
Abstract
The aim of this study is to identify the demographics and epistaxis burden of hereditary hemorrhagic telangiectasia (HHT). A questionnaire was sent to participants with HHT who were recruited from a prospectively maintained respiratory clinic data base in a tertiary hospital. Details on demographics, HHT symptoms, family history, epistaxis severity, and treatment received were recorded. There were 34 of 60 responses (57%). Two responses were from families of the deceased. Of the 32 evaluable patients (men, 14; women 18), the average age was 51 years (range, 23–78 years). The average age of HHT diagnosis was 31 years (range, 3–61 years). The diagnosis of HHT was made by the respiratory team in 13 patients; neurologist (2); ear, nose, and throat (ENT) specialist (4); general practitioner (5); hematologist (4); gastroenterologist (1); and not mentioned in two patients. Twenty-seven of 32 patients (84%) had a positive family history of HHT. Only 13 patients had formal genetic testing (4 endoglin, 1 activin receptor–like kinase, 8 unknown gene). All patients who presented to the respiratory clinic had a background of epistaxis, which was noted on presentation. The average age at initial epistaxis was 14 years (range, 2–50 years). The frequency of epistaxis was daily 63% (n = 20), weekly 9% (3), monthly 16% (5), and a few times a year 10% (3), and unstated in one patient. Nine of 32 patients (28%) required a transfusion. Six patients thought that they were unable to perform daily activities due to epistaxis. Only 15 of 32 patients (47%) were under the care of an ENT specialist. The treatment plan for epistaxis management was deemed good by 7 patients, adequate in 8, poor in 6, and not stated by 11 patients. In conclusion, this survey is the first to quantify the epistaxis burden within the northeast of England. The management of epistaxis needs specific education and treatment to optimize the quality of life among these patients.
The clinical diagnosis of HHT rests on the Curaçao criteria 4 ; spontaneous recurrent nosebleeds, mucocutaneous telangiectasia (multiple at characteristic sites: fingertip pulps, lips, oral mucosa, or tongue), visceral involvement (gastrointestinal, pulmonary, hepatic, cerebral, or spinal arteriovenous malformations [AVM]), and family history (a first-degree relative affected according to these criteria). Three of four criteria are required for a definite clinical diagnosis of HHT, two criteria for “possible” HHT, and 0 or 1 criterion makes the diagnosis unlikely. Advances in molecular biology have revealed multiple genes linked to HHT. To date, five HHT genetic subtypes are recognized: three linked to particular genes and the remaining two are associated with a particular locus. The causative genes are endoglin (ENG), ALK1, and SMAD-related protein 4. 5 The former two account for 80% of cases, whereas the rarer SMAD-related protein 4 causes juvenile colonic polyps in addition to HHT. 6
Certain populations have a predominance of one mutation over another. For example, Spanish and other Mediterranean countries (France, Italy) have more ALK1 mutations in contrast to northern Europe or North America, which have ENG. 7 It is unclear whether this reflects the referral practice of HHT centers or genuine geographic variation. The genotypephenotype relationship has been explored extensively, with results of some reports that indicate that ENG mutations are more frequently associated with lung AVMS, 8 whereas ALK1 mutations with liver problems.9,10 Although HHT is highly penetrant, the nature and severity of HHT vary among individuals, even within the same family. This may partly be related to the hundreds of mutations associated with each HHT gene and as yet unidentified genetic modifiers.
From an otolaryngology point of view, patients with HHT typically present with recurrent epistaxis of varying severity and frequency,11,12 which can be challenging to manage both in the primary and secondary care setting. Of significant concern is the diagnostic delay in HHT, which leads to increased morbidity and mortality, and poor quality of life, not to mention a psychosocial impact both on the individual and his or her family.13,14 This is mainly due to poor knowledge among health care professionals, inadequate disease awareness among patients, and a lack of promptly available diagnostic tools.
There have been several studies that evaluated the epidemiologic and clinical manifestations of HHT nationally and internationally. To date, there has been only one U.K. study that evaluated the epistaxis burden among the national community. 15 The purpose of this study, which is the first of its kind, is to survey the demographic makeup of the HHT population of the northeast of England as well as to quantify epistaxis burden within the local community.
Methods
Patients with HHT were recruited from a prospectively maintained respiratory clinic data base at Freeman Hospital, Newcastle upon Tyne (tertiary center). This tertiary clinic caters to the entire northeast population, which totals 2.5 million residents (2011 census). Sixty patients with three or four Curaçao criteria were included. Ethics exemption was granted by the NRES Committee North East — Newcastle and North Tyneside 2. A questionnaire (1) recording details on demographics, HHT symptoms, family history, epistaxis severity, and treatment received was posted to patients in 2013. Responses (postal and online) were transcribed into an Excel spreadsheet by the study team. A postal reminder was sent after the initial request to improve the response rate. Fig. 1, Fig. 2 and Fig. 3, Table 1, Table 2.

