
Abstract
Intracranial dermoid cysts are congenital ectodermal inclusion cysts that have a propensity to occur in the midline sellar, parasellar, or frontonasal regions. These cysts enlarge by means of glandular secretion and epithelial desquamation. Surgical resection has traditionally included a craniotomy, but endoscopic approaches are now used with increasing regularity. A binostril approach is normally used to access dermoid cysts due to the midline nature of the lesions. In this case report, we describe the successful surgical resection of a dermoid with 1.5-cm of intracranial extension using a unilateral endonasal endoscopic approach with no complications and with no postoperative anosmia. Although the unilateral endoscopic technique is not plausible for all epidermoid or dermoid cysts of the anterior cranial fossa, it should be considered a viable alternative technique when faced with a dermoid limited to one side of the falx cerebri.
Although a craniotomy was previously considered mandatory to achieve gross resection of intracranial dermoids, more recently, endoscopic approaches have been used with excellent success.3,4 Endoscopic techniques produce superb visualization during tumor excision and eliminate postoperative cosmetic concerns. However, preservation of olfaction is difficult because a large portion of the anterior cribriform plate is resected for surgical access to the tumor. This article details the unique case of a unilateral endoscopic approach to an intracranial dermoid cyst that resulted in preservation of contralateral olfactory function.
Case Report
A 46-year-old man presented with a history of worsening headaches over the past several weeks. He denied nasal congestion, epistaxis, visual changes, and anesthesia or weakness of his face. His head and neck examination as well as a diagnostic nasal endoscopy were unremarkable. Because of his worsening headaches, a computed tomography scan of the paranasal sinuses was obtained that showed a right cribriform mass that appeared to originate from the anterior cranial fossa eroding the right side of the crista galli (Fig. 1 A). A magnetic resonance imaging scan confirmed the presence of a 1.5 × 1.5-cm cystic mass (Fig. 1 B).
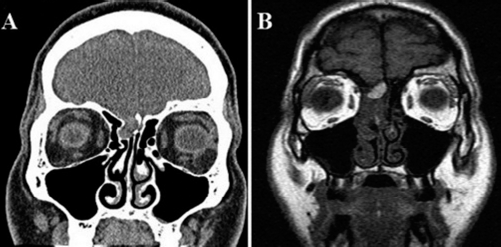
Coronal (A) computed tomography scan and (B) T1-weighted magnetic resonance imaging scan showing an asymmetric olfactory mass.
After discussing the surgical options and associated risks with the patient, he elected to undergo transnasal endoscopic resection of the intracranial dermoid cyst, rather than open bifrontal craniotomy. Because of the position of the cyst to the right side of the crista galli and falx cerebri on imaging, we discussed the possibility of conserving olfaction with a strictly unilateral approach. However, he was informed to expect anosmia if a bilateral, binostril approach was required for complete resection. Intraoperatively, a right-sided full endoscopic sinus surgery was performed with a wide maxillary antrostomy, traditional sphenoethmoidectomy with skeletonization of the skull base, and a frontal sinusotomy. The middle turbinate was also resected. The dura was incised anteriorly, the cyst contents were identified, and the capsule was dissected off of the crista galli (Fig. 2 A). It was elevated and retracted away from the brain and falx cerebri. The involved dura and olfactory bulb of the olfactory cleft were removed (Fig. 2 B). Importantly, the cyst was isolated to the right of the falx cerebri and crista galli providing the opportunity to spare contralateral olfaction. Multilayer closure was performed with a Biodesign dural graft (Cook Medical, Bloomington, IN), underlay graft, and an ipsilateral septal flap (Fig. 2 C). The patient had an excellent recovery from the surgery and was discharged on postoperative day 1. He is clear of recurrent cyst at 6 months of clinical and imaging follow-up with no change in the sense of smell according to the patient.
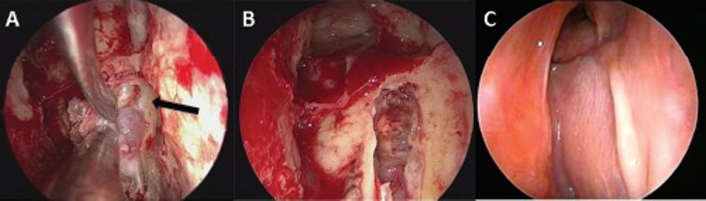
Transnasal endoscopic views of the (A) intraoperative dissection of the cyst off the side of the crista galli (arrow, crista galli), (B) final defect after cyst removal, and (C) 6-month postoperative image with the nasoseptal flap well healed and frontal sinus patent.
Discussion
The only definitive treatment for dermoid cysts is surgical removal. Surgical resection has been associated with significant morbidity, including meningitis, anosmia/hyposmia, cerebral spinal fluid leak, damage to the sinuses, intracerebral hemorrhage, cerebral edema, epilepsy, memory and concentration deficits, and osteomyelitis.3,5,6 Additionally, incomplete removal of the cysts may result in up to a 100% recurrence rate. 5 Bilateral endonasal approaches are described in the literature but are accompanied by the risk of hyposmia/anosmia. Duz et al. 7 described an endonasal resection of a 1.8 × 2.5 × 2-cm intradural dermoid cyst in the frontobasal region. However, they left the lining of the cyst because it was adhered to neural and vascular structures and is, thus, highly likely to recur. The senior authors (B.A.W., and K.O.R.) previously reported on transnasal endoscopic resection of two large intracranial dermoid cysts that had 4- to 5-cm parenchymal extension into the frontal lobe. 3 A bilateral endoscopic approach was required and both patients have anosmia secondary to the large skull base resection required for access. In the current subject, there was 1.5 cm of intracranial extension but the unilateral endoscopic technique spared his sense of smell on the contralateral side.