
Abstract
Resection of a juvenile nasopharyngeal angiofibroma (JNA) is challenging because of high intraoperative blood loss secondary to the tumor's well-developed vascularity. Endoscopic sinus and skull base surgeons commonly collaborate with neurointerventionalists to embolize these tumors before resection in an attempt to reduce the vascular supply and intraoperative bleeding. However, angioembolization can be associated with significant complications. Geometric alopecia from angioembolization of JNA has not been previously reported in the otolaryngologic literature. In this study, we discuss geometric alopecia from radiation exposure during preoperative angioembolization of a JNA.
Preoperative angiography and subsequent embolization of the vascular supply of JNAs are routinely performed for larger tumors to decrease intraoperative bleeding and the need for transfusions.4,5 Angioembolization can be associated with serious side effects and may lead to patient morbidity and mortality. 6 Nevertheless, complications related to radiation exposure during angioembolization are infrequently reported. Damage to the skin, hair, and subcutaneous tissues is a well-established complication of radiation therapy. Similar complications have been reported after fluoroscopic procedures; however, they are considered uncommon complications in this setting. 7 To our knowledge, this entity has not been previously reported in the otolaryngologic literature. Here, we present a rare case of alopecia after preoperative embolization of a large JNA. This report aims to increase the otolaryngologist's awareness of this rare complication of angioembolization. The protocol for this study was reviewed and approved by the Institutional Review Board of the University of Medicine and Dentistry of New Jersey-New Jersey Medical School, Newark, NJ.
Illustrative Case
A 13-year-old boy with a 3-month history of nasal obstruction was referred to our institution for evaluation and management of a right sinonasal mass after a biopsy was consistent with JNA. Computed tomography and magnetic resonance imaging showed a large 3.7 × 5 × 4.5-cm, primarily right-sided, nasopharyngeal lesion with extension into the right pterygopalatine fossa, infratemporal fossa, and bilateral sphenoid sinuses, as well as erosion of the anterior clivus and right pterygoid plates (Fig. 1, A, B, D, and E). Nasal endoscopic evaluation revealed a large mass obstructing the right nasopharynx with deviation of the posterior nasal septum to the left (Fig. 2 A).
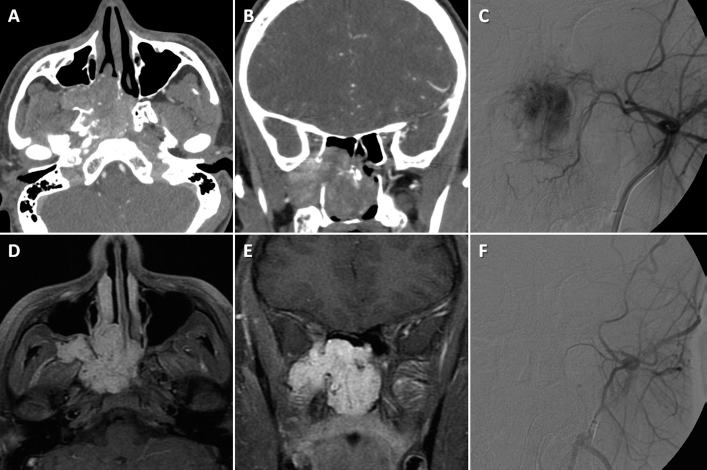
(A) Axial and (B) coronal, preoperative contrast-enhanced computed tomography (CT) scans of the paranasal sinuses show an expansile right nasopharyngeal mass with expansion of the pterygopalatine fossa and extension into the infratemporal fossa. (D) Axial and € coronal T1-weighted gadolinium-enhanced magnetic resonance imaging (MRI) show a hyperintense lesion with a few signal voids suggestive of a juvenile nasopharyngeal angiofibroma (JNA). (C) Preembolization and (F) postembolization angiograms show cessation of the tumor blush after embolization of the tumor's vascular supply.

(A) Thirty-degree nasal endoscopic examination revealed a right nasopharyngeal mass. (B and C) Intraoperative tumor resection. Postoperative (D) axial and (E) coronal computed tomography (CT) scans of the paranasal sinuses showed gross total tumor resection. (F) Photograph showing the geometric alopecia.