Epistaxis frequency over the past 2 years.
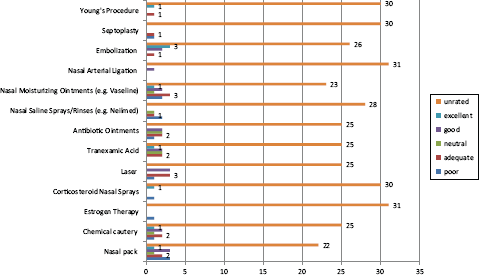
Efficacy of various epistaxis treatment strategies.

Rating of resources and the impact of HHT on the individual and his or her family.
HHT demographics

n/a = not applicable.
Epistaxis details

A&E = accident and emergency department; GP = general practitioner; ENT = ear, nose, and throat specialist; n/a = not applicable.
Results
Demographics
There were 34 of 60 responses (57%). Two responses were from families of the deceased. Of the 32 patients who were evaluable (14 males, 18 females), the average age was 51 years (range, 23–78 years). The average age on HHT diagnosis was 31 years (range, 3–61 years). Twenty-seven of 32 patients (84%) had a positive family history of HHT. Thirteen of 32 patients (41%) had formal genetic testing (4 ENG, 1 ALK, 8 did not remember the type of genetic mutation). In terms of initial clinical presentation, 23 of 32 (72%) had epistaxis, 18 of 32 (56%) had skin telangiectasia, and 8 of 32 (25%) had chest symptoms.
Epistaxis
Twenty-three of 32 patients (72%) reported epistaxis. The average age at initial epistaxis was 14 years (range, 2–50 years). The diagnosis of HHT was made by the respiratory team in 13 patients, the neurologist (2), ENT specialist (4), general practitioner (5), hematologist (4), and gastroenterologist (1), and not mentioned in two patients.
A range of medical and surgical treatments had been used with varying degrees of success. Only 16 of 32 were seeing (or had seen) an ENT specialist. Nine of 32 patients (28%) had transfusion within the previous 2 years. Nasal packs had been used for 10 individuals, chemical cautery (8), estrogen cream (2), corticosteroid nasal spray (2), transexamic acid (6), antibiotic ointment (7), nasal saline solution rinse (4), or Vaseline (9). Of the more-invasive treatments, laser was used in 7 individuals, arterial ligation (2), embolization (6), septoplasty (2), and the Young procedure (2). There was a great deal of variability in the efficacy of the treatments. Of the limited numbers who underwent invasive treatments (nasal artery ligation, embolization, and the Young procedure), beneficial effects were reported.
Discussion
The management of HHT is certainly challenging and demands a multidisciplinary approach. There is often no dedicated ENT specialist, clinic, or epistaxis treatment plan for these individuals. Due to the disparate treatment approaches, these individuals (particularly the refractory cases) and their families are often left frustrated, and the emotional and psychosocial impact cannot be understated. There have been limited studies that evaluated the epistaxis burden among the U.K. HHT community. This background provided the impetus for undertaking a survey among the northeast HHT population, which to our knowledge is the first to assess the local demographics and epistaxis severity.
One of the key findings, which is not unique just to our study, is the diagnostic delay between initial epistaxis presentation and HHT diagnosis. This is not surprising because most of the HHT symptoms, including recurrent epistaxis and telangiectasia, become more prevalent with age and are most present by 50 years of age. This lapse presents a significant opportunity to intervene and reduce both the morbidity and mortality associated with HHT, diagnose other family members, and provide genetic counseling to those planning to have children. Given that the current genetic testing methods can identify at least 80% of individuals with HHT, this would be useful in diagnosing younger adults and children, many of whom are asymptomatic or have only mild symptoms but who are at risk of recurrent hemorrhage and AVM complications.
This study was unable to make any correlation between the genotype and phenotype because only a third of the patients underwent genetic testing. It has been recognized that distinct phenotypic differences arise with ENG mutations (HHT1) and ALK1 mutations (HHT2). In the study by Guttmacher et al., 16 the subjects with HHT1 have significantly earlier onset of epistaxis and telangiectasis. In our study, there was a significant variation in epistaxis burden in terms of frequency and severity (the need to visit the accident and emergency department, the need for blood transfusion, and the ability to carry out the daily activity). The frequency of epistaxis was daily 63% (n = 20), weekly 9% (3), monthly 16% (5), and a few times a year 10% (3), and unstated in one patient. This mirrors other recent studies. 15 In our survey, 9 of 32 patients (28%) required a transfusion. Six patients thought that they were unable to perform daily activities due to epistaxis.
