
Abstract
The application of image-guided systems to sinus surgery is gaining in popularity. This study tried to evaluate the efficacy of image-guided surgery (IGS) in the fenestration of the sphenoid sinus in patients with chronic rhinosinusitis (CRS) who received revision functional endoscopic sinus surgery (FESS). A total of 51 CRS patients who received revision FESS incorporating IGS between January 2010 and August 2011 by two surgeons were enrolled in this study. A group of 30 CRS patients who underwent revision FESS by the senior surgeon without incorporating IGS was chosen for comparison. The penetration rates for the sphenoid sinus were 91.2% when performed by the senior surgeon with IGS and 91.3% when done by the other surgeon with IGS. The penetration rate for the sphenoid sinus was 68.6% for revision FESS without IGS. The fenestration rate for the sphenoid sinus in revision FESS without IGS was significantly lower than that in revision FESS with IGS (p = .004). Our results showed that IGS was a beneficial procedure for opening the sphenoid sinus in the revision cases.
The sphenoid sinus is situated deep within the center of the skull base and is surrounded by important neurovascular structures. 6 Endoscopic sphenoidotomy is a common procedure during routine FESS. 7 Opening the sphenoid ostium is recommended when a patient's symptoms are suggestive of sphenoid obstruction or a disease is found in the region of the ostium or sphenoethmoid recess. 7 During FESS, it is possible for the surgeon to mistake a large posterior ethmoid cell (Onodi cell) for the sphenoid sinus. 8 Therefore, the surgical approach to the sphenoid sinus remains a great challenge for FESS. 9 To identify the sphenoid ostium, surgical anatomy of the sphenoid ostium has been studied, and a variety of endoscopic surgical techniques have been suggested.9,10 The purpose of this study was to investigate whether IGS could improve the success rate for the sphenoid sinus fenestration in CRS patients who underwent revision FESS.
Materials and Methods
Patients
An optical-based image-guidance system (Stealth-Station Treon; Medtronic, Inc., Louisville, CO) has been available to otolaryngologists at Taichung Veterans General Hospital, Taiwan, since January 2010. A total of 51 patients with CRS who underwent revision FESS incorporating IGS performed by two surgeons (authors of this article, Dr. Jiang is senior to Dr. Liang) between January 2010 and August 2011 were enrolled in this study. The diagnosis of CRS was based on a history of rhinosinusitis, the findings of nasal endoscopy, and an examination of computed tomography (CT) scans. 11 Duration of disease was qualified by continuous symptoms for at least 12 consecutive weeks. Nasal endoscopy identified discolored nasal drainage in the nasal cavities, nasal polyps, polypoid swelling, or edema of the middle meatus or ethmoid bulla. CT scans revealed mucosal thickening, complete opacification or air-fluid level of one or more sinuses. Any patient whose surgical specimen confirmed fungal balls or tumor growth in sphenoid sinus was excluded from the study.
Another group of 30 CRS patients with the same inclusion and exclusion criteria who underwent revision FESS, including endoscopic sphenoidotomy by the senior surgeon between September 2007 and December 2009, was chosen for comparison. The demographic data of the study subjects are shown on Table 1. This study was approved by the Institutional Review Board of Taichung Veterans General Hospital.
Characteristics of study subjects

IGS = image-guided surgery; CT = computed tomography; SD = standard deviation.
Analysis of Variance test.
Pearson's χ2 test.
CT Score
The preoperative CT scans were scored according to the staging methods described by Lund and Mackay. 12 The CT findings of maxillary, anterior ethmoid, posterior ethmoid, sphenoid, and frontal sinuses were graded as 0 to 2 (0 = clear sinus; 1 = partial opacification; 2 = total opacification), and the osteomeatal complex was scored as 0 or 2 (0 = not obstructed; 2 = obstructed). The right and left sinuses were scored independently.
Operative Procedures
The FESS procedures used the anterior to posterior and posterior to anterior modalities to open the diseased sinuses demonstrated by nasal endoscopy and CT. Endoscopic sphenoidotomy was performed if CT scans revealed a disease in the sphenoid sinus or endoscopy found a disease in the posterior ethmoid sinus. Whether the sphenoid sinus was successfully fenestrated was confirmed by image guidance system (Fig. 1) and recorded in the operation notes. The same FESS procedures were done in those patients without IGS, but whether the sphenoid sinus was successfully fenestrated was reviewed using the operation notes. Both surgeons used same operative procedures.
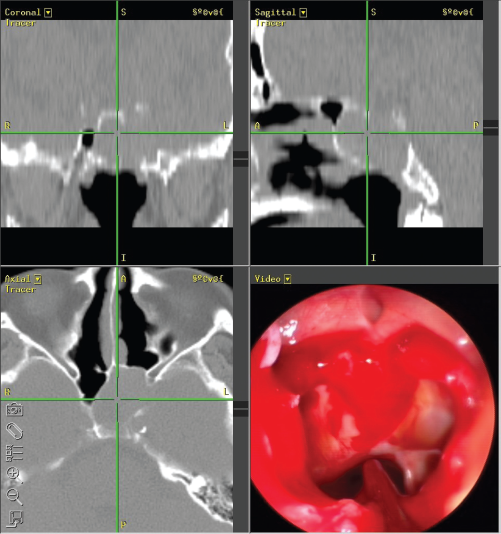
A suction probe of image-guided system has been placed in the sphenoid sinus; crosshairs on the CT images confirm this localization.
