
Abstract
A 48-year-old female patient with uncontrolled severe asthma was referred to our hospital for anti-IgE therapy. She was suffering with persistent wheezing and dyspnea after a severe asthma attack that had taken place 5 months previously. Her asthma had not been controlled with adequate asthma treatment, including budesonide at 320 μg + formoterol at 9 μg b.i.d. combination, montelukast at 10 mg/day, and oral steroids (30–40 mg/day of prednisolone), during this period. She was hospitalized for evaluation for anti-IgE therapy. Chest radiography revealed a left-sided hilar opacity. Fiberoptic bronchoscopy was performed and showed an endobronchial lesion obstructing the left lower bronchus lumen. Computed tomography also revealed a nodular lesion at the same location. The patient underwent left lower lobectomy and mediastinal lymph node dissection. Pathological examination concluded the diagnosis of typical carcinoid tumor. After surgery, her symptoms disappeared and she has had no recurrence. In conclusion, a diagnosis of severe asthma requires confirmation of asthma. Uncontrolled symptoms that linger despite aggressive therapy warrant evaluation to rule out other etiologies, such as a carcinoid tumor, before selecting new treatment options.
Case Presentation
Her vitals were stable with a heart rate of 76 bpm, a temperature of 36.5°C, blood pressure of 110/70 mmHg, and respiratory rate of 18/min on physical examination. Her examination was normal with the exception of decreased auscultation in the left lung. Her routine blood count was hematocrit, 38.2%; leukocyte, 9300; and erythrocyte sedimentation rate 13, mm/hr. Spirometry showed an obstructive pattern (forced expiratory volume in 1 second [FEV1], 2.20 L [82%]; forced vital capacity [FVC], 3.45 L [110%]; FEV1/FVC, 60%). We were unable to show spirometric reversibility but were able to learn that during a previous hospitalization at another clinic, she had had a reversible airway obstruction. (prebronchodilator FEV1, 1.70 L [64%]; postbronchodilator FEV1, 2.01 L [75%]; reversibility, 17%). Her skin-prick test was positive for house-dust mites. Total IgE level was 115 kU/L. All data about the patient seemed to indicate that she could be a candidate for anti-IgE therapy. Chest radiography revealed a left-sided hilar opacity. For further evaluation, computerized tomography was performed and showed a 15-mm nodular lesion located in the left lower lobe bronchus (Fig. 1). These radiological findings changed our management plan and diagnosis from asthma to a chest mass. A fiberoptic bronchoscopy was performed, which revealed an endobronchial lesion obstructing the left lower bronchus lumen (Fig. 2). Biopsy was not performed because the lesion was highly vascularized and there was a risk of bleeding. Bronchial lavage fluid was removed from the left bronchus. Cytological examination of the lavage fluid was normal. The patient was transferred to the thoracic surgery ward for surgical treatment. She underwent left lower lobectomy and mediastinal lymph node dissection.
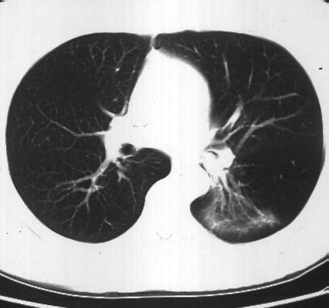
Thorax CT scan of the patient.

Bronchoscopic imaging of the carcinoid tumor.
Histopathological evaluation revealed an intrabronchial tumor, made up of monotonous cells with oval or round, finely granular nuclei and eosinophilic cytoplasm. No mitotic figures or necrosis was detected. The stroma was vascular and scant. Focal tumoral invasion of the lung parenchyma through the bronchial wall was also noted. Immunohistochemical staining indicated epithelial and neuroendocrine differentiation of the tumor cells with cytoplasmic positivity of pancytokeratin, chromogranin A, synaptophysin, and CD56. These findings established the diagnosis of a typical carcinoid (TC) tumor (Figs. 3 and 4). The dissected peribronchial and regional lymph nodes showed no metastasis.

The tumor made up of uniform polygonal cells with finely granular chromatin in round nuclei and moderate amount of eosinophilic cytoplasm. There were no nuclear atypia, mitosis and necrosis, H&Ex400.

