSF rhinorrhea reported that 16% of patients developed occult leaks and ultimately presented with meningitis an average of 6.5 years after trauma. 6 In many cases, persistent or recurrent CSF rhinorrhea is not recognized until the development of meningitis or other intracranial complications.6–8 CSF rhinorrhea due to previous skull base fracture has been reported to occur up to 48 years beyond the initial injury.1,9,10
The incidence of CSF rhinorrhea after traumatic head injury has been variably reported. In general, most leaks present immediately or shortly after the injury. A case series of 84 instances of CSF leak after head trauma that was published >60 years ago reported that only three patients presented more than 3 months after their injury. 11 More recently, a case series of 51 traumatic CSF leaks found that only 8 patients presented months to years after the initial injury, with the great majority occurring within several days. 6 Although the exact fraction of patients who present late after injury is not clear, these reports demonstrate that leaks can present many years after the trauma occurs.
The etiology for delayed leaks is unclear. Small dural defects may heal spontaneously, but persistent fracture lines or areas of weakness along the skull base can persist years beyond the injury, particularly because such fractures are rarely corrected surgically. Meningitis or localized inflammation often helps to seal small dural tears, but atrophy of the resulting scar and changes to surrounding bone can potentially occur over many years, thus weakening the site and increasing the risk for delayed leaks. For example, Leung et al. 12 reported a case of delayed CSF rhinorrhea in a patient 9 years after blunt head trauma. A small cribriform fracture at the time of injury was managed conservatively; however, the patient later developed clear rhinorrhea and seizures, and a repeated computed tomography scan showed a 1.5-cm defect at the fracture site, with an associated meningoencephalocele. Such enlarging fractures are rare, with previous estimates of incidence at between 0.05% and 1.6% 13 Some patients with previous skull base fractures may also be at increased risk for delayed CSF rhinorrhea due to predisposing factors, such as obesity or intracranial hypertension. This is highlighted by examples of delayed CSF rhinorrhea that have occurred after acute events that elevate intracranial pressure, including sneezing, coughing, and straining.14,15
Our case highlights the importance of long-term follow-up and counseling for patients with traumatic skull base fractures. Regardless of whether CSF rhinorrhea is a part of the patient's initial presentation, such injuries create the potential for delayed leaks, meningitis, and other complications that may occur many years after the initial injury. Although most traumatic CSF leaks resolve spontaneously, the risk of delayed complications indicates that some fractures and/or leak sites may need to be surgically repaired even if no active rhinorrhea is appreciated. Future studies that prospectively evaluate outcomes for patients with head trauma and skull base fractures may help to more clearly define indications for surgical repair.
Conclusion
CSF leaks that occur months or years after traumatic skull base injury may be more widespread than presently realized. As our case illustrated, accurate and timely diagnosis of this complication often presents significant challenges, with risks such as meningitis and other intracranial complications potentially becoming more frequent over time. Patients with even a distant history of traumatic skull base injury who present with symptoms consistent with a CSF leak should be thoroughly evaluated for this complication.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article