
Abstract
Allergic rhinoconjunctivitis denotes both nasal and ocular manifestation of allergy, which may be solely treated with intranasal steroid. This study compares the efficacy of mometasone furoate nasal spray (NS) and fluticasone furoate NS in treatment of allergic rhinoconjunctivitis. The secondary objective is to study the severity of baseline ocular symptoms in allergic rhinoconjunctivitis. Seventy-eight patients with allergic rhinoconjunctivitis were assessed subjectively and objectively using twice-daily symptom scores for nasal (reflective total nasal symptom score [rTNSS] and instantaneous TNSS [iTNSS]) and ocular (reflective total ocular symptom score [rTOSS] and instantaneous TOSS [iTOSS]) symptoms, rhinoconjunctivitis quality-of-life questionnaires (RQOLQs), and acoustic rhinometry. All measurements were taken at baseline and at 4 and 8 weeks of treatment. Sixty-three patients who were randomized into the mometasone furoate group (n = 36) and the fluticasone furoate group (n = 27) completed the study. Seventy-six percent of patients had mild ocular symptoms, 20.5% had moderate symptoms, and only 2.6% had severe symptoms at baseline based on the iTOSS; 65.1% had mild nasal symptoms and 3% had severe nasal symptoms. There was significant reduction in the symptom scores after 1 week (p < 0.05). Both groups had significant improvement in RQOLQ scores after 1 month, which further improved at 2 months (p < 0.05). The nasal dimensions also improved in both groups (p < 0.05) but there was no statistically significant difference between groups. Both mometasone furoate and fluticasone furoate are effective as single-modality treatment of allergic rhinoconjunctivitis. The majority of patients manifest mild ocular symptoms that may be solely treated with intranasal steroids.
To our knowledge, there has been no head-to-head study that compares fluticasone furoate NS and mometasone furoate NS in the treatment of persistent allergic rhinoconjunctivitis. There is also no prospective study that focuses on treatment of ocular symptoms solely with mometasone furoate NS, making its use for allergic rhinoconjunctivitis less popular in our center. Hence, this study was performed to compare the efficacy between mometasone furoate NS (Naso-nex; Merck Sharp & Dohme Corp., Heist-op-den-Berg, Belgium) and fluticasone furoate NS (Avamys; Glaxo-SmithKline, County Durham, UK) by objective and subjective means using the acoustic rhinometry, daily documentation of nasal and ocular symptoms severity, and the rhinoconjunctivitis quality-of-life questionnaire (RQOLQ). As a secondary objective the severity was assessed of the ocular symptoms in allergic conjunctivitis. Although ocular symptoms have been found to occur hand in hand with allergic rhinoconjunctivitis, the severity of these ocular symptoms has not been formally studied.
Materials and Methods
Study Design
This was an 8 week, randomized, investigator-blinded study to compare efficacy of mometasone furoate NS and fluticasone furoate NS for treatment of allergic rhinoconjunctivitis. It was conducted in the Otorhinolaryngology Clinic, Universiti Kebangsaan Malaysia Medical Center after obtained approval by the local ethics committee. An approval from the Institutional Review Board was obtained before commencement of this study.
Patients between 12 and 59 years old were invited to participate in this study if they had both nasal and ocular symptoms of allergic rhinoconjunctivitis present for >2 years with a positive skin-prick test. Patients were excluded if they were pregnant, had other nasal conditions causing nasal obstruction such as severe deviated nasal symptoms or nasal polyps, were smokers, or were using INS or oral steroids for 4 weeks before the baseline period. Patients who were on other INSs were required to undergo a washout period of 4 weeks. Patients were dropped from the study if they did not complete 80% of their symptom scores in their diary or were noncompliant to treatment.
Patients who met the criteria were screened by undergoing a 2-week baseline period to assess severity of their symptoms using a provided diary. They were allowed rescue medications (tablet loratadine at 10 mg with a maximum dose of once daily). After the baseline period, the severity of nasal and ocular symptoms was evaluated. Those with zero ocular symptoms were dropped from the study. Only patients with documented nasal and ocular symptoms were randomly assigned using a computer-generated code of 0 and 1. Investigator blinding was maintained by a dedicated pharmacist who did not disclose the treatment groups until all patients had completed the study. Fluticasone furoate NS and mometasone furoate NS were provided in a metered nasal pump spray bottle. Mometasone furoate NS uses a top activating device that was administered at 200 μg once daily whereas the more concentrated fluticasone furoate NS uses a side activating device administered at 110 μg daily. Patients were then scheduled to visit at 4 and 8 weeks of treatment for assessment of efficacy. Compliance of patients during treatment was assessed on follow-up visit by interview and also diary documentation.
