
Abstract
Although a variety of theories have been proposed about functions of the paranasal sinuses, not one is clear today. Nonetheless, paranasal sinus–related diseases are associated with a high rate of morbidities. Therefore, it is essential to identify the structure and pathophysiology of the paranasal sinuses. Computed tomography (CT) is a valuable tool displaying anatomic variations and diseases. Because paranasal sinus development is a complex and long-lasting process, there are great structural variations between individuals. Several degrees and combinations of aplasias and hypoplasias have been reported; however, there is only one case of total paranasal sinus aplasia in the literature. Here, we present the second case of total paranasal sinus aplasia. Paranasal sinus development, functions of the paranasal sinuses, and the role of CT were evaluated.
A variety of paranasal sinus anomalies have been described in the literature but, to our knowledge, only one case of total paranasal sinus aplasia has been reported. 9 This article presents the second case of total paranasal sinus aplasia.
Case Report
The patient, a 57-year-old woman, presented to our clinic with the complaints of occasional nasal stuffiness and chronic frequent bilateral headache attacks concentrating around both ears and lasting a few days. Headache accompanied nausea, fullness of the face and ears, and hearing loss during attacks. Additionally, she described tiredness around upper jaw during chewing. Physical examination of the temporomandibular joint appeared normal. She said she had never caught a cold before.
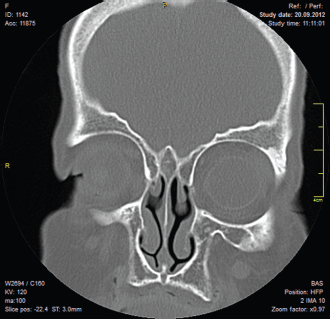
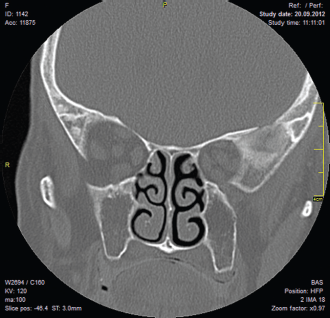
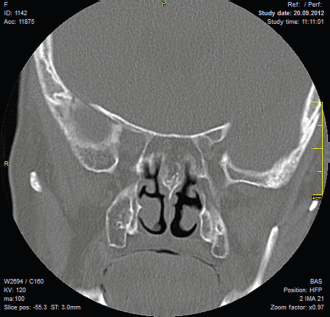
She had no previous history of recurrent sinusitis attacks, previous nasal surgery, or facial trauma. Physical examination did not reveal any pathological sign, and lateral nasal wall, septum, and nasal cavities were normal. Her facial appearance was normal. CT scans were obtained with 3-mm-slice thickness and 1-mm increment. The CT scans showed normal-appearing nasal septum and conchae. However, there was total lack of development of all paranasal sinuses (Figs. 1–14).

Coronal CT scan of the patient.

Coronal CT scan of the patient.
Coronal CT scan of the patient.

Coronal CT scan of the patient.

Coronal CT scan of the patient.

Coronal CT scan of the patient.
Coronal CT scan of the patient.
Coronal CT scan of the patient.
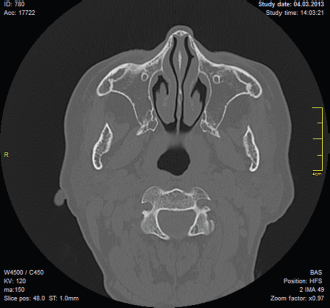
Axial CT scan of the patient.

Axial CT scan of the patient.

Axial CT scan of the patient.

Sagittal CT scan of the patient.

Sagittal CT scan of the patient.