Statistical Analysis
The ages and CT scores of patients were compared among 3 groups by Analysis of Variance test, and the sex of patients was compared by Pearson's χ 2 test. Mann-Whitney tests were used to compare CT scores between IGS and non-IGS patients operated by the senior surgeon and those of patients operated between two surgeons. The success rates for the sphenoid sinus fenestration were compared between IGS and non-IGS patients receiving revision FESS using Pearson's χ 2 test. All computations were performed using SPSS version 17.0 (SPSS, Inc., Chicago, IL). Two-tailed p < .05 was considered statistically significant.
Results
Characteristics of Study Subjects
The characteristics of study subjects are listed in Table 1. The mean preoperative CT score was 7.93 ± 2.59 for 68 sinuses where revision FESS incorporating was performed by the senior surgeon and 7.35 ± 3.23 for 23 sphenoid sinuses where revision FESS incorporating IGS was performed by the junior surgeon. The mean preoperative CT score was 7.96 ± 2.21 for 51 sinuses where revision FESS without IGS was performed by the senior surgeon. The CT scores were not significantly different between IGS and non-IGS patients receiving revision FESS by the senior surgeon (p = .994) and were not significantly different between IGS patients receiving revision FESS by the senior and junior surgeons (p = .406).
Comparison of the Success Rate for the Sphenoid Sinus Penetration
Among 68 revision sphenoidotomies performed by the senior surgeon, 62 sphenoid sinuses were successfully opened using IGS. The success rate for the sphenoid sinus penetration was 91.2%. Among 23 revision sphenoidotomies by the junior surgeon, 21 sphenoid sinuses were successfully opened using IGS (success rate 91.3%). Among 51 revision sphenoidotomies performed without IGS, 35 sphenoid sinuses were successfully opened (success rate 68.6%). The success rate for the sphenoid sinus penetration was significantly higher when using IGS than without IGS for the senior surgeon (p = .004) but was not different between two surgeons (p = 1.000) (Table 2).
Comparison of the success rate for the sphenoid sinus penetration

IGS = image-guided surgery.
Pearson's χ2 test.
p < .05.
Discussion
Endoscopic sphenoidotomy has become the mainstay procedure when a sphenoid sinus requires opening. 8 Operations related to the sphenoid sinus have become considerably easier since the introduction of the Messerklinger technique in the 1980s because of advancements in sinus surgical instrumentation and the improvements in optical technology. However, it is often difficult to find the natural ostium of the sphenoid sinus, even for experienced surgeons. 6 Despite detailed review of preoperative CT images and meticulous surgical technique, complications of sphenoid sinus surgery can occur. 7
IGS is a real-time comparison of intraoperative anatomy, with preoperative imaging information showing the precise location of a surgical instrument within the surrounding structures.4,5,13 It has been shown that IGS allows the surgeons to comfortably operate with altered anatomy and facilitates a more complete operation.4,13 A recent metaanalysis provides evidence from current published literature that both major and total complications are less likely to occur with the use of IGS than the use of non-IGS during ESS. 14 In a nationwide questionnaire survey of image-guided FESS conducted in the United States in 2006, the authors found that the most commonly acceptable indication for IGS was revision surgery, followed by frontal and sphenoid sinus surgery. 15 In this study, we tried to evaluate the efficacy of IGS in revision FESS. We compared the success rates for the sphenoid sinus penetration with and without IGS in patients who received revision FESS. When IGS was done, the success rates were higher than 90%. However, when revision FESS was performed without IGS, the success rate dropped to 68.6%. The success rate was significantly higher when IGS was used than without IGS. This indicated that sphenoidotomy is difficult in revision FESS cases partly because of anatomic distortion in revision surgery or partly because of the existence of unfavorable factors, which resulted in the failure of primary FESS. With the IGS help, the success rate for the sphenoid sinus penetration was increased in our revision cases.
We also compared the success rates for the sphenoid sinus penetration between two surgeons when IGS was performed. Although the performance of FESS is different in the professional years between two surgeons in this study, the success rates were both higher than 90% with the aid of IGS. It implied that IGS might shorten the learning time of FESS.
Although our results showed that IGS was a beneficial procedure for opening the sphenoid sinus in the revision cases, it needs to be emphasized that this is a retrospective study. Some bias might have occurred. Patients in the IGS group and non-IGS group underwent FESS in different periods by the surgeon, the basic technique and experience should not change a lot before and after IGS usage. Moreover, whether the sphenoid sinus was successfully penetrated is more difficult to confirm without IGS. It is possible to mistake opening Onodi cell for penetrating sphenoid sinus. Therefore, the actual success rate for the sphenoid sinus penetration might be lower than 68.6% in non-IGS group.
The severity of disease has been evaluated by CT scans in this study. The Lund-Mackay scores were not different between IGS and non-IGS patients and between two surgeons. However, we did not evaluate the severity of disease in sphenoid sinus separately, because we thought that the severity of disease in sphenoid sinus was difficult to measure correctly using Lund-Mackay system.
With the IGS help, there still were six sphenoid sinuses in six revision cases, which could not be opened by the senior surgeon. According to Hamberger et al.'s classification of the pneumatization of the sphenoid sinus, 16 two sphenoid sinuses belonged to a conchal pattern and 3 sinuses were a presellar pattern. The last sphenoid sinus was much smaller than the contralateral one. On the other hand, whether IGS could reduce the complication rate in sphenoidotomy was not evaluated in this study.
Conclusion
Our results showed that IGS was a beneficial procedure for opening the sphenoid sinus, especially in the revision cases. However, it needs to be emphasized that this is a retrospective study, so some bias might have occurred.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article