
Abstract
The safety of shared specific vaccines (SSVs) has been questioned by some experts. The purpose of this study was to evaluate the safety of SSVs. Details of systemic allergic reactions after subcutaneous immunotherapy injections were captured on a standardized form from July 2005 to July 2010. Patient records were evaluated for factors that might be associated with increased rate of systemic reactions and, in addition, were examined for any errors. Systemic reaction rates (SRRs) using a combination of shared and patient-specific vaccines (PSVs) were similar to previously reported studies (0.23 reactions per 100 shots). There were no systemic reactions resulting from errors where the incorrect shared allergen was administered, but we did note one reaction after an erroneously administered PSV. There were two dosage errors associated with both shared and patient-specific immunotherapy. Most reactions were mild to moderate (World Allergy Organization grade, 1 or 2). Severe reactions with 911 activations were noted in six patients. Thirty percent of reactions occurred out of the office and the average time to reaction was 48 minutes. Epinephrine was administered in only 60% of patients. Epicutaneous reactivity to mites, cats, dogs, and pollen but not mold occurred significantly more in reactors. Differences in SRRs were encountered between satellite offices. Using a combination of SSV and PSV, SRRs were similar to previously reported studies; moreover, no systemic reactions occurred where a SSV was erroneously administered. SRR surveillance is a useful safety tool.
SCIT is considered a safe procedure with a low prevalence of systemic reactions; however, severe systemic reactions have been documented in a small number of patients. These reactions include cases of fatal anaphylaxis secondary to SCIT: Lockey reported 46 fatalities after SCIT over a 45-year period, 6 and a survey from the American Academy of Allergy Asthma and Immunology reported 41 fatalities over a 12-year period. 7
Shared specific vaccines (SSV) refers to the practice of administering a single aliquot from the same allergen immunotherapy vaccine vial to two or more individuals, as opposed to patient-specific vaccines (PSV) where a single vial is prepared for each patient. SSV does not refer to the practice of drawing up aliquots from several vaccine vials into the same syringe. SSV is widely used in certain states and regionally 8 ; however, PSV is preferred by most allergy program training directors. 8
The safety of SSV has been questioned. Aaronson and Gandhi 9 published the results of an e-mail survey documenting immunotherapy errors and reported 527 systemic reactions. This included 24 reactions requiring hospitalization and 1 death. This survey did not document the association of these reactions with either PSV or SSV. However, they concluded that as an important way of reducing errors, “All vials should be patient specific, and off-the-board treatment with common vials of vaccine (SSV) should be discontinued.”
The purpose of this study was to evaluate the safety of SSV over 5 years in a single specialty group allergy practice where both SSV and PSV are used as well as to examine the properties and the patient profiles associated with these reactions.
Methods
All patients receiving allergen immunotherapy injections for inhalant allergens in our practice from 2005 through 2010 were included in this study that was retrospective in design. We have, however, instituted a standard office protocol where all systemic reactions were recorded on a standard form approved by American Academy of Allergy Asthma and Immunology that captured the details of the reactions. 10 These were scanned into the patient's electronic record and then filed centrally for future analysis. In addition, in the case of patients who developed systemic reactions after leaving our office, no further injections were given without an office visit with an allergist. The details of the prior reaction were recorded on the same form during this visit. Patient records were evaluated for factors that might be associated with increased rates of systemic reactions and for any dosing errors or errors in vaccine administration. The number of patient immunotherapy encounters per year was obtained from the computerized medical record database. This study included only data on patients who were receiving immunotherapy injections in our practice and did not capture data from “send out” vaccines, administered in other practices using extract provided by us.
Immunotherapy patients in our practice typically are placed on customized vaccines depending on their skin test profile with epicutaneous and if needed intradermal testing, as well as clinical history in accordance with the current immunotherapy practice parameter. 11 Seventy-seven percent of patients received at least one treatment with SSV and may have had a second or third vaccine with PSV. Over 90% of patients who received SSV received one or more vaccines of dog; cat; dust mite; Dermatophagoides farinae/Dermatophagoides pteronyssinus; or a tree, grass, and weed mix. All patients receiving “send out” vaccines received PSV. Immunotherapy build-up typically consisted of weekly injections for 20 weeks. The target maintenance dose of allergen was consistent with that recommended in the practice parameter.
One hundred seventeen records of patients who had never had a systemic reaction and had been on SCIT for at least 6 months were reviewed for comparison regarding prevalence of allergic sensitization profiles, asthma controllers, and large local reactions. Statistical significance was evaluated by independent chi-squared analysis.
This study was submitted to our local Institutional Review Board (Southern New Hampshire Medical Center) and was judged to meet exempt status.
Results
Over the 5-year period, 230 systemic reactions were recorded in a total of 98,007 immunotherapy patient encounters. Women comprised 57.5% of patients, with a mean age of 34.7 years, and 83% were white. These values did not differ from a group of nonreactors who had been on immunotherapy for at least 6 months.
The clinical characteristics of reactors are shown in Table 1. There was considerable variance in terms of the time on SCIT and on maintenance, with a range of just a few weeks to 12 years, accounting for the large standard deviations. The preponderance of reactions occurred during the build-up phase but over one-third did occur on maintenance. Large local reactions were frequently observed. The percentage of patients on inhaled steroids and montelukast were not statistically significantly different from nonreactors (37.8% versus 32.6% [p = 0.32] and 19.5% versus 14.4% [p = 0.21]).
Clinical characteristics of reactors