The cytoplasmic positivity of chromogranin-A in tumor cells, Chromogranin-Ax400.
After surgical resection, she was asymptomatic with budesonide at 160 jug + formoterol at 4.5 jug combination therapy and had a better pulmonary function (FEV1, 2.53 L [95%], FVC, 4.29 L [138%]; FEV1/FVC, 59%). Eight months after the operation, she had another asthma attack. She was hospitalized for asthma treatment and further evaluation of recurrent tumor. There was the presence of reversible airway obstruction, particularly in the small airways, on spirometric evaluation (FEV1, 2.24 L [85%] with 10% reversibility and forced expiratory flow at 25–75%, 1.63 L [49%] with 17% reversibility). Computerized tomography of the thorax, abdomen, and pelvis revealed no pathological finding. Bronchoscopy was performed and cytological examination of the lavage fluid result was normal. She had no recurrence for 2 years and her asthma is presently well controlled.
Discussion
Today, achieving asthma control is indicated as the main goal of asthma management by international guidelines. Although most asthma patients can be treated and controlled with inhaled steroids, some patients remain uncontrolled despite adequate asthma therapy. In our country, nearly one-half of patients with asthma were found uncontrolled in a multicenter survey. 1 A systematic review should be conducted during the management of uncontrolled asthmatic patients, and it is imperative that this include first reconfirming that a diagnosis of asthma is appropriate and then evaluating for other coexisting diseases that may influence one's asthma control. Here, we report a case of uncontrolled asthma that was, after further evaluation, revealed to be a carcinoid tumor.
Pulmonary carcinoid tumors are the most frequently encountered benign tumors of the tracheobronchial tree and constitute 2–5% of all lung can-cers.2,3 TCs and atypical carcinoids (ACs) are subgroups of neuroendocrine tumors that are determined as low-grade and intermediate-grade tumors according to biological aggressiveness, respectively. TCs account for 90% of all carcinoids and 80% show up in a peripheral location. 4 Although TCs are low-grade tumors, regional lymph node metastasis can be seen in 10–23% of cases; this rate, however, is 40–50% for ACs. 5 This accounts for the higher 5-year survival rates seen in TCs when compared with ACs.5–7
The most common symptoms of pulmonary carcinoid tumors are hemoptysis (caused by high vascularization), lower respiratory tract infections, cough, wheezing, and shortness of breath.8,9 Some patients may be asymptomatic. There is usually a time gap from the onset of symptoms until diagnosis, and patients are often misdiagnosed with asthma.6,10–13 There are a limited number of cases diagnosed as carcinoid tumor who had also received a true diagnosis of coexisting asthma. The patient we present here had already received a diagnosis of asthma proven by reversible bronchial obstruction, and it was for this reason that her symptoms of dyspnea and wheezing were first attributed to asthma. The differential diagnosis was expanded after her poor response to standard therapy; thus, it is not surprising that a further treatment choice of anti-IgE was considered for this patient.
Anti-IgE (omalizumab) is an approved treatment for patients with severe asthma that acts on decreasing serum IgE levels. Several published studies have documented the effectiveness of this molecule in effectively treating asthma. We have been prescribing anti-IgE therapy in our tertiary clinic since 2006. In light of our experience, we believe that several factors impact a good response to anti-IgE treatment. First, proper determination of the correct indications for medicine use is vital, closely followed by the proper selection of patients. The most important issue, in our opinion, in achieving this is confirming diagnosis and excluding comorbid diseases. Therefore, the patient described in this study was evaluated accordingly. Clinical symptoms and reversible airway obstruction in spirometry led us to believe her asthma diagnosis was valid initially even though another disease state did in fact exist. Also, because an asthma attack occurred 8 months after the surgery we were convinced that she did have real asthma, retrospectively. In the literature, the associated factors with worsening asthma control included poor adherence, rhinitis, gastroesophageal reflux disease, nasal polyps, vocal cord dysfunction, bronchiectasis, allergic bronchopulmonary aspergillosis, Churg-Strauss syndrome, drugs, airway malignancy, respiratory tract infections, and thyrotoxicosis.14–16 Our patient had already been evaluated for upper airway disease and gastroesophageal reflux disease by an ear-nose-throat physician and a gastroenterologist, respectively, and no pathology was determined at the first hospital to which she was admitted. During the hospitalization period, she was adherent to her asthma therapy. There were no other diagnostic criteria supporting allergic bronchopulmonary aspergillosis and Churg-Strauss syndrome. She was not taking any kind of medication (e.g., β-blocker, angiotensin-converting enzyme inhibitor, or nonsteroidal anti-inflammatory drug) that could exacerbate asthma. No clinical or laboratory finding of thyrotoxicosis or infection was present. We decided to make the differential diagnosis of a possible chest mass based on the left hilar opacity observable from chest radiography. In the light of computerized tomography, we performed a fiberoptic bronchoscopy and made the diagnosis of carcinoid tumor by bronchoscopic biopsy specimen.
Pulmonary carcinoids are generally located centrally in the main or lobar bronchi.17,18 Available specimens for pathological examination can generally be provided from fiberoptic bronchoscopy and histopathological diagnosis is easily achieved. In this case, the tumor was located in the left lower bronchus and could easily be seen during fiberoptic bronchoscopic examination. A biopsy specimen was not taken because carcinoid tumors are highly vascularized and there is a risk for hemorrhage in nearly one-fourth of cases.4,19 Furthermore, some authors advise against performing biopsies with flexible bronchoscopes. 20
Because treatment options differ according to tumor type, determining a tumor's histological type is important. In this case, the microscopic, morphological, and immunohistochemical features were characteristic for pulmonary carcinoid tumor. Pulmonary carcinoid tumors are divided into low-grade TCs and intermediate-grade ACs based on histopathological criteria. A typical pulmonary carcinoid tumor shows no focal necrosis and rare mitosis whereas an atypical pulmonary carcinoid tumor shows either focal necrosis or mitosis numbering between 2 and 10/mm2.21,22 In our case, the absence of mitosis and necrosis with the characteristic morphological and immunohistochemical features were compatible with a low-grade typical pulmonary carcinoid tumor.
Surgery is the main choice for treatment of carcinoid tumors. In general, radical excision with detailed lymph node sampling is recommended. 8 In patients with a centrally located typical pulmonary carcinoid, bronchial sleeve resection or sleeve lobectomy is preferred. Despite its having a low recurrence rate, peripherally located TCs should be thought of as low-malignant tumors and resected anatomically. A more extensive surgical approach is recommended in AC tumors. 18 Our patient was treated with left lower lobectomy and mediastinal lymph node dissection and had experienced no recurrence for 30 months.
This case is an example of the importance of making a good differential diagnosis and confirming a diagnosis of asthma. Asthma unresponsive to treatment should alert clinicians to the possibility of differential diagnoses of other reasons for airway obstruction. Consequently, we strongly support the view that diagnosis confirmation is essential in patients with uncontrolled asthma before trying more expensive treatments.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article