Preoperative six-vessel cerebral angiography showed internal and external carotid artery contributions to the tumor vasculature bilaterally, with extensive tumor blush on superselective catheterization of the internal maxillary arteries (IMA; Fig. 1 C). Embolization of the right IMA was performed with polyvinyl alcohol particles (Embosphere Microspheres; Merit Medical Systems, Inc., South Jordan, UT). The left IMA was subsequently embolized with N-Butyl Cyanoacrylate glue (TRUFILL Liquid Embolic System; Cordis Neurovascular, Inc., Miami Lakes, FL) with cessation of contrast extravasation (Fig. 1 F). No immediate postprocedural complications were documented. The patient underwent uneventful endoscopic resection of the tumor (Fig. 2, B and C). Gross total resection was confirmed by postoperative computed tomography scan (Fig. 2, D and E). He had an uncomplicated hospital and postoperative course.
At 6-week follow-up, the patient was noted to have a large, well-demarcated, semicircular segment of alopecia in the right occipitoparietal region (Fig. 2 F). Exclamation mark hairs were not found and pulltests were positive over the affected areas of alopecia. There was also no evidence of vascular compromise to the area. No other abnormalities of the scalp were noted within the affected region. Physical exam was otherwise unremarkable. A diagnosis of geometric alopecia was rendered and the patient's alopecia resolved after 6 months (Fig. 3). He remained stable without recurrence of the alopecia or JNA at 12 months.

Photograph showing repopulation of hair in the area of geometric alopecia at 6 months.
Discussion
Damage to the integumentary system is a well-known complication of direct, local radiation exposure to a region of the body, as with radiation therapy. Procedures that use fluoroscopic guidance (i.e., angiography and embolization) also expose patients to external radiation beams that allow for the guidance of interventional tools required to perform endovascular treatments. Integumentary reactions to radiation exposure have similarly been reported after fluoroscopic procedures; however they are considered uncommon complications in this setting. 7 Reactions range from mild skin changes that heal without intervention to life-threatening injuries that require immediate attention. Patients may experience associated pain, may be subjected to emotional distress, and can suffer from permanent disfigurement. 7
The differential diagnosis of alopecia in the setting of head and neck angiography includes alopecia areata, drug-induced alopecia, pressure-induced alopecia, and alopecia related to arterial occlusion. 8 The geometric nature of the alopecia in our case suggests that the affected area had prolonged radiation exposure.8,9 This is a form of radiation dermatitis, caused by the high sensitivity of the anagen follicles to radiation. This condition typically has a delayed onset and a temporary course, with spontaneous regrowth of hair up to several months after the insult.8–11 Permanent hair loss has also been reported. 10 Interestingly, the skin of the scalp is relatively insensitive for skin reactions (e.g., erythema and ulceration) but is more sensitive for hair loss compared with elsewhere in the body. 12 No therapy exists for radiation-induced alopecia. 8
Alopecia, like skin damage, is considered a deterministic effect of radiation exposure; a threshold exists above which the probability of damage increases rapidly. Thus, radiation time (proportional to radiation dose) should be minimized to prevent patients from experiencing radiation-induced complications. Exposure from previous interventions may have an additive effect. Thus, careful monitoring of exposure time (and dosage if possible) including dose fractionation (interval between exposures) is critical to reducing the risk of radiation-induced complications. 7 Digital subtraction angiography procedures for head and neck tumors can expose patients to doses as high as several grays (Gy) per minute. 7 A reported threshold for temporary epilation is 300–600 Gy and 700 Gy for permanent hair loss. 9 A recent study reports the use of direct puncture techniques versus the transarterial approach, which may lessen fluoroscopy time with similar efficacy and bleeding rates. 4
To our knowledge, no reports of this entity exist in the otolaryngologic literature to date. The otolaryngologist should be attentive to the possibility of epilation after angioembolization for a number of reasons. Although not a direct by-product of the otolaryngologic surgical resection of the tumor, preoperative counseling should include a discussion of the risk of temporary alopecia from angioembolization. An accurate history must be obtained including all previous radiation exposures, because many times, patients are not informed that fluoroscopic procedures entail radiation exposure. 7 The otolaryngologist must work closely with the neurointerventionalist to ensure that angiography time is minimized to prevent these outcomes. In fact, at our institution, only large JNAs with major bleeding anticipated are embolized before resection, as to prevent unnecessary irradiation to patients. Furthermore, skin manifestations generally present 1 month after angiographic procedures 7 and are likely to be noticed or mentioned at follow-up visits in an outpatient setting. Thus, the otolaryngologist should be prepared to enquire about, diagnose, and manage these side effects.
Conclusions
Preoperative JNA embolization for gross total tumor resection may result in radiation exposure-related consequences. Although alopecia may be a relatively benign complication of the fluoroscopic-guided procedures, changes in external appearance may have a psychosocial effect on patients and may be permanent. Otolaryngologists must be aware of this entity to adequately educate and inform their patients. Additionally, interventional radiologists should establish precautions to prevent these adverse effects.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article