Sagittal CT scan of the patient.
Discussion
Functional roles of paranasal sinuses continue to be elusive. 10 Some of the functions ascribed to these sinuses are as follows: they lighten the skull; assist in facial growth and architecture; produce nitric oxide gas; function as pillars for dispersal of masticatory forces; provide protection for the brain; provide thermal insulation for the central nervous system and sense organs; serve to increase surface area of the olfactory mucosa; provide even distribution of inspired air, which aids in olfaction; impart resonance to the voice; and serve as an adjunct in air conditioning of inspired air. 11
Although the development of paranasal sinuses begins in the 3rd week of gestation, their expansion continues after birth throughout early adulthood. 12 At birth rudimentary maxillary and ethmoid sinuses are present but sphenoid and frontal sinuses are undeveloped. The maxillary sinus extends laterally past the infraorbital canal by the age of 4 years and reaches the maxillary bone by the age of 9 years. At birth, ethmoid cells are more developed anteriorly and pneumatization progresses in a posterior direction. Their growth lasts until late puberty. Pneumatization of the sphenoidal sinuses can be detected as early as 2 years of age and they reach the final size by the age of 14 years. The last paranasal sinus undergoing major expansion is the frontal sinus. Its growth starts after 2 years of age and reaches its final size after puberty.
Paranasal sinuses present great structural variations. Aplasia of the sphenoidal sinus is extremely rare. Frontal sinus aplasia is present unilaterally in 15% and bilaterally in 5% of normal adults. 13 Maxillary sinus aplasia is extremely rare, whereas maxillary sinus hypoplasia is a well-known clinical entity. 14 Maxillary sinus hypoplasia is reported in 1.7–10.4% of patients with sinonasal symptoms.15,16
To the best of our knowledge, this is the second case report of total paranasal sinus aplasia in the English language literature. 9
When we are dealing with paranasal sinus diseases we must consider paranasal sinus aplasia and hypoplasia for several reasons. First, the prevalence of frontal and sphenoidal sinus aplasia or hypoplasia have been shown to be higher in patients with cystic fibrosis or primary ciliary dyskinesia. 8 So, in a patient with paranasal sinus hypoplasia and aplasia, we should consider and exclude primary ciliary dyskinesia and cystic fibrosis. Second, paranasal sinus aplasia and hypoplasia may lead to misdiagnosis of infections or mass lesions. 17 These patients may be treated for months with the diagnosis of chronic sinusitis if we rely only on the routine x rays. Although plain paranasal sinus radiography has low sensitivity and specificity in the diagnosis of rhinosinusitis, it is frequently preferred because of its low cost and significantly lower radiation exposure dose. In suspicious cases, CT should be performed. Some limited studies, such as three-slice CT, digital tomosynthesis was proposed with acceptable accuracy and lower radiation dose. However, standard CT scan remains the gold standard in revealing anatomic details.18,19 CT reveals excellent detailed anatomy of the paranasal sinuses.20–23 Third, paranasal sinus aeration should be considered during endoscopic sinus surgeries to avoid possible complications and to perform appropriate surgeries. Fourth, evaluation of the complaints of the patients with paranasal sinus aplasia and hypoplasia may enlighten us on the functions of the paranasal sinuses. We think that chronic recurrent headache and jaw tiredness on chewing may be related to total paranasal sinus aplasia. Her headache history is compatible with a migrainous type. We think paranasal sinus aplasia decreased the threshold of pain occurrence. She was devoid of the functions of the paranasal sinuses such as skull lightening, thermal insulation for central nervous system, and sense organs. Therefore, any irritating factor such as cold air, chemical irritants, stress, and anxiety easily triggers the headache. Her second complaint, masseter tiredness on chewing, points out another function of the paranasal sinuses, which is dispersal of masticatory forces on chewing.
The other total paranasal sinus aplasia patient reported by Celebi and friends had less specific complaints attributed to aplasia. 9 His major symptom was fullness of the face, which was also described by our patient. He did not have headache and masticatory problems. Fortunately, both patients were free of recurrent sinus infections.
Conclusion
Paranasal sinuses are subject to great structural variations. CT scan is the main tool to reveal the detailed structure of the paranasal sinuses. They may show great aeration differences ranging from normal to total aplasia. We have to be aware of any of these morphological alternatives to reach correct diagnoses and treatment of diseases. Patients with aplasia and hypoplasia may be evaluated to make clear the roles of the sinuses.