SCIT = subcutaneous allergen-specific immunotherapy; PSV = patient-specific vaccine; ACE = angiotensin-converting enzyme.
The features of systemic reactions and treatments are presented in Table 2 using the World Allergy Organization (WAO) Subcutaneous Immunotherapy Systemic Reaction Grading System. 12 Only 17% of reactions were moderately severe or severe (grade 3 or 4), but six patients required transport to the emergency department and no fatal reactions occurred. The mean time to reaction was 48 minutes; however, a large variance was noted from just a few minutes to 24 hours in one patient.
Features of systemic reactions and treatments

WAO = World Allergy Organization; PEF = peak expiratory flow.
Two systemic reactions were noted to be associated with errors in dosing. These were both secondary to the previous dose having been recorded incorrectly. No reactions were associated with incorrect SSV injections where the incorrect shared allergen mix was injected; however, we did document one reaction where a PSV was erroneously administered to the wrong patient.
The time to onset of reaction in Fig. 1 shows the large variance.
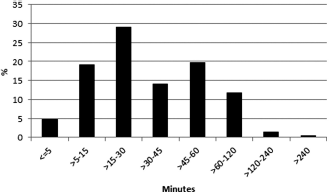
Histogram of time to onset of reaction.
Only 52% of reactions occurred within 30 minutes of injection administration. The epicutaneous testing reactivity profile of reactors shown in Table 3 was statistically significantly greater compared with the nonreactors for all aeroallergens groups except for molds.
Sensitization profile of reactors percent positive epicutaneous tests

The treatments used for the systemic reactions are noted in Table 4. Approximately 30% of patients reacted after leaving the office and either self-medicated or received treatment at another facility.
Treatment of systemic reactions and dosage adjustments (in percentages)

The variation of systemic rates by office per year in Fig. 2 shows significant variability between different offices. The global mean reaction rate was 0.23 per 100 patient immunotherapy encounters or 0.10 per 100 injections.
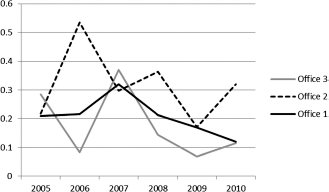
Systemic reaction rate by office.
Figure 3 represents a Kaplan-Meier survival analysis of percent of patients without systemic reactions over the 5-year period. Each year and cumulatively 2.8% of patients had a systemic reaction.