This survey demonstrated that only 15 of 32 patients with HHT and with epistaxis (47%) were seeing an ENT specialist, not necessarily at the Freeman Hospital, which has implications on the quality of treatment. These patients are frequently self-treating, attending the primary care providers or the accident and emergency providers. With only 7 of 32 patients rated their epistaxis treatment plan as good, this trend is particularly disappointing and needs remedial action. The efficacy of various epistaxis treatment strategies is a crucial point in the quality of life of patients with HHT. A surprising finding from this survey is that the epistaxis treatment strategy was disparate across the various ENT departments in the northeast. Many epistaxis treatments remained untried (hence not rated), whereas those treatments that were attempted (both surgical and medical) were limited to a very few patients (n = 3), with varying efficacy. Hence, there is a need to coordinate the epistaxis management strategy among ENT departments.
What is particularly striking is the patients' perceived lack of resources and information on epistaxis, with only 9 of 32 rating them as good. Only 7 of 32 understood the medical consequences of epistaxis. Only 6 of 32 understood the emotional and/or psychological impact that epistaxis episodes were having on their family. Part of this may be related to the fact the repeated epistaxis episodes are associated with the impairment of psychosocial quality of life, together with relationship modifications. 14 Indeed, these patients felt different and often experienced a desire to withdraw compared with others.
Comments on Methodology
The strengths of this survey are that, by setting out a minimum data set a priori, we were able to ensure that key demographic data, epistaxis severity, and treatment options were captured. In addition, the impact of HHT on the individual's quality of life as well as his or her family was also evaluated. There are a number of validated tools to measure HHT impact, both generic and disease specific. Until recently, various HHT units used their particular systems for grading epistaxis severity, which may be due to comfort with their own systems. In 2010, a standardized, validated epistaxis severity score was introduced. 17 The score was weighted on six factors, including frequency, duration, intensity, need for medical attention, anemia, and need for transfusion. At the outset, we thought that using multiple validated questionnaires to capture the various domains may compromise patient response rate. Therefore, a decision was made to devise our own single questionnaire (see Appendix A1), which would be easily administered, understood, and completed, thus improving compliance.
It is important to acknowledge the limitations of this study. One of the key issues is the low sample size, moderate response rate, selection, and recall bias. The low sample size is a reflection that this HHT sample is from a respiratory data base of patients who also had pulmonary AVM. At present, we are limited to using this data base because there is not an HHT data base in the primary or secondary care setting. Regardless of the data base, the true prevalence of HHT in the community may not be represented accurately because some patients with milder phenotypes may not present to health care services. The respiratory HHT data base also covers a large geographic area where our ENT department is not the sole service, thereby resulting in differences in epistaxis management. Given the hereditary nature of HHT as well its highly penetrant nature, one method to obtain a more representative larger sample would be to include other members of the family affected by HHT who may not necessarily be in the respiratory data base. Other data bases can be used, but these also have limitations. The “Health Improvement Network,” a longitudinal, computerized general practice data base is one such example, but it only covers 5% of the U.K. population. By using this data base, it was shown that HHT was underdiagnosed in the United Kingdom, particularly in men (which reflects their lower consultation rates with primary care services) and lower socioeconomic groups. There was also a marked variation in the prevalence of HHT among different geographic regions across the United Kingdom, being highest in the southwest and lowest in the west Midlands. 18 Surveying the HHT Foundation International contacts would also yield a larger morerepresentative sample.
The moderate response rate is also another limitation. We attempted to improve the response rate through reminders as well as integrating an online response. Despite our best efforts, only a 57% response rate was achieved. The lower response rate could be a reflection of the burdens and limitations of everyday life experienced by the patient affected with HHT. On the opposite end of the spectrum, those with milder epistaxis symptoms may be less inclined to respond.