Assessment of Efficacy
Patients were provided a diary to score the severity of their nasal (rhinorrhea, congestion, sneezing, and itching) and ocular symptoms (watering, itching, and redness) using a 4-point categorical scale from 0 to 3. 11 The total nasal symptom score (TNSS) is defined as the combined total score of the nasal symptoms. Total ocular symptoms score (TOSS) is the total of all three ocular symptoms. These scores were recorded twice daily and separated into reflective and instantaneous scores. Reflective scores (reflective TOSS [rTOSS] and reflective TNSS [rTNSS]) were scored twice daily: before administering morning dose and 12 hours later. It addressed the question, “how have you felt for the past 12 hours?” Instantaneous scores (instantaneous TOSS [iTOSS] and instantaneous TNSS [iTNSS]) represent patients symptoms at the time of evaluation and was performed once daily before dose administration. The main measure for efficacy was the instantaneous scores (iTNSS and iTOSS). The scores were averaged per week and used to categorize patients into mild-moderate and severe symptoms (Table 1). Efficacy was measured by comparison of mean weekly scores to baseline (the higher score out of the 2-week baseline period). Mean weekly scores were also used to compare the efficacy between the two treatment groups.
Severity of symptom scores scale

TNSS = total nasal symptom score; TOSS = total ocular symptom score.
The Junipers RQOLQ was used to assess the quality of life before and after treatment with INS. 12
Objective assessment was performed using acoustic rhinometry (RhinoScan, Interacoustics, Assens, Denmark). The nasal dimensions recorded were the minimal circumferential area 1 (MCA1) and MCA2. The measurements were performed by one investigator to avoid interobserver error.
RQOLQ and acoustic rhinometry measurements were performed at baseline and at 4 and 8 weeks of treatment. Measurements were also taken at 8 weeks of treatment because there was lack of data regarding response of ocular symptoms in allergic rhinoconjunctivitis at 4 weeks.
Statistical Analysis
Collected data was coded and entered into SPSS Version 20 (SPSS, Inc., Chicago, IL) for evaluation. Statistical analysis was calculated based on the change from baseline. A two-sided test were used to assess efficacy of treatment and also to compare the efficacy between the treatment groups. Values of p < 0.05 were considered significant.
Results
Seventy-eight patients fulfilled the inclusion criteria after they completed their baseline diaries; 76.7% had mild ocular symptoms, 20.5% had moderate symptoms, and only 2.6% had severe ocular symptoms; 65.1% had mild nasal symptoms and 3% had severe nasal symptoms at baseline.
Fifteen patients were dropped from this study, making the total dropout rate of 19.2%. The main reason for dropout was noncompliance to medications and default of follow-up. The remaining 63 patients completed the study with satisfactory diary documentation. Of these 63 patients, 27 were from the fluticasone furoate NS treatment group and 36 were form the mometasone furoate NS treatment group. There were 27 male (42.9%) and 36 female (57.1%) patients with a mean age of 28.65 ± 1.22 years (Table 2).
Demographic data between mometasone furoate NS and fluticasone furoate NS groups

NS = nasal spray.
Symptom Score
The mean iTNSS for mometasone furoate NS and fluticasone furoate NS were 4.85 ± 2.56 and 4.95 ± 2.77, respectively, and the mean iTOSS were 3.15 ± 2.05 and 2.38 ± 1.43, respectively, at baseline. There were no significant differences in the baseline scores between the study groups. Both groups showed significant reduction in nasal and ocular symptoms after 1 week of treatment (p < 0.05; Table 3). However, there were no significant differences in symptoms scores after treatment between the groups (Fig. 1).
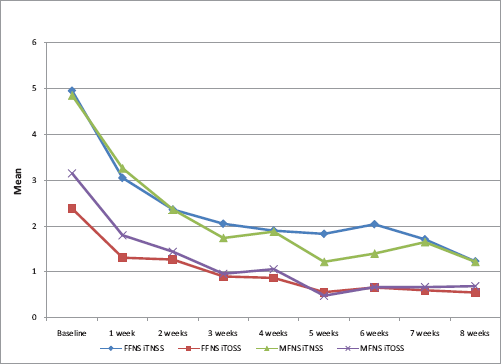
Comparison between instantaneous total nasal symptom score (iTNSS) and instantaneous total ocular symptom score (iTOSS) after treatment with mometasone furoate nasal spray (NS) or fluticasone furoate NS. There was no statistical difference in efficacy between the two intranasal steroids.
Symptom score at baseline and after treatment for mometasone furoate NS and fluticasone furoate NS

Boldface type indicates significance at a value of p < 0.05.
NS = nasal spray; rTNSS = reflective total nasal symptom score; iTNSS = instantaneous total nasal symptom score; rTOSS = reflective total ocular symptom score; iTOSS = instantaneous total ocular symptom score.
Rhinoconjunctivitis Quality-of-Life Questionnaire
The overall RQOLQ scores at baseline were 3.5 and 3.39 for fluticasone furoate NS and mometasone furoate NS, respectively. The baseline sores for all domains were not significantly different at baseline. Both groups showed significant reduction in RQOL sores after 1 month of treatment, which was further reduced after 2 months of treatment (Table 4).
Comparison RQOLQ scores between mometasone furoate NS and fluticasone furoate NS at baseline (1 and 2 mo)

NS = nasal spray; RQOLQ = rhinoconjunctivitis quality-of-life questionnaire.
Acoustic Rhinometry
The nasal dimensions measured on acoustic rhinometry were significantly increased after 1 and 2 months of treatment in both groups. The total MCA1 increased from 0.42 to 0.47 cm2 after 1 month of treatment and further improved to 0.50 cm2 after 2 months for patients treated with mometasone furoate NS. Patients treated with fluticasone furoate NS also achieved a similar increase on total MCA1 from baseline (0.47 cm2) and after 1 month (0.56 cm2). Comparison between groups did not show any statistically significant difference. Fluticasone furoate NS showed a statistically significant improvement in total MCA1 over mometasone furoate NS after 1 month of treatment but not at 2 months (Table 5).
Comparison of nasal dimensions between mometasone furoate NS and fluticasone furoate NS
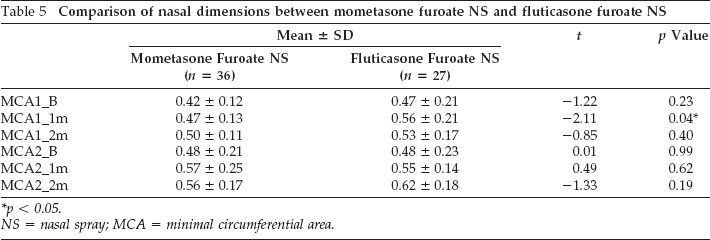
p < 0.05.
NS = nasal spray; MCA = minimal circumferential area.
Adverse Effect
The incidence of adverse effect during this study was 36.1% for mometasone furoate NS and 22.2% for fluticasone furoate NS. Overall adverse effect incidence was 30.1%. The most common adverse effect was pharyngitis. There were no reports of nasal pain or epistaxis during this study.
Rescue Medications
Patients were permitted rescue treatment (tablet loratadine at 10 mg) during the course of this study if their symptoms were not controlled with medications. For the mometasone furoate NS group the mean tablet taken per patient was 3.1 tablets during the 2-week baseline period, 3.0 tablets during the first 4 weeks, and 3.0 tablets during the second 4 weeks of treatment. The fluticasone furoate NS group, on the other hand, only needed 1.89 tablets during baseline, 0.85 tablets during the first 4 weeks, and 0.7 tablets during the last 4 weeks. The overall mean tablets taken for mometasone furoate NS group were 3.0 tablets per patient and only 1.1 tablets per patient were needed in the fluticasone furoate NS group.
Discussion
Allergic rhinoconjunctivitis is often used interchangeably with allergic rhinitis because ocular symptoms are usually present in allergic rhinitis. Studies have found a high incidence of watery/itchy eyes in allergic rhinoconjunctivitis (61–81%)3,13 but did not specify the severity of the eye symptoms. A study in Switzerland reported that only 22.4% of patients considered ocular symptoms to be the most bothersome symptom in seasonal allergic rhinoconjunctivitis. 14 Our study showed that the majority of patients with persistent allergic rhinoconjunctivitis had mild ocular symptoms. Our mean baseline TOSS was 3.15 and 2.38 for each treatment group. This reflected the mild ocular symptoms experienced by the majority of our patients. Tolerance due to constant exposure to dust mites, which is the most common 15 allergen for perennial allergic rhinitis in our country, may explain the mild symptoms. Another study in Europe on perennial allergic rhinoconjunctivitis that used the same 4-point categorical scale found a relatively low baseline ocular score of 4.2 16 compared with a study of seasonal allergic rhinoconjunctivitis, 17 which reported a score of 6.3. This suggests that ocular symptoms in patients with persistent allergic rhinoconjunctivitis tend to be less severe 18 and less prevalent than seasonal allergic rhinitis. 19 Additional studies on ocular symptoms and their relation to other atopies would be useful to understand the mechanism of ocular allergies and its best option of treatment.
There has been mounting evidence that supports INS as a single-modality treatment for both nasal and ocular symptoms of allergic rhinoconjunctivitis.20,21 Consistent with previous studies, this study indicated reduction in nasal and ocular symptom for both mometasone furoate NS22,23 and fluticasone furoate NS. 24 Both INSs are equally effective and attained optimal efficacy after 1 month of treatment together with improvement of ocular symptoms. Although fluticasone furoate NS is thought to be pharmacologically superior to other INSs it did not translate into superior clinical efficacy in this study. 25 Other INSs have been studied for treatment of allergic rhinoconjunctivitis. Triamcinolone acetonide NS was found to be equally as effective as fluticasone propionate and loratadine. 26 Beclomethasone NS, a first-generation INS, was also effective when compared with placebo in relieving ocular symptoms. 27 In contrast, there is limited study on the efficacy of ciclesonide NS on ocular symptoms of allergic rhinitis. A study by Ratner et al. 28 did not find any significant reduction in ocular symptoms when comparing ciclesonide NS with placebo. Although there may still be some contradictory evidence, INS remains a powerful pharmacologic tool for the treatment of allergic rhinoconjunctivitis.
Both treatment groups attained optimal efficacy after 1 month of treatment together with improvement of ocular symptoms. Krouse et al. 29 reported that the optimal duration for perennial allergic rhinitis study was 4 weeks. Based on our experience, this may also be applied for allergic rhinoconjunctivitis. However, evidence only supports use of INSs for ocular symptoms of allergic rhinoconjunctivitis. Primary allergic conjunctivitis is treated with antihistamines or mast stabilizing eye drops. 20 Rosenwaser et al. 30 found fluticasone furoate NS was not effective for treatment of primary allergic conjunctivitis.
The overall RQOLQ scores were significantly improved after 1 month with further improvement after 2 months in both groups. A population study performed found that the average overall RQOL score for patients without any allergic rhinitis was 0.2. 31 We found the overall score for mometasone furoate NS and fluticasone furoate NS reduced to 0.66 and 0.77, respectively, after 8 weeks of treatment from the baseline score of 3.5 and 3.39 for each treatment group. Therefore, INS improves quality of life but not to the normal population score even after 8 weeks of treatment. Furthermore, patients with persistent allergic rhinitis had been found to have poorer quality of life compared with the intermittent group. 32
Objective assessment was included in this study to support any difference in efficacy using acoustic rhinometry. The MCA1 usually corresponds with the anterior portion of the inferior turbinate because it measures the most narrow portion between 1 and 3 cm from the edge of the vestibule, which represents the valve area. The lower the MCA indicates a higher degree of nasal obstruction. Patients with mucosal disease will have a lower MCA, which agrees with our study where mean baseline MCA1 for our patients were 0.42 and 0.48 cm2 for each treatment group. Improvement in MCA1 translates into reduction of nasal congestion. 33 Consistent with subjective improvement, the MCA of our patients has also improved. Although there was a statistically significant difference between mometasone furoate NS and fluticasone furoate NS in reducing MCA1 in the 1st month, it was not supported by the subjective assessment.
The limitation of this study was the small number of patients because of difficulty recruiting patients with persistent eye symptoms with allergic rhinitis. There were also a large number of patients with only mild ocular symptoms in this study with high variability.
Conclusion
The majority of these patients experienced mild ocular symptoms. Both intranasal steroids subjectively and objectively improved allergic rhinoconjunctivitis. Therefore, both can be suitably used as a single modality treatment for both nasal and ocular symptoms.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article
Acknowledgments
The authors thank the members of the Pharmaceutical Department at the University of Kebangsaan Malaysia Medical Center who kindly assisted in the blinding procedure of this study.