Kaplan-Meier survival analysis of percent of patients without systemic reactions.
Discussion
Studies of immunotherapy-induced systemic reactions have reported the systemic reaction rate (SRR) per 100 injections. The literature is not always clear whether the term “injections” means immunotherapy encounters or actual number of injections given. Reported SRR in these studies have varied widely and most do not state whether PSV or SSV have been used. In part, this variance can be explained by a variety of build-up regimens used. Winther 13 reported a rate of 2.5%; however, they used a modified cluster regimen and included both venom and inhalant allergens. Tinkelman 14 reported the results of their 1-year prospective study with SRR of 0.054, but patients only waited for 20 minutes and they may have missed numerous delayed reactions. Alsamarai 15 reported an SRR of 0.25 in a 9-year prospective study using European Academy of Allergology and Clinical Immunology reporting system. 16 Cox et al. 11 documented an average SRR of 0.2 per 100 injections with conventional inhalant allergen immunotherapy. Sheikh reviewed the SRR literature and reported a mean SRR of 0.5. 17
This is one of the first studies we are aware of specifically examining the safety of SSV. The mean SRR reported over a 5-year period of 0.23 per 100 immunotherapy encounters or 0.1 per 100 injections is consistent with other reported SRR studies. The SRR in our study did vary by year and also by office and we believe this is a useful surveillance tool both at the office and at the individual nurse level to identify outliers in terms of SRR. Most of these reactions were mild (grade 1 or 2). We labeled any patient who had a drop in blood pressure as grade 4. Nine of 15 patients so classified promptly responded to epinephrine and were discharged. Six patients (2.6%) had severe, possible life-threatening reactions that required transportation to the emergency room. This rate is similar to the frequency of class 3 reactions previously reported by Bernstein. 18 This classification system, however, differs from the WAO grading system in that unlike class 3 reactions, WAO grade 4 reactions do not require severe life-threatening anaphylaxis for inclusion. We believe this is confusing, because non-life-threatening reactors with transient hypotension are included as class 4, some of whom may have had a vasovagal component.
Although it may appear that we have a higher percentage of more severe reactions, compared with this study, we believe that the data are not comparable. First, our data set, unlike Bernstein's study where practitioners were asked to recall reactions over the past year, did not rely on physician recall. Second, we do believe that our data set is complete, capturing all of the reactions. Third, it is possible that many of the patients who were placed in class 2 in this study would under the new WAO classification be upgraded to grade 3. Finally, whereas ~50% of our patients had persistent asthma, a risk factor for more severe reactions, these data are not included in their study.
The safety of SSV has been documented in a second study published in an abstract by Sheikh et al. from Beth Israel Hospital in Boston who performed a 2.5-year prospective study. 17 This group uses SSV exclusively, incorporating only what they consider major allergens into their treatment. They reported an even lower SRR of 0.02, although in their definition of systemic reactions they included only WHO grade 2 or greater and the rate reported was per injection not immunotherapy encounter (personal communication, Javed Sheikh, Beth Israel Deaconess Hospital).
Importantly, no errors in either study were documented where the administration of the wrong SSV vaccine resulted in a systemic reaction. One patient had a systemic reaction after the incorrect PSV. There were two dosage errors recorded in our study, one of whom received SSV.
Reactions have also been reported as reaction rate per patient. This must be adjusted as the reaction rate per patient per year to compare different studies. None of the studies that we reviewed were reported in this format. In addition, the number of reactions needs to be adjusted for multiple reactors. The reaction rate in our study was 2.8 reactions per 100 patients per year. Reactions rates per patient are, however, optimally visualized by Kaplan-Meier analysis (Fig. 3) of percent of patients surviving without systemic reactions.
The third update of the immunotherapy practice parameter 11 while accepting SSV as a valid form of treatment, states, “Individually prepared and labeled vials are recommended because they have several potential advantages over shared vials (i.e., vials of allergen extract used for multiple patients). These potential advantages include being able to prepare labels with specific patient identifiers, less distractions during mixing, and less frequent mixing.” We believe that the latter part of this statement is factually incorrect, in that there is more wastage in the preparation of PSV, because this usually includes at least one reserve dose. In addition, the preparation of PSV in the allergy laboratory requires many more steps that are repeated for each patient than an equivalent SSV vial. This statement does not recognize the increased potential for errors associated with PSV in the allergy laboratory. The most severe reaction we have observed in our practice was one of the 24 patients requiring hospitalization reported by Aaronson and Gandhi. This patient had life-threatening anaphylaxis requiring intubation and ventilation with almost a week spent in the intensive care unit. The reaction occurred after the first dose from her top concentration and resulted from an allergy laboratory error where the vaccine provided to us by a board-certified allergist had not been diluted. Protein analysis revealed that the build-up bottles did not contain any allergen.
The properties of reactions and reactors were also examined. Angiotensin-converting enzyme inhibitors (ACEI) have been proposed to increase the risk of anaphylaxis. There did not appear to be an association of ACEI use with systemic reaction, and patient's ACEI regimens were not altered before initiating immunotherapy. β-Blocker use was also noted in a small number of patients with systemic reactions, but every effort was made not to place patients on this class of medication on immunotherapy.
Almost 25% of patients who had a systemic reaction had a previous systemic reaction at any time, and 38 of the reactions in the study were recorded in patients who reacted previously during the study period, confirming that this is a high-risk group who need to be treated cautiously. Large local reactions occurred in 61% of patients with a rate of 67% in nonreactors. It became obvious that the significance of this data was flawed in that this was retrospective and a uniform definition of what comprised a large local reaction was not adopted by all of the nurses. In addition, some of these reactions were delayed and were self-reported by the patient.
Over one-third of patients were on asthma controller medications. Uncontrolled asthma has been associated with increased systemic severity and possibly an increased SRR. 11 Reactors in this study, however, did not appear to have a greater prevalence of persistent asthma as judged by the use of asthma controllers compared with nonreactors. We did not examine differences in asthma severity or control in these two groups.
The significantly enhanced epicutaneous reactivity in reactors indicates that this may be a risk factor for the development of systemic reactions.
Although systemic reactions may occur with refills of new vaccines, only 11% of reactions were associated with vaccine refills in the case of PSV, all of whom received a cut back in the dosage. This implies that this is not a major risk factor for reactions.
The mean time to reaction of 48.4 minutes and 30% of reactions occurring out of the office suggests that although we are following current immunotherapy guidelines and requesting a 30–minute wait period, a longer wait of 45 minutes may be needed and high-risk patients should receive an epinephrine autoinjector. We do accept that the actual time recorded beyond 30 minutes is subject to significant recall bias by patients and, in addition, the median time to reaction was 30 minutes. Surprisingly, only 60% of patients received epinephrine. This may have been because of the mild reactions noted in many patients and the delayed onset of reactions in other patients who had already left the office. Only 12% of patients who receive epinephrine received a second dose. This is lower than published reports in the patients presenting with food 19 or stinging insect-induced 20 anaphylaxis.
In summary, we provide evidence that in a practice that extensively uses SSV, this is safe and in a setting with trained allergy nurses was not associated with an increased SRR or an increased number of errors.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article
Acknowledgments
The authors thank Dr. Javed Sheikh and Dr. George Vaida for review of this article and Rachel Melamed and Venkatarama Krishnan, Ph.D., for statistical analysis.