Comparison with other Studies
The average HHT diagnosis age in our survey was 31 years (range, 3–61 years), which is comparable with other European studies. In a recent Italian study (n = 233), the age of first referral and the age of first definite diagnosis of HHT were 29.2 years and 40.1 years, respectively. 19 The average age at initial epistaxis was 14 years (range, 2–50 years). Similarly, in a Norwegian study (n = 98, 77% of the patients' epistaxis commenced by or before the age of 20 years. 20
Clinical Applicability of the Study
This survey highlights the epistaxis burden within the HHT community of the northeast of England as well as lack of support. Clearly, changes in practice require consideration. There needs to be improved awareness of the possibility of HHT in those presenting with recurrent epistaxis to speed up diagnosis. Genetic testing would be useful to establish the genetic-phenotype relationship in those with definite HHT as well as other family members. This will be essential for surveillance and screening of those with mutations. In a recent study by Cohen et al., 21 the economic advantages of genetic screening over repeated clinical screening can be substantial.
Referral pathways to ENT for epistaxis management should be implemented. A dedicated multidisciplinary clinic with a specialist nurse would allow for a more streamlined approach to such patients. In addition, having a dedicated HHT clinic for epistaxis would be an important consideration in coordinating future clinical trials. There should also be a support group to allow patients to draw from experience and to better inform and support the families. Due to the chronicity of this condition, advice of self-management of epistaxis will be instrumental. Currently, information for patients with HHT and their families is available through a number of self-help Web sites (country and language specific).
United Kingdom http://www.telangiectasia.co.uk
Ireland http://www.Gracenolan.com
United States and international http://www.hht.org
Denmark http://www.osler.dk
France http://www.amro-france.org
Germany http://www.morbus-osler.de
Italy http://www.hht.it
The Netherlands http://www.renduoslerweber.nl
That said, it should be appreciated that major hurdles remain due to the wide geographic distribution of these patients as well-funding issues. The NHS is operating at a time of austerity; the lack of coordinated funding to manage these patients with no specific tariff is not conducive to developing a dedicated multidisciplinary HHT service. The significant geographic distances that need to be covered by patients should the HHT service be centralized should also be borne in mind.
Recommendations
Analysis of our data indicates that there is a wide degree in variation of severity of epistaxis.
The management of epistaxis remains suboptimal, and treatment should best be tailored to the individual patient, ideally by a dedicated specialist or clinic.
A concerted effort to increase awareness of this disease among both families and physicians is necessary to reduce the diagnostic delay as well provide the necessary psychosocial support in dealing with this condition.
Conclusion
This is the first study to report on the HHT burden within the northeast U.K. community. As patients present with a wide degree in variation of severity of epistaxis, treatment should be tailored to the individual patient. A graduated treatment plan that incorporates conservative, nonsurgical measures to more aggressive surgical treatments can be considered.
Appendix A1
HHT Questionnaire
Section I: General History
What is your sex?
Male
Female
What is your age?
At what age was your diagnosis of HHT made
Is there a family history of HHT?
Yes
No
Details………..
What were your symptoms that led to the diagnosis?
Skin telangiectasia (tiny skin blood vessels)
Chest problems
Neurologic problems
Heart problems
Anemia/bleeding from your bowel
Nosebleeds
Other — please specify
Where was your diagnosis of HHT made?
General practitioner (GP)
Hospital
Other — please specify
What type of medical professional suspected/made the diagnosis of HHT in you?
General practitioner (GP)
Respiratory (lungs)
Gastroenterologist (gut)
Neurologist (brain)
Dermatologist (skin)
Ear, nose, and throat (ENT)
Other — please specify
Have you had genetic testing?
Yes
No
If yes to genetic testing, what is your HHT gene?
Endoglin
ALK1
Other
What resources have you found useful in obtaining knowledge about HHT? (Please circle all that apply)
General practitioner (GP)
Hospital doctor
Internet
Books
Patient groups
Other — please specify
Section II: Nosebleed History
Have you had nosebleeds?
Yes
No
Do you have nosebleeds from
One nostril
Both nostrils
How old were you when had the first nosebleed?
When was your last nosebleed?
On average, how frequent have nosebleeds been in the past 2 years?
Daily
weekly
monthly
few times a year
once a year
none
Have your HHT nosebleeds resulted in visits to accident and emergency department?
Yes
No
If yes, please specify how often:
Have the nosebleeds been severe enough to require a blood transfusion?
Yes
No
How many transfusions have you had in the past 2 years as a result of your nosebleeds?
Have you been unable to carry out your daily activities due to nosebleeds?
Yes — please specify
No
Who has treated your nosebleeds to date? Please circle all that apply?
General practitioner (GP)
Ear, nose, and throat (ENT)
Accident and emergency (A&E)
Other – please specify
Please rate how effective the nosebleed treatments you have used are. Mark N/A if you have not used the treatment before.
Other nosebleed treatment:
With regard to HHT nosebleeds, how would you rate the following:
Are you seeing (or have seen) an ENT specialist about your nosebleeds?
